1694
Efficiency of 3D ky-kz centric acquisition in whole heart coronary MRA (WHCA) using high resolution deep learning reconstruction (HR-DLR)1Department of Radiology, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan, 2Department of Radiology, Tohoku University Hospital, Sendai, Japan, 3Canon Medical Systems Corporation, Otawara, Japan, 4Department of Radiology, University of California, San Diego, La Jolla, CA, United States
Synopsis
Keywords: Heart, Cardiovascular, coronary artery
Whole heart coronary MRA (WHCA) using fast field echo (FFE) with 3D centric ky-kz trajectory was compared with conventional FFE on healthy subjects. The mean acquisition was almost within 5 minutes using a 30-mm threshold in real-time motion correction with a navigator echoes. High resolution deep learning reconstruction (HR-DLR) was also applied to improve the image quality.Introduction
In general, whole heart coronary MRA (WHCA) at 3T is acquired using fast field echo (FFE) and real-time motion correction (RMC) with a diaphragm (90-180 degrees) navigator-echo. A total scan time, therefore, depends on the efficacy of the subject’s diaphragm motion range, and it may often take a long acquisition time, which subsequently results in image quality degradation.1 We introduced the 3D centric ky-kz FFE acquisition and obtained 100% efficiency in a 30-mm navigator echo range, as compared to conventional acquisition with a 5-mm navigator echo range, resulting in an efficacy to increased efficiency of about 60%.2 Further reduction of scan time and improvement of image quality may be achieved with high-resolution deep learning reconstruction (HR-DLR). The purpose of this study was to develop high spatial and temporal resolution WHCA using centric FFE with applying high resolution HR-DLR and to compare with standard 3D FFE acquisition.Methods
The study was approved by our institutional review board. All MR imaging data were obtained with a clinical 3-T MR imager (Vantage Centurian 3T, Canon Medical Systems, Japan; gradient amplitude: 100 mT/m; slew rate: 200 mT/m/s) in 6 healthy subjects.The proposed and conventional WHCAs were imaged with ECG-triggered and navigator-gated under free breathing acquisition in axial sections covering the whole heart. Acquisition parameters of our proposed method are TR/TE=3.6/1.4 ms, 488 Hz bandwidth (BW), 198x256 matrix, 1.5-mm sections, 4 or 5 segments, acquisition window of 80~90 ms per segment, and a centric ky-kz 3D FFE using real time motion correction (RMC) band of 30 mm with 90-180 degrees navigator echo. Acquisition parameters of the conventional WHCA are TR/TE=5/1.9 ms, 326 Hz BW, 192x256 matrix, 1.5-mm sections, 4 or 5 segments, acquisition window of 120~130 ms per segment, and a sequential 3D FFE using RMC band of 5 mm.
High resolution deep learning reconstruction (HR-DLR): Figure 1 shows the HR-DLR algorism. The first process is a denoising block followed by the second process of up-sampling block. The acquired k-space data is transformed to a complex image with coil data combined and Fourier transform. The complex-valued image is input to the neural network (NN) for denoised images. Then, the denoised images are enlarged and zero-fill interpolation (ZIP) to provide higher resolution images.
Image evaluation: Each main coronary segment was divided into right coronary artery (RCA): #1, #2, and #3; left main trunk (LMT): #5; left anterior descending (LAD): #6 and #7; and left circumflex artery (LCx) #11 and #13, and their image quality was evaluated on per segment using a 3-point scale with non-diagnostic=0, fair or diagnostic=1 (some blurring and artifacts, but diagnostic), and superior in diagnostic=2 (less blur and no artifacts). Images were assessed using multiplanar reconstruction and thin section maximum intensity projection. Scan time of all acquisitions were measured. Statistical analysis was performed using paired t-tests for the comparison of variance. A p<0.05 is considered statistically significant.
