1784
Automatic Assessment of UTE MRI High Signal Volume in the Lung for Pediatric Patients with Cystic Fibrosis1Department of Electrical, Computer, and Biomedical Engineering, Toronto Metropolitan University, Toronto, ON, Canada, 2Department of Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4Department of Pediatrics, University of Toronto, Toronto, ON, Canada, 5Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada, 6Department of Physics, Toronto Metropolitan University, Toronto, ON, Canada
Synopsis
Keywords: Quantitative Imaging, Lung, UTE, CF, Pediatric
High signal volume (MR-HSV) obtained by Ultrashort Echo-Time (UTE) MRI has been shown to be associated with disease severity in adults with CF, but has yet to be investigated in pediatric CF patients. In this study, MR-HSV was automatically extracted from UTE MRI of pediatric CF (n=9) and healthy (n=4) participants. MR-HSV measurements were significantly increased in CF compared to health, and increased MR-HSV correlated with decreased lung function (ie. FEV1pp, FEV1/FVC). The findings in this work confirm that MR-HSV measurement is feasible in pediatric participants and may reflect disease severity associated with airway/parenchyma signal intensity abnormalities in CF.Introduction
Cystic Fibrosis (CF) lung disease is characterized by mucus plugging and inflammation that leads to permanent structural damage and eventual respiratory failure1. While computed tomography (CT) is the clinical standard for long-term monitoring of CF, it exposes patients to ionizing radiation, and in the context of repeated imaging is not ideal. However, recent studies indicate that abnormally high signal intensity regions are apparent in ultra-short echo time (UTE) magnetic resonance imaging (MRI) in CF patients. In particular, UTE MR high signal volume (MR-HSV) was shown to correlate with visual scoring, pulmonary function, and CT high attenuation areas in adults with CF2. To our knowledge, MR-HSV has not been investigated in pediatric CF patients. We hypothesize that in pediatric CF patients, regions of mucus plugging/inflammation appear as MR-HSV. Therefore, our objective was to develop an automated method to extract UTE MR-HSV and determine if MR-HSV differentiates pediatric CF and healthy participants and is correlated to pulmonary function.Methods
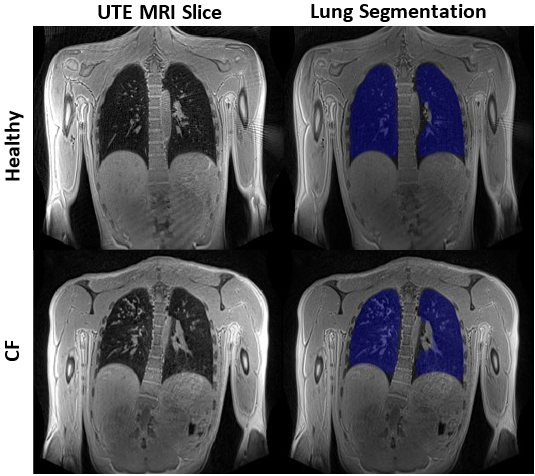
Demographics, pulmonary function, and MRI of pediatric CF participants and age-matched healthy controls were collected at The Hospital for Sick Children (Toronto, Canada). UTE lung images were acquired during free-breathing at 3T using a stack-of-spirals volumetric interpolated breath-hold examination (UTE Spiral VIBE) research application sequence3,4: TR=4.50ms, TE=0.05ms, flip angle=5°, FOV=480x480mm2, resolution=1.5x1.5x1.5mm3. To avoid breathing artefacts, prospective gating was used based on the respiratory signal, which was estimated during scanning from navigator acquisitions that were played out