1726
Elevated Magnetic Susceptibility Suggests Distinct Neurodegenerative Pathology in World Trade Center First Responders1Department of Biomedical Engineering, Stony Brook University, Stony Brook, NY, United States, 2Department of Radiology, Stony Brook Medicine, Stony Brook, NY, United States, 3Program in Public Health and Department of Family, Population, and Preventative Medicine, Stony Brook Medicine, Stony Brook, NY, United States, 4Department of Medicine, Stony Brook Medicine, Stony Brook, NY, United States
Synopsis
Keywords: Neurodegeneration, Degenerative
Mounting evidence has shown that first responders to the 9/11 terrorist attack on the World Trade Center(WTC) are developing early-onset dementia but the underlying pathology driving this remains to be understood. Our team assessed the relationship between cognitive impairment and susceptibility differences in the brains of responders for the first time using quantitative susceptibility mapping(QSM). While research on Alzheimer’s disease has reported changes in QSM across several regions, we found elevated susceptibility located in the amygdala of responders with CI. Our findings bolster evidence suggesting that WTC responders are experiencing unique pathology which could point to a novel neurodegenerative disease.Introduction
The collapse of the World Trade Center (WTC) created dust clouds that deposited a myriad of neurotoxins and heavy metals onto sites where responders were actively searching for survivors from the terrorist attacks of 9/11/20011,2. Toxic dust was ingested by responders during all operations3,4 and now, at mid-life, the most severely exposed responders are experiencing high levels of cognitive impairment without the types of pathology that normally drive cognitive decline5.Quantitative susceptibility mapping (QSM) has become a popular tool for the evaluation of paramagnetic and diamagnetic material accumulation6-9 and changes have been identified across neurodegenerative diseases including Alzheimer’s and Parkinson’s diseases10. While recent evidence has emerged connecting brain iron dysregulation and cognitive function in healthy subjects11, studies investigating QSM following severe exposure to inhaled ferrous dust but prior to the onset of severe neurodegeneration have had inconsistent findings10,12,13. As such, investigations are still working to reliably identify regions expected to change in parallel with cognitive impairment.
In this study, we aimed to evaluate whether increases in magnetic susceptibility, as measured by QSM, are higher in responders with cognitive impairment (CI) as opposed to cognitively unimpaired (CU) responders.
Methods
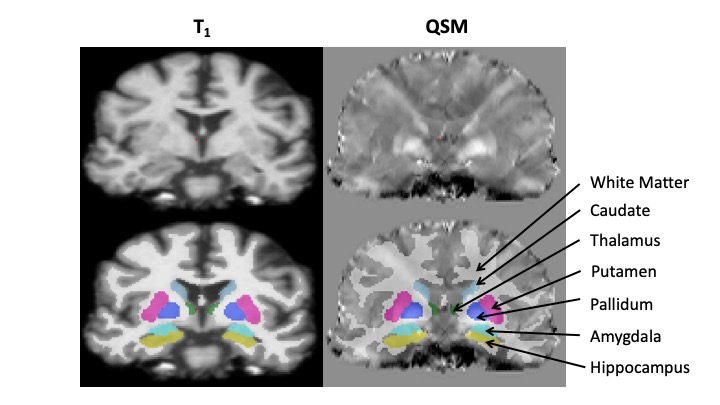
In total, 19 responders (14 male/5 female) with mean ages of 55.57 ± 4.77 years and 57.40 ± 6.19 years (p=0.50), were recruited for MRI imaging. Cognitive impairment was diagnosed following NIA-AA research guidelines and ranges in severity from mild cognitive impairment to mild dementia of the Alzheimer’s type 14,15. QSM images were acquired using multi-echo gradient echo sequences (8 echos, TEs = 6.2, 12.4, 18.6, 24.8, 31.2, 37.2, 43.4, 47.6ms, TR=71ms, in-plane resolution = 1x1mm2, slice thickness = 2mm, flip angle = 15), T1 weighted images (T1w) were also acquired using MPRAGE (TE/TR/TI = 3.24/2300/900 ms, voxel size = 0.87x0.87x0.87mm3, flip angle = 9).QSM maps were generated using morphology-enabled dipole inversion9 with nonlinear formulation to measure the susceptibility levels of material in the brain. After data collection, multi-echo phase datasets were prepared for QSM processing via nonlinear fitting complex echoes for field map estimation8, spatial unwrapping16, and background field removal17. Following contrast generation, T1w and QSM maps were registered together using the FMRIB Software Library FLIRT tool by linear18,19 then deformable registration techniques for regional analysis. Regions for statistical analysis were based on commonly reported areas in the QSM literature which relate to cognitive deficits10 and shown in Figure 1.