Results
Figure 2 shows a scan time summary of both centric FFE and standard FFE. The RMC with a 30-mm threshold in the centric ky-kz acquisition allows a 100% efficiency of collecting all echo signals with the mean scan time of 4:44 minutes (within 5 minutes in all but one with bradycardia) in our volunteers with heartrate range of 50-70 bpm. On the other hand, the RMC with a 5-mm threshold in the regular acquisition gave a various scan time (12 to 20 minutes, mean scan time of 14:56 minutes) depending on the efficiency of RMC. Applying the HR-DLR process provides all centric ky-kz FFE images with less noise and higher resolution outcomes (Figure 3). Figure 4 shows representative cases of 3D centric ky-kz FFE with HR-DLR and conventional FFE. The 3D centric ky-kz FFE with HR-DLR offers high-resolution images without sacrificing signal intensity and contrast with a scan time of less than 5 minutes. The sharpness of vessel structures is obtained with HR-DLR.The centric FFE showed significantly higher image qualities in overall and RCA compared with standard FFE. Image qualities in LAD and LCx tended to be higher in centric FFE than in standard FFE but showed the no significant difference (Table 1).
The acquisition window of the centric ky-kz trajectory and standard was 80~90 and 120~130 ms, respectively. The shortening of entire scan time by using centric acquisition allows to apply a shorter acquisition window. Furthermore, the contrast-determined time of the centric order is filled at the center of k space. On the other hand, the contrast-determined time of the standard acquisition may be out at the off-center slice encoding, due to the linear k space filling in the PE direction (Figure 5).
Conclusions
The WHCA using centric ky-kz FFE with a 100% efficiency in RMC provides the entire scan time consistently almost within 5 minutes (all but one with bradycardia). In addition, applying HR-DLR offers denoising in source images and higher resolution images to improve delineation of small coronary arteries.Our proposed WHCA allows a rapid data acquisition in spite of irregular breath pattern while providing the better image quality than conventional WHCA. This technique will improve the ease-of-use of coronary artery imaging for practical use.
Acknowledgements
This work was partly supported by an NIH grant (R01HL154092) (MM).References
1. Sakuma H, Ichikawa Y, Chino S, et al. Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography. J Am Coll Cardiol. 2006; 48(10):1946-50.
2. Morita Y, Ota H, Masuda A, et al. Rapid Whole Heart Coronary MRA with 100% respiratory gating efficiency: Fast 3D Wheel data sampling with denoising deep learning reconstruction. ISMRM 2020 p1323.
Figures
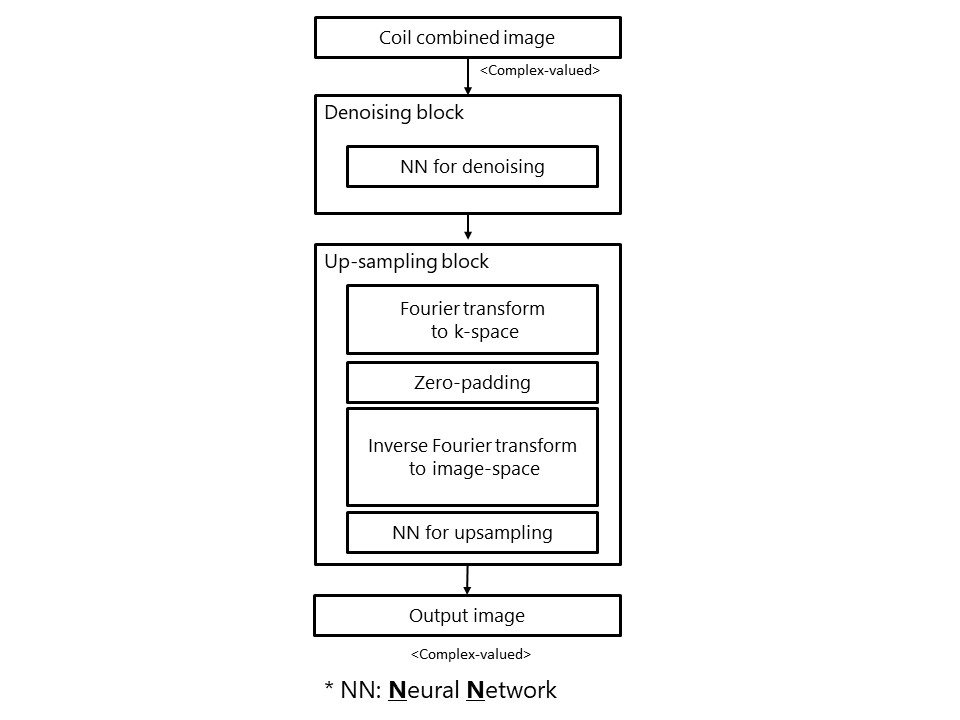
Figure 1.