throughout the acquisition. MR images containing significant streaking artefacts (>20% of lung slices) were removed. The lungs were automatically segmented using a deep learning model5 to generate the MRI lung volume (Figure 1). For automatic post-processing, segmentation artefacts were eliminated by removing any excess connected components, followed by applying morphological dilation and erosion. The voxels inside the lung were extracted by applying the segmentation mask, and MR signal values were normalized to [0,1] by rescaling to the 0.1-percentile and 99.9-percentile. MR-HSV was defined as the volume greater than mode+k*standard deviation (SD), normalized by the MRI lung volume2. To determine the optimal threshold for MR-HSV, various values were tested (k=1,2,3,4). The Mann–Whitney U test was used to compare participant demographics, pulmonary function, and MRI measurements between CF and healthy participants. The correlation between MR-HSV and pulmonary function (forced expiratory volume in 1s (FEV1), and FEV1/forced vital capacity (FEV1/FVC)) was investigated using Spearman correlations.Results
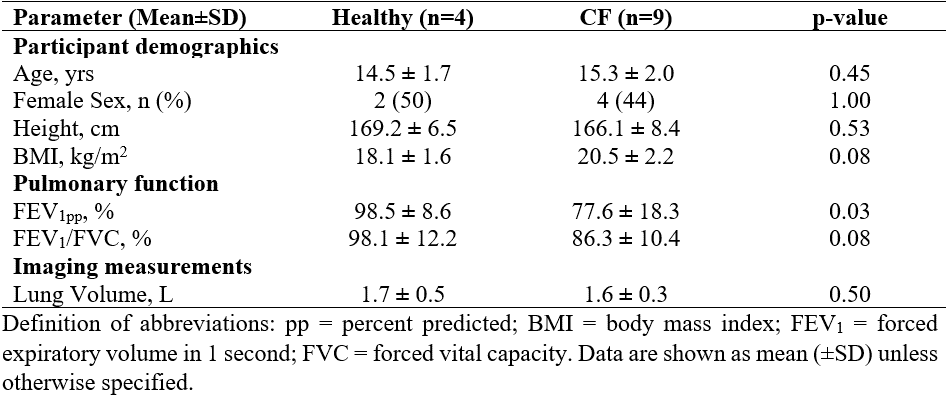
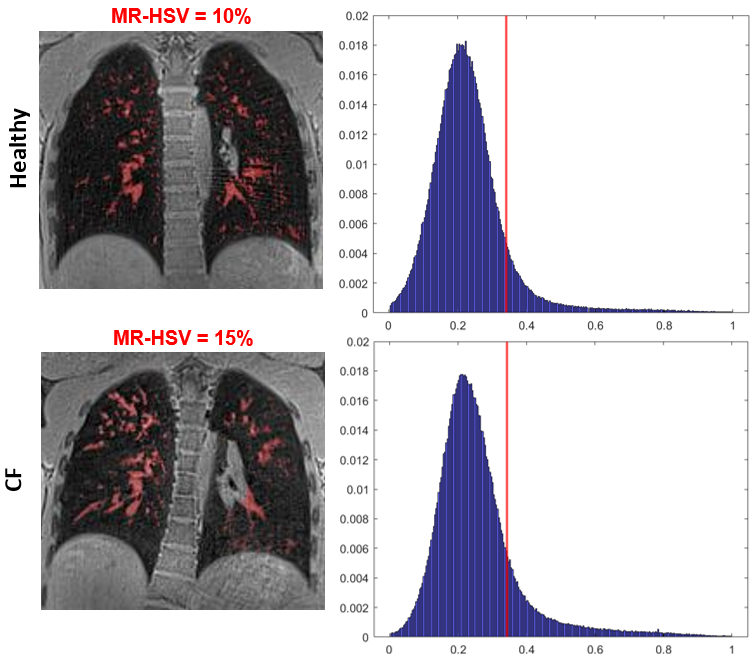
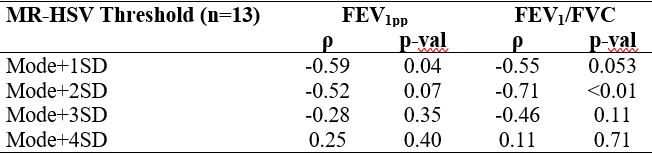
A total of 18 (n=11 CF, n=7 healthy) participants were evaluated. However, 5 participants were removed due to streaking artefacts possibly associated with uncorrected cardiac or bulk motion; 13 participants remained (n=9 CF, n=4 healthy). There were no differences between the groups for age, sex, or MRI lung volume (p>0.05) (Table 1). Compared to healthy controls, CF participants had reduced FEV1pp (p<0.05), but not FEV1/FVC. For representative CF and healthy participants, Figure 2 shows HSV regions highlighted in red, along with their corresponding histograms and mode+1SD threshold. Table 2 shows the comparison of various thresholds for quantifying MR-HSV in the healthy and CF participants. For MR-HSV generated with mode+1SD and mode+2SD thresholds, there were significant differences between healthy and CF participants (p<0.05). The MR-HSV with mode+1SD threshold had the strongest correlation with FEV1pp (ρ=-0.59, p=0.04), while MR-HSV with mode+2SD had the strongest correlation with FEV1/FVC (ρ=-0.71, p<0.01) (Table 3).Discussion
This study confirms that quantifying HSV with UTE Spiral VIBE MRI is feasible in most pediatric participants. It was observed that there was a greater extent of MR-HSV in CF compared to healthy participants, and an increase in MR-HSV was significantly correlated with worse lung function. In CF patients, these high signal intensity regions presumably reflect abnormalities related to disease, potentially mucus plugging and inflammation. In the future, these findings may be confirmed by expert reader evaluation of morphology hallmarks associated with CF, and/or by comparison with CT imaging. Previous work by Benlala et al2 quantified MR-HSV using pointwise encoding time reduction with a radial