1702
Breath-hold Whole Heart Coronary MRA with Parallel Imaging, Compressed Sensing and Deep Learning reconstruction
Mitsuharu Miyoshi1, Atsushi Nozaki1, Shigeo Okuda2, Masahiro Jinzaki2, and Tetsuya Wakayama1
1Global MR application and workflow, GE Healthcare Japan, Tokyo, Japan, 2Department of Radiology, Keio University School of Medicine, Tokyo, Japan
1Global MR application and workflow, GE Healthcare Japan, Tokyo, Japan, 2Department of Radiology, Keio University School of Medicine, Tokyo, Japan
Synopsis
Keywords: Heart, Cardiovascular, Coronary Artery
For Breath-hold Whole Heart Coronary MRA, we developed the combination of Parallel Imaging and Compressed Sensing to accelerate scan time and Deep Learning reconstruction to improve the image quality. With the combination of these techniques, we could obtain Coronary MRA with 1.8mm isotropic acquisition voxel size in a possible breath-hold scan time. Deep Learning recon effectively improved the SNR and image quality.
INTRODUCTION
Whole Heart Coronary MRA (WHCA) has been used to provide the additional information on coronary arteries in cardiac MRI. Long scan time, which often takes more than 10 minutes, is problematic for WHCA to ensure the image quality and makes it difficult to improve adoption rate of WHCA in cardiac MRI. In clinical practice, respiratory motion of the patient is sometimes non-periodic and unstable, which causes motion artifact in respiratory-triggered scan. Breath-hold acquisition can be expected to be a promising solution to address the current problems in WHCA. In this study, we developed the combination of Parallel Imaging (PI) and Compressed Sensing (CS) to accelerate scan time and Deep Learning (DL) recon 1 to improve the image quality and demonstrated the combination of these techniques can be used for Breath-hold WHCA.METHODS
A healthy subject was scanned on 3T scanner (SIGNA Pioneer, GE Healthcare, WI) under IRB approval and written informed consent. Before WHCA imaging, 2D CINE sequence was used to determine the optimal trigger delay and the acquisition window in cardiac cycle of the subject. For WHC MRA imaging, 3D Fast SPGR was used with CHESS, T2-prep and ECG cardiac gating. The scan parameters are as follows: FOV=32cm, Trigger Delay=450ms, Trigger Window=150ms, Flexible AIR coil. Three parameters, receiver band width (BW), ARC PI acceleration and CS acceleration were adjusted to achieve breath-hold scan and the following cases are compared.(Case 1) BW=62.5 kHz, TR=3.3ms, PI acceleration=3.0, CS acceleration=1.8, Scan time=27sec.
(Case 2) BW=125 kHz, TR=3.2ms, PI acceleration=3.0, CS acceleration=1.8, Scan time=20sec.