High-resolution deep learning reconstruction (HR-DLR) process pipeline. The first process is denoising block followed by the second process of up-sampling block. The acquired k-space data is transformed to a complex image with coil data combined and Fourier transform. The complex-valued image is input to the neural network (NN) for denoised images. Then, the denoised images are enlarged and zero-fill interpolation (ZIP) to provide higher resolution images.
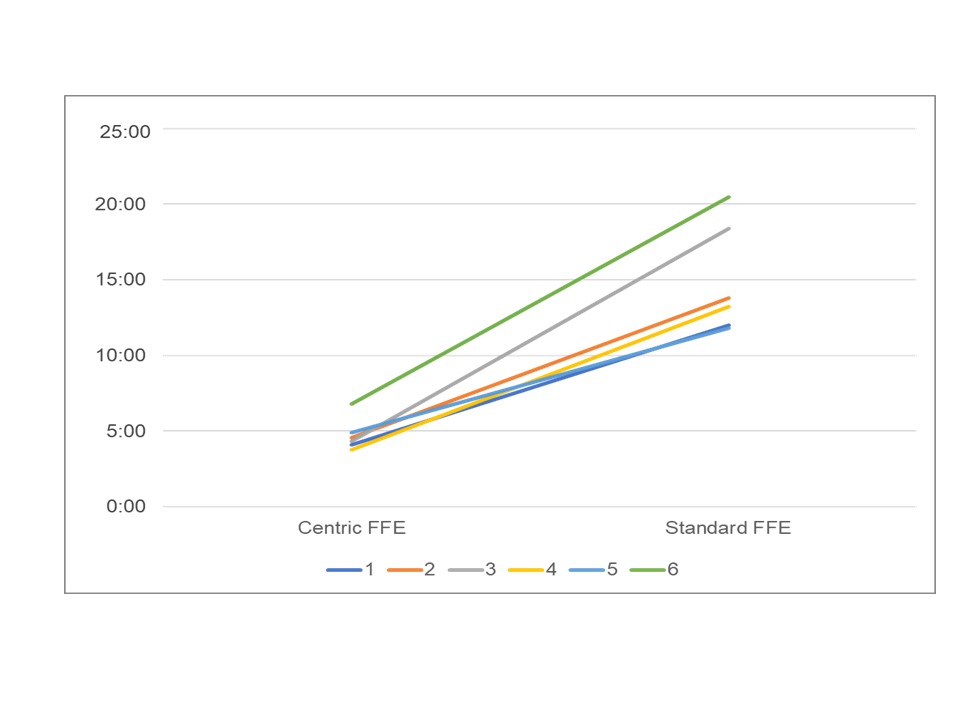
Figure 2.
Scan time of both centric FFE and standard FFE. The mean scan time was 4min.44sec. (within 5 min. all but one with bradycardia and 100% respiratory gating efficiency in all volunteers) in centric FFE and 14min. 56sec. (a various scan time with 12 to 20 minutes depending on the efficiency of RMC) in standard FFE.
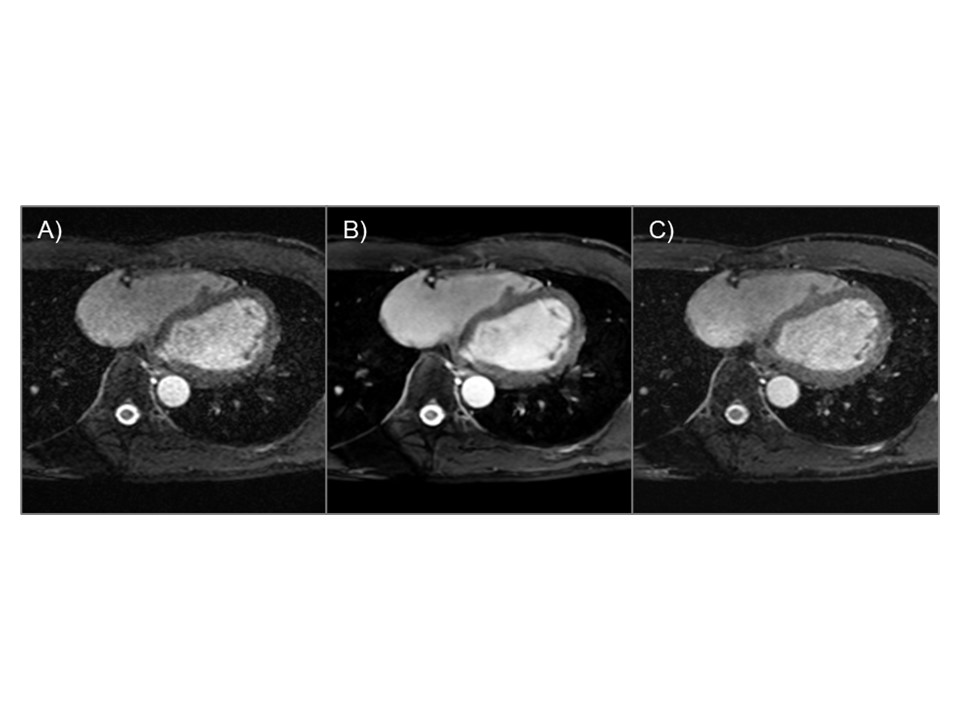
Figure 3.