acquisition (PETRA) UTE MRI in adults with CF, and also showed significant correlations for MR-HSV with FEV1pp. However, there were differences in the optimal threshold, age of the participants (adults vs. pediatric), and pulse sequence and acquisition parameters. As such, more research is required to determine the optimal threshold/sequence for quantifying MR-HSV on UTE MRI in pediatric CF patients. Additionally, MR-HSV does not discriminate between high signal intensity originating from the lung parenchyma or the pulmonary vasculature. Further development of methods is required to potentially separate the pulmonary vasculature structures. Furthermore, although the difference for MR-HSV between CF and healthy participants was significant, the magnitude was relatively small, and likely explained by the mild CF cohort, and small numbers in this study. Despite this, these results show that even in mild pediatric CF disease, an increase in MR-HSV can be detected.Conclusion
In this proof-of-principle study with a small number of pediatric CF and healthy participants, we demonstrate that MR-HSV can be automatically extracted from UTE Spiral VIBE MRI. MR-HSV was significantly elevated in CF patients compared to healthy participants, and was significantly negatively correlated with lung function. These findings motivate further exploration of MR-HSV as a quantitative biomarker for the evaluation of CF disease severity using larger pediatric cohorts.Acknowledgements
We acknowledge research funding from the Canadian Institutes of Health Research (CIHR). D. Genkin acknowledges salary support from the Natural Sciences and Engineering Research Council (NSERC). M. Kirby acknowledges support from NSERC and the Canada Research Chair Program (Tier II). The authors thank Jacky Au, Sharon Braganza, Daniel Li, Aviva West, Ruth Weiss, Tammy Rayner, and Leslie Burns for assistance with imaging experiments.References
1. Turcios NL. Cystic Fibrosis Lung Disease: An Overview. Respir Care. 2020 Feb;65(2):233-251. doi: 10.4187/respcare.06697. Epub 2019 Nov 26. PMID: 31772069.
2. Benlala I, Point S, Leung C, et al. Volumetric quantification of lung MR signal intensities using ultrashort TE as an automated score in cystic fibrosis. Eur Radiol. 2020 Oct;30(10):5479-5488. doi: 10.1007/s00330-020-06910-w. Epub 2020 May 15. PMID: 32415586.
3. Zanette B, Schrauben EM, Munidasa S, et al. Clinical Feasibility of Structural and Functional MRI in Free-Breathing Neonates and Infants. J Magn Reson Imaging. 2022;55: 1696-1707. doi: 10.1002/jmri.28165
4. Mugler J, Meyer C, Pfeuffer J, et al. Accelerated Stack-of-Spirals Breath-hold UTE Lung Imaging. Proc. Intl. Soc. Mag. Reson. Med. 2017;45:4904.
5. Weng AM, Heidenreich JF, Metz C, et al. Deep learning-based segmentation of the lung in MR-images acquired by a stack-of-spirals trajectory at ultra-short echo-times. BMC Med Imaging. 2021 May 8;21(1):79. doi: 10.1186/s12880-021-00608-1. PMID: 33964892; PMCID: PMC8106126.
Figures