Results
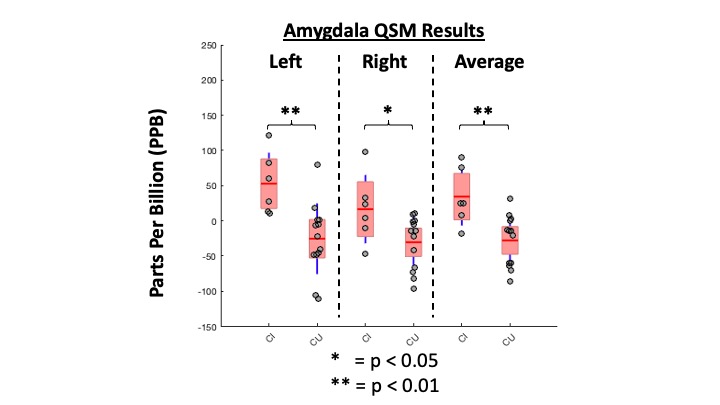
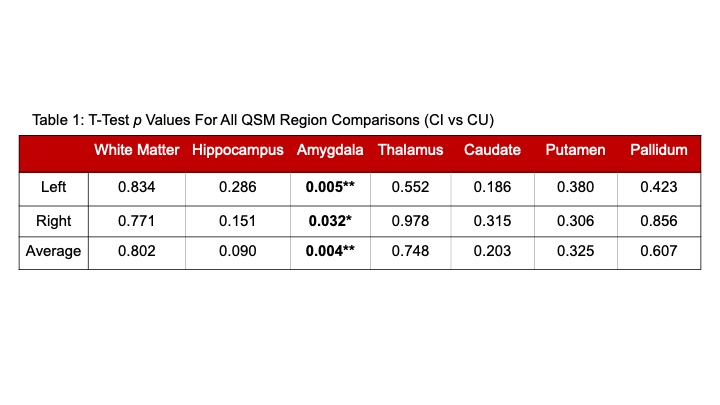
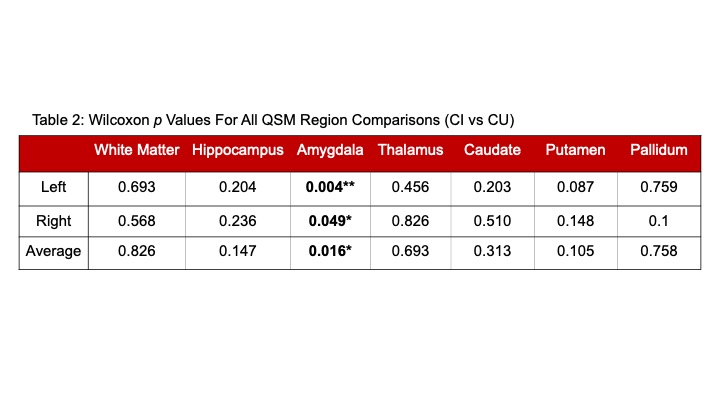
A chi-square test for cognition status resulted in no significant difference observed in the number of males or females reporting healthy cognition relative to cognitively impaired subjects (p=0.111). Figure 1 shows the QSM map obtained from a representative subject. Table 1 summarizes the statistical test results for seven regions commonly reported in the literature. This is followed by non-parametric analysis shown in Table 2 given the limited sample size. Among the regions, the amygdala reflected significantly elevated QSM values in CI as compared to CU responders in the left (p=0.005), right (p=0.032), and averaged regions (0.004). Figure 2 shows a box plot of amygdala QSM values for all subjects; non-parametric analyses revealed similar findings. Whereas other regions were not found to be significantly different between CI and CU.Discussion
Studies investigating changes in Alzheimer’s disease have reported consistency in QSM elevation in structures such as the amygdala, caudate, and putamen10. Our results reveal an intriguing signature of significantly elevated QSM but only for the amygdala bilaterally in responders with CI. This result is unique and may support work in this cohort suggesting the potential for unique pathology in a population with a high risk of neurodegenerative stress that has been linked to lengthy exposures at the World Trade Center. One limitation of this study comes from its limited sample size. Further work with a larger sample size paired with other imaging metrics to target pathologies, such as measures of neuroinflammation, could contextualize sources of these findings.Conclusion
Results demonstrate the potential presence of iron deposition might be at play in WTC responders suffering from cognitive impairment. These results may reflect the potential for toxic metal deposition and may also be indicate the hallmark of a unique pathology inconsistent with conventional neurodegeneration.Acknowledgements
The authors would like to thank the generous support for this work via the following funding sources: (R01 AG049953) and (R01 AG067590).References
1. Landrigan, P. J. et al. Health and environmental consequences of the world trade center disaster. Environmental health perspectives 112, 731-739 (2004).
