1700
Analysis of baseline and cardiac function factors affecting the image quality of contrast-free 3.0T MR coronary angiography
Gang Zhang1, Wei Xing1, Zhiwei Shen2, Jianxiu Lian2, and Ke Jiang2
1The First Affiliated Hospital of Henan University of CM, Henan, China, 2Philips Healthcare, Beijing, China
1The First Affiliated Hospital of Henan University of CM, Henan, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Heart, Cardiovascular
Magnetic resonance coronary angiography (MRCA) imaging technology is still somewhat sophisticated, with numerous elements influencing image quality. This study found that for subjects with high BMI, high heart rate, and high systolic blood pressure, further optimization of imaging sequences and parameters is needed to explore individualized coronary MR imaging protocols.Introduction
Magnetic resonance coronary angiography (MRCA) imaging technology is still somewhat sophisticated, with numerous elements influencing image quality. Additionally, there is no globally acknowledged standard of practice for the examination, limiting its widespread clinical promotion. The purpose of this study is to investigate the important parameters influencing the quality of MRCA image using a large sample of clinical MRCA data, and to provide an objective and reliable basis for image quality control.Methods
One hundred seventy subjects who underwent whole-heart coronary MR imaging were included. A 3.0T MRI and a 32-channel dS Torso coil (Ingenia CX, Philips, The Netherlands) were utilized. A whole-heart coronary scan with the following parameters was performed using a 3D modified water-lipid separation (mDixon) sequence: TR/TE: shortest, The flip angle:10, FOV: 350 mm ×150 mm, the acquisition pixels: 1.5 mm ×1.5 mm, layer thickness: 1.5 mm, NSA: 1. The patient was positioned supine, and electrocardiographic monitoring electrodes were connected to the anterior chest wall to monitor the R-wave and activate cardiac gating. The respiratory gating was linked to the patient's supraumbilical position, and the patient was told to cooperate with the breathing command during the test.The mDixon raw images were imported into the ISP 9 Workstations (Philips, The Netherlands) post-processing workstation, and the CT view module was used to perform reconstruction such as surface reconstruction and maximum intensity projection of the coronary arteries to observe and evaluate the coronary artery structures from different angles.The quality of 3-branch coronary images was assessed using subjective scores, and four graded groups of excellent to moderate poor were classified. The differences between subjects in different groups in terms of baseline (age, sex, BMI), cardiac function (heart rate, systolic blood pressure, diastolic blood pressure, ejection fraction, and output per beat) were analyzed, and their correlation with image quality scores was explored.
Results
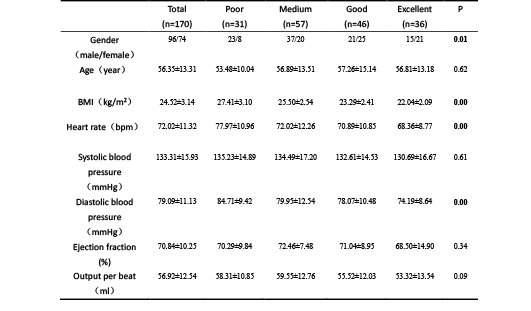
BMI, heart rate, and systolic blood pressure were statistically different between different MR coronary imaging quality groups (P < 0.05) and correlated with image quality scores, where BMI and heart rate were negatively correlated with image quality, while gender, age, systolic blood pressure, diastolic blood pressure, ejection fraction, and output per beat, were not correlated with image quality scores (P > 0.05).Conclusion
This study found that for subjects with high BMI, high heart rate, and high systolic blood pressure, further optimization of imaging sequences and parameters is needed to explore individualized coronary MR imaging protocols.Acknowledgements
noneReferences
noneFigures
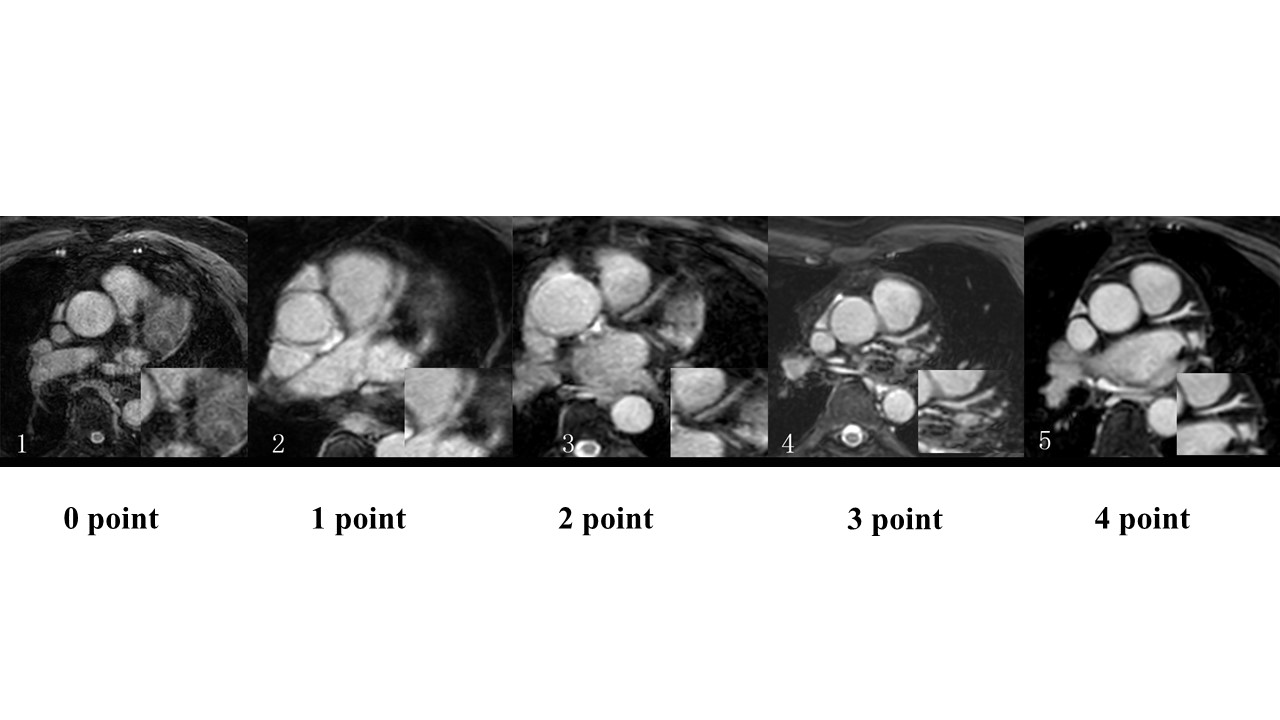
Figure 1 Image quality score of participants.
DOI: https://doi.org/10.58530/2023/1700