(Case 3) BW=125 kHz, TR=3.0ms, PI acceleration=4.0, CS acceleration=1.6, Scan time=19sec.
The data was acquired with 1.8mm isotropic resolution and reconstructed to 0.625 x 0.625 x 0.8mm resolution. To investigate the effect of DL Recon, the raw data was retrospectively processed with the conventional Reconstruction and DL Recon. A circle Region Of Interest (ROI) was placed on the Ascending Aorta near origin of RCA, and the aorta SNR was calculated from the following equation: aorta SNR = (ROI mean) / (ROI SD).
RESULTS
Figure 1 is the image of origin of RCA. Aorta signal was measured in this plane and aorta SNR also shown in Figure 1. RCA images of breath-hold WHCA are shown in figure 2. In case 1, scanning time was the longest (30 sec) but SNR was the best. In case 2, higher BW was used to shorten scanning time. SNR was reduced with higher BW, but SNR was recovered with DL. In case 2 and 3, balance between PI and CS was changed but SNR was similar. DL could improve SNR and sharpness in all cases.DISCUSSION
We could achieve breath-hold HWCA with scan time less than 30 seconds by the combination of PI and CS. In such acquisition with high acceleration, SNR and image quality are easily problematic, however DL recon could improve them effectively. By using high BW and DL reconstruction, we could achieve 20 seconds scan time. Higher BW could reduce the scanning time, but SNR was also reduced. DL reconstruction could recover the SNR of the higher BW images. SNR in case 2 with DL was higher than that in case 1 without DL. The balance between PI and CS were changed in case 2 and 3. Because acceleration factor was high enough in both cases, there was no significant difference of SNR and images. It is difficult for patients to hold breathing for 30 sec, and 20 second protocol can be used for clinical cases.CONCLUSION
Parallel Imaging and Compressed Sensing could accelerate scan time and Deep Learning reconstruction could improve the image quality. The combination of these techniques can be useful for Breath-hold Whole Heart Coronary MRA.Acknowledgements
No acknowledgement found.References
1. Lebel, R.M. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. August 2020, http://arxiv.org/abs/2008.06559Figures
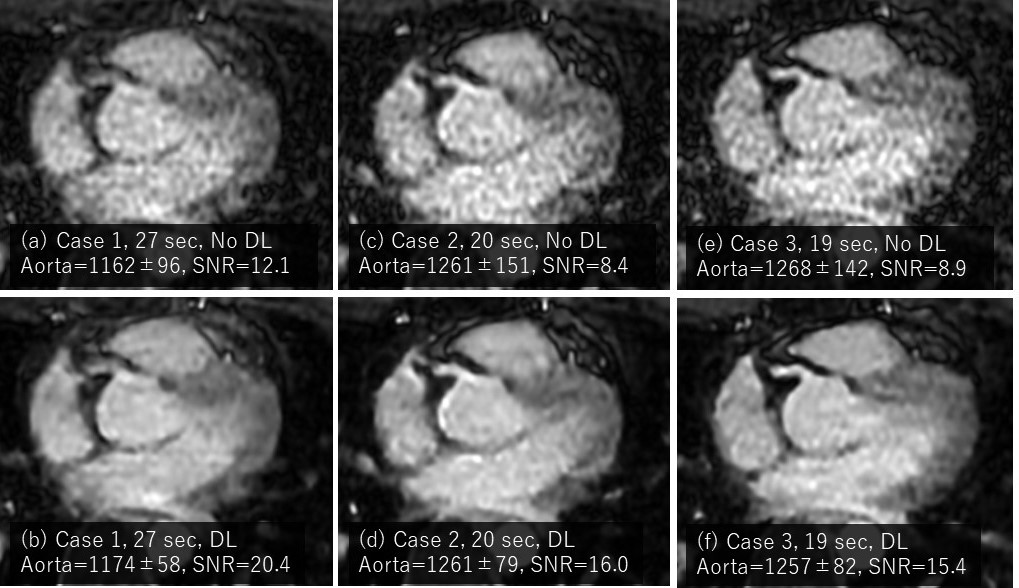
Figure
1: Breath-holding
WHCA image at Ascending Aorta near origin of RCA.
Left to right: (a,
b) Case 1, (c, d) Case 2, (e, f) Case 3. Top to bottom: DL off/on.
Measured aorta
Signal (mean, SD) and aorta SNR are
also described.
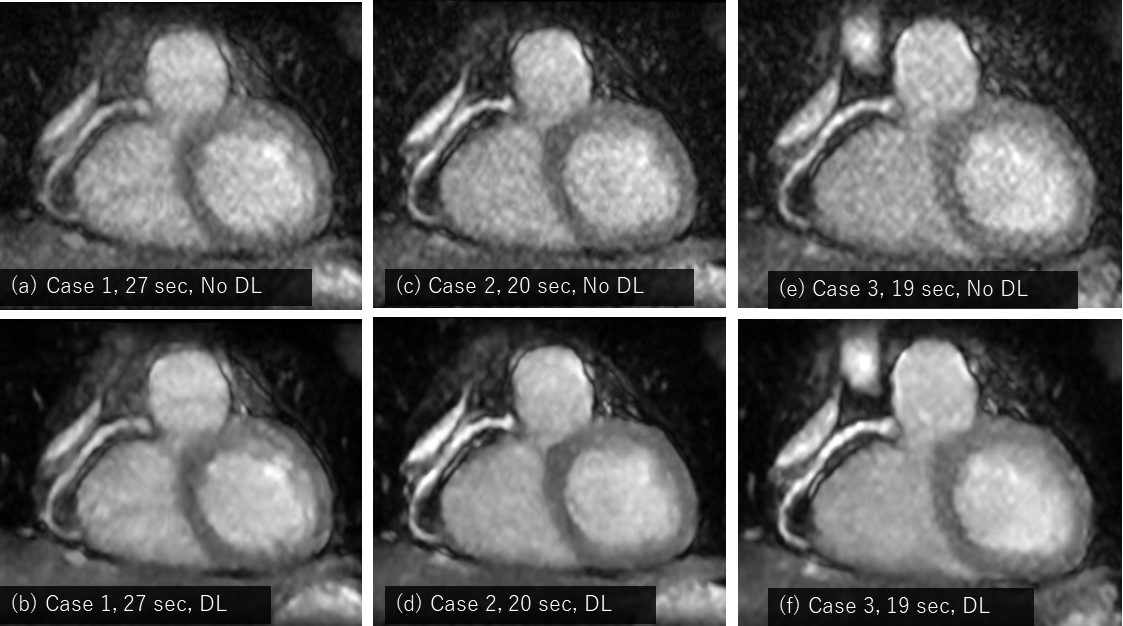
Figure
2: RCA
images of Breath-holding WHCA. 4.4mm MIP image.
Left to right: (a,
b) Case 1, (c, d) Case 2, (e, f) Case 3. Top to bottom: DL off/on.
DOI: https://doi.org/10.58530/2023/1702