1695
Native MR angiography of the thorax using Compressed Sensing and 1-point Dixon at 3T: Comparison with standard fat suppression and 2-point Dixon
Michaela Schmidt1, Marcel Dominik Nickel1, and Daniel Giese1
1Siemens Healthcare, Erlangen, Germany
1Siemens Healthcare, Erlangen, Germany
Synopsis
Keywords: Vessels, Blood vessels
For increased vessel contrast a robust fat suppression of adjacent fat is desirable in MR angiography. While spectral fat suppression can be insufficient, fat separation based on 2-point Dixon requires the acquisition of a second echo. A 1-point Dixon approach based on opposed-phase imaging is presented here that allows to suppress fat dominated voxels effectively while keeping scan efficiency. The approach is evaluated in volunteers and compared to conventional approaches regarding image quality, artifacts, fat suppression and vessel diameter.Introduction
MR angiography (MRA) offers a safe, noninvasive, radiation- and iodinated contrast-free tool to assess vascular anatomies. Dixon fat-suppression promises to increase contrast by robustly suppressing fat adjacent to vessels but is time consuming [1]. Other fat suppression techniques such as SPectral Attenuated Inversion Recovery (SPAIR) or spectral fat suppression are faster but less robust. The aim of the present study was to develop a novel native, large field-of-view, high-resolution, free-breathing MRA technique using a modified 1-point Dixon and compare it with the typical 2-point Dixon and SPAIR in terms of scan time, image quality, fat suppression and vascular signal.Methods
For the prospective evaluation, we acquired an ECG triggered 3D GRE native MRA in the thorax and upper abdomen with T2-preparation, 11-fold Compressed Sensing (CS) acceleration. A cross-paired diaphragmatic navigator was used enabling scanning in free-breathing with a data acceptance window of ± 4.5 mm. The research sequence was acquired on a 3T clinical MRI scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany). The sequence was repeated 3 times keeping all scan parameters constant, only varying the fat suppression or separation technique. In Figure 1 relevant scan parameters are listed.Water-fat separation based on the Dixon method relies on the assumption that the signal at a voxel $$$x$$$ and echo time TE can be modeled as
$$S_e(x)=(W(x)+c_eF(x))\exp(i\Phi_e(x))$$
with water contribution $$$W(x)$$$, fat contribution $$$F(x)$$$, dephasing coefficient $$$c_e$$$ and phase error $$$\Phi_e(x)$$$. Crucial ingredient is a robust determination of the phase error $$$\Phi_e(x)$$$, which for 1-point Dixon relies on additional acquisitions or model assumptions [2,3]. Aiming at a robust application without dependence on additional input, no additional penalty in the noise propagation and mainly aiming to suppress fat signal in the provided images, the common approach is modified, and focus put on opposed echo times for which $$$c_e = -1$$$ (or in general real and negative). Existing phase unwrapping methods as used for 2-point Dixon can then be used to determine $$$\Phi_e(x)$$$ and phase corrected images with the contrast $$$W(x) - F(x)$$$ be obtained. For application on a scanner an existing 2-point Dixon algorithm was therefore modified and integrated into the scanner reconstruction pipeline to additionally provide $$$WmF(x) = max(W(x) - F(x),0)$$$ images. These only show water dominated image voxels and therefore efficiently suppress fat, albeit with a modified contrast for voxels that contain both components.
The 1-point Dixon results were compared to 2-point Dixon and SPAIR in 6 volunteers (age 51 ± 17, 2 female) regarding net scan times, artefact level (1: none, 2: minor, 2: major), fat suppression performance (1: optimal, 2: minor, 3: major regions not suppressed) as well as MR signal in ROIs drawn in the aortic lumen, the mediastinal adipose fat and the lung parenchyma. Additionally, the inner vessel diameter of the aorta at the level of pulmonary artery was compared.
Results
All 3 MRA scans in all 6 volunteers were successfully acquired and reconstructed inline on the scanner. Net scan times are displayed in Fig1 and were significantly (p<0.05) shorter for 1-point Dixon (4min2s ± 2min1s) and SPAIR (3min29s ± 1min15s) compared to 2-point Dixon (5min45s ± 3min12). 1-point Dixon and SPAIR showed minor artifacts in most volunteers with a score of (1.8 ± 0.4 and 1.8 ± 0.8) (Fig 2) while 2-point Dixon had a better score of 1.2 ± 0.4. SPAIR showed insufficient fat suppression (Fig1), especially of the mediastinal adipose fat, with a performance score of 2.5 ± 0.55 in all 6 volunteers while fat-water separation was optimal for all volunteers for 1-point and 2-point Dixon with a score of 1 ± 0. Signal values for ROIs in the aorta, lung parenchyma and mediastinal adipose fat as well as vessel diameter for the different methods and volunteers are displayed in Table 2. Evaluation of the AO diameter showed consistency between the three different acquisition types with no apparent outlier.Discussion
Conventional 1-point Dixon focuses on water-fat separation and relies on additional input or model assumptions. Furthermore, the echo time ideally corresponds to a perpendicular magnetization direction between water and fat components. Here a different approach was taken to achieve a robust, self-contained application relying on an antiparallel magnetization direction between water and fat components. While strictly speaking no longer a separation of components, it is still referred to 1-point Dixon in this work and aims at applications that focus on water and/or fat dominated voxels such as MRA. Especially in subjects with irregular breathing patterns the acceleration of scan time 1-point Dixon offers is crucial. SPAIR fat suppression in the thorax had problems to completely suppress the mediastinal adipose fat. Although 2-point Dixon had the best artifact score, 1-point Dixon and SPAIR showed only minor artifacts probably diagnostically not relevant. The presented results motivate further evaluation, ideally in a clinical setting. The approach is not limited to non-contrast MRA but may also be used to suppress fat in contrast enhanced MRA without the need of subtraction.Conclusion
A contrast free, large field-of-view, high-resolution, free-breathing MRA technique using 1-point Dixon showed promising results. While being as fast as simple fat suppression strategy like SPAIR it suppressed the fat robustly while maintaining high lumen signal and contrast to surrounding tissue.Acknowledgements
No acknowledgement found.References
1. Pennig, L., Wagner, A., Weiss, K. et al. Int J Cardiovasc Imaging 37, 315–329 (2021). https://doi.org/10.1007/s10554-020-01979-2 2.