A) The centric ky-kz using a 30-mm RMC threshold without HR-DLR, B) with HR-DLR, and C) Standard methods with a 5-mm RMC threshold with the scan time of 12 minutes.
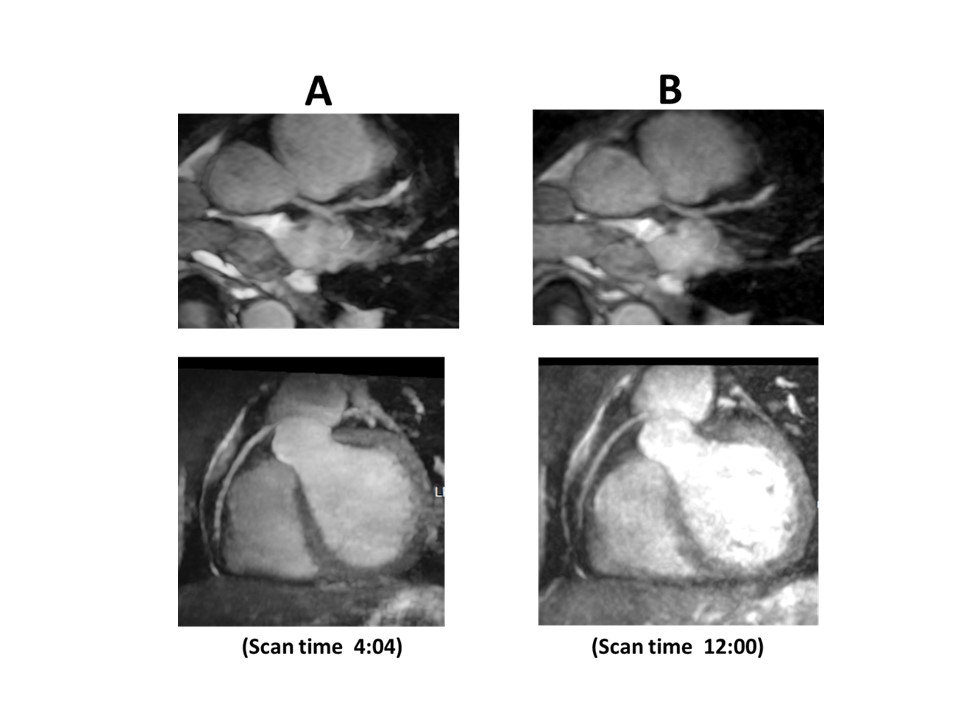
Figure 4.
Representative cases of A) our proposed WHCA (centric ky-kz FFE) and B) conventional WHCA (standard FFE) in thin-slab maximum intensity projection of left coronary artery and right coronary artery.