2. Lioy, P. J. et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ Health Perspect 110, 703-714 (2002).
3. Clouston, S. A. P. et al. Cognitive impairment and World Trade Centre-related exposures. Nature Reviews Neurology (2021).
4. Galea, S. et al. Psychological sequelae of the September 11 terrorist attacks in New York City. N Engl J Med 346, 982-987 (2002).
5. Clouston, S. A. P. et al. Incidence of mild cognitive impairment in World Trade Center responders: Long-term consequences of re-experiencing the events on 9/11/2001. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring 11, 628-636 (2019).
6. de Rochefort, L. et al. Quantitative susceptibility map reconstruction from MR phase data using bayesian regularization: validation and application to brain imaging. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 63, 194-206 (2010).
7. Liu, J. et al. Morphology enabled dipole inversion for quantitative susceptibility mapping using structural consistency between the magnitude image and the susceptibility map. Neuroimage 59, 2560-2568 (2012).
8. Liu, T. et al. Nonlinear formulation of the magnetic field to source relationship for robust quantitative susceptibility mapping. Magnetic resonance in medicine 69, 467-476 (2013).
9. Liu, Z., Spincemaille, P., Yao, Y., Zhang, Y. & Wang, Y. MEDI+ 0: morphology enabled dipole inversion with automatic uniform cerebrospinal fluid zero reference for quantitative susceptibility mapping. Magnetic resonance in medicine 79, 2795-2803 (2018).
10. Ravanfar, P. et al. Systematic review: quantitative susceptibility mapping (QSM) of brain iron profile in neurodegenerative diseases. Frontiers in neuroscience 15, 41 (2021).
11. Howard, C. M. et al. Cortical iron mediates age‐related decline in fluid cognition. Human brain mapping 43, 1047-1060 (2022).
12. van Bergen, J. M. et al. Colocalization of cerebral iron with Amyloid beta in Mild Cognitive Impairment. Sci Rep 6, 35514 (2016).
13. Hwang, E. J. et al. Texture analyses of quantitative susceptibility maps to differentiate Alzheimer's disease from cognitive normal and mild cognitive impairment. Med Phys 43, 4718 (2016).
14. Albert, M. S. et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7, 270-279 (2011).
15. McKhann, G. M. et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & dementia 7, 263-269 (2011).
16. Li, W., Wu, B. & Liu, C. Quantitative susceptibility mapping of human brain reflects spatial variation in tissue composition. Neuroimage 55, 1645-1656 (2011).
17. Schweser, F., Deistung, A., Lehr, B. W. & Reichenbach, J. R. Quantitative imaging of intrinsic magnetic tissue properties using MRI signal phase: an approach to in vivo brain iron metabolism? Neuroimage 54, 2789-2807 (2011).
18. Jenkinson, M., Bannister, P., Brady, M. & Smith, S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 17, 825-841 (2002).
19. Woolrich, M. W. et al. Bayesian analysis of neuroimaging data in FSL. Neuroimage 45, S173-S186 (2009).
Figures