2. Ma J, J. Magn. Reson. Imaging, 27: 881-890. https://doi.org/10.1002/jmri.21281 3.
3. Stinson EG et al., Magn Reson Med. 2018; 80: 1556-1567. https://doi.org/10.1002/mrm.27152
Figures
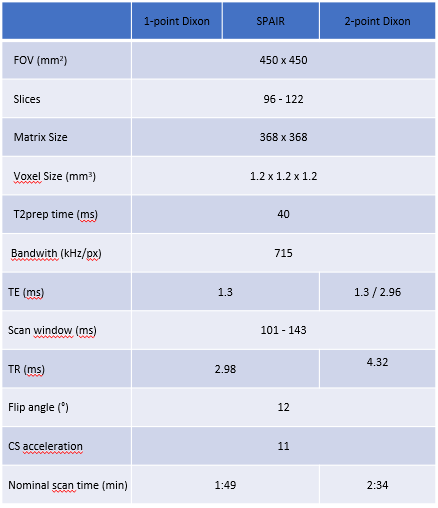
Scan
Parameters for 1-point Dixon, 2-point Dixon and SPAIR acquisitions.
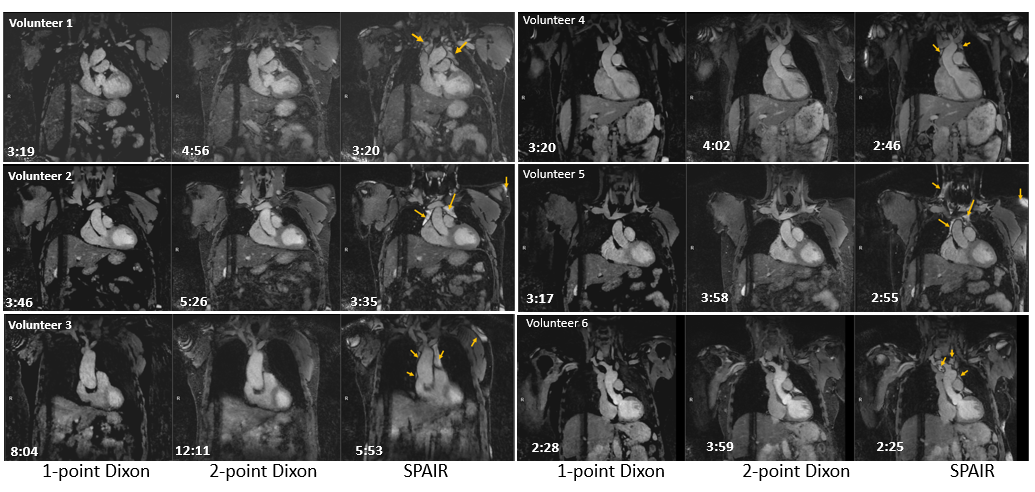
Coronal View of all 6 volunteers with all
3 techniques showing insufficient fat suppression, especially of the mediastinal
adipose
tissue
with
SPAIR fat suppression compared to both Dixon methods. The
individual scan time per Volunteer is displayed.
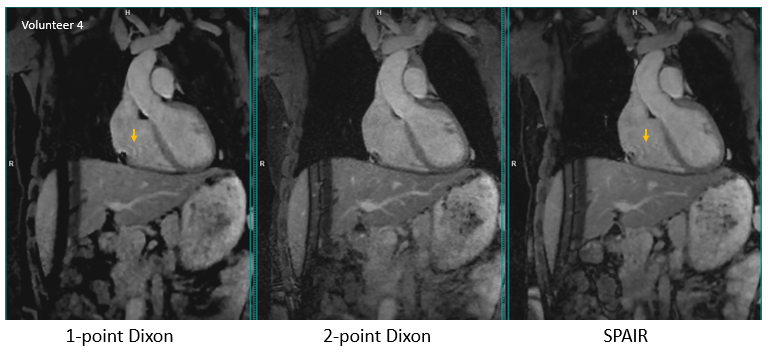
Example
for minor artifacts
in 1-point Dixon and SPAIR MRA
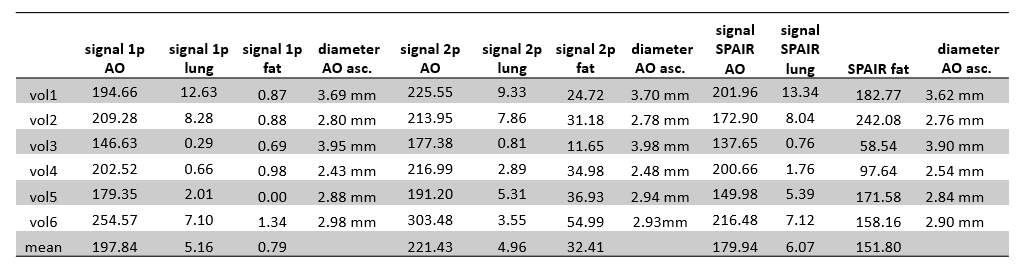
Individual and mean signal of the aorta, lung
parenchyma and mediastinal adipose fat and vessel diameter of the aorta ascendens for all 3 techniques.
DOI: https://doi.org/10.58530/2023/1695