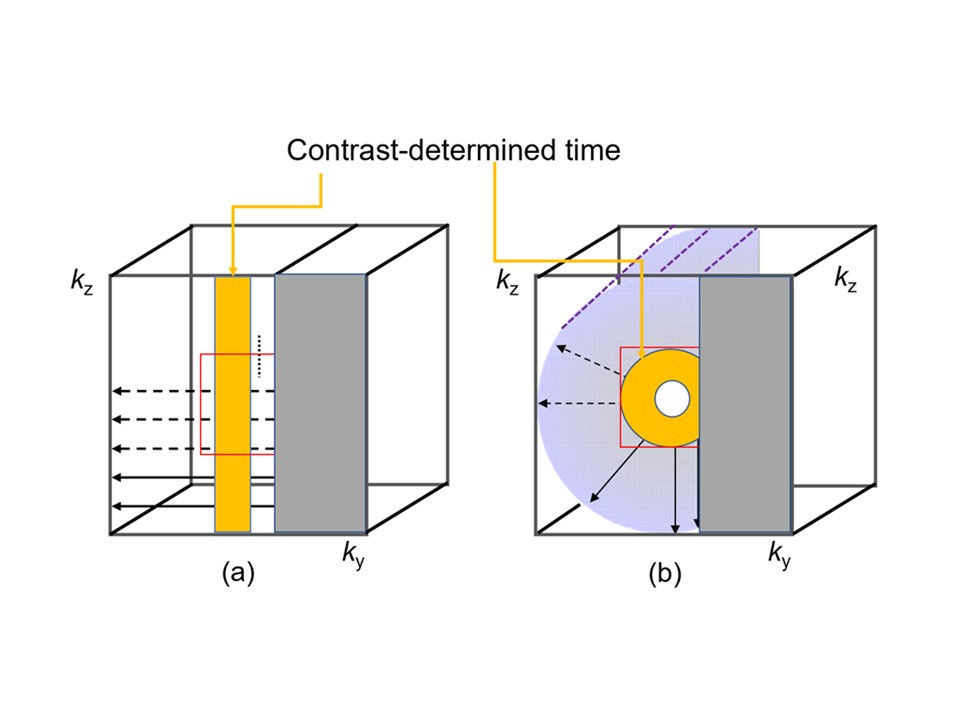
Figure 5.
Standard (a) and Centric ky-kz order (b) show contrast determined time of each acquisition. The contrast-determined time of the standard is linear with slice encoding which shows missed at the center of k space, whereas the centric order gives entire k space center within the contrast-determined time.
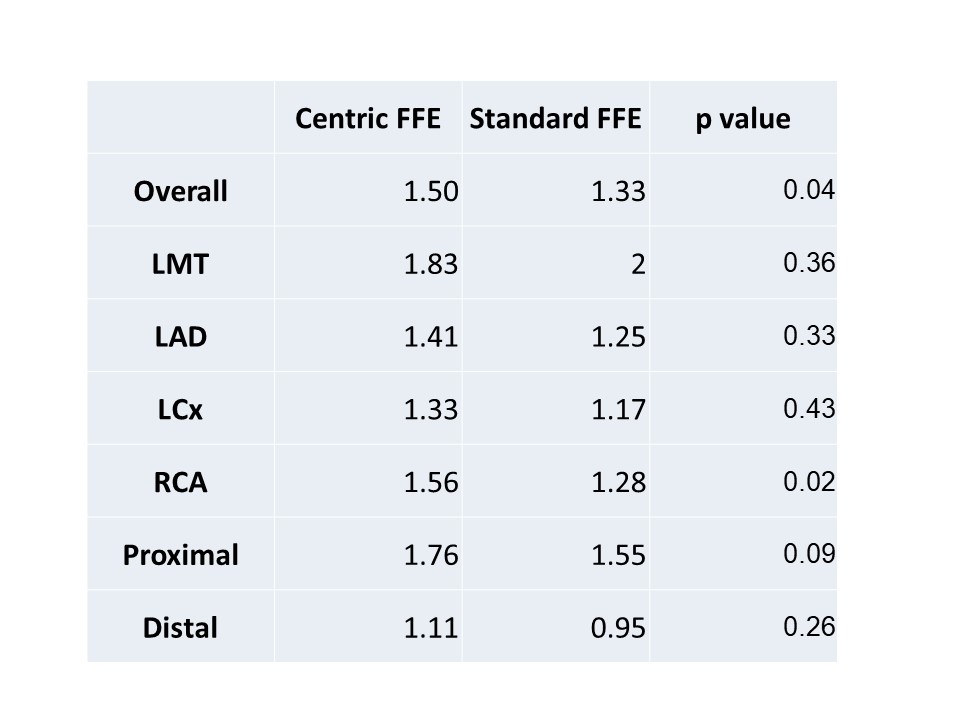
Table 1.
Image quality between centric FFE and standard FFE .