1693
Acceleration of brain MRA with Spiral, compared with Compressed SENSE1The Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Vessels, Brain, TOF
The purpose of this study is to quantitively and qualitatively evaluate the clinical feasibility of spiral-based TOF-MRA (MRAspiral) in terms of acceleration of data acquisition and imaging performance, with reference to the routine use of TOF-MRA with C-SENSE=4. The results showed that MRAspiral with τ=8 (2min7s) can significantly reduce the acquisition time by 44.3% with a balanced image quality and scan time for arteries visualization and clinical diagnosis.Introduction
Fast, safe and reliable cerebral angiography is crucial for the diagnosis, treatment planning and follow-up evaluation of cerebrovascular diseases, especially for ischemic stroke caused by thromboembolic vessel occlusion. Time-of-flight magnetic resonance angiography (TOF-MRA) is a non-invasive, non-radiation, non-contrast angiography technique to achieve three-dimensional intra- or extracranial vascular imaging and is widely used in clinic, but the acquisition time is relatively long. The compressed sensing (CS) technique based on k-space pseudo-random under-sampling is useful in fast MR imaging.1 The Compressed SENSE(C-SENSE) is a combine of the CS and the sensitivity encoding(SENSE) parallel imaging.2 Compared with routine brain TOF-MRA, MRA using C-SENSE with an acceleration factor 4 (CS=4) can significantly reduce the acquisition time without losing the image quality.3,4 Spiral imaging is recently introduced to achieve TOF-MRA imaging. This method uses spiral stacking with in-plane spiral trajectories, which has shorter echo time (TE) and inherent compensation for higher gradient moments.5 However, there is little clinical validation of spiral imaging in the evaluation of TOF-MRA acceleration and small vessel display ability.6 The purpose of this study is to quantitively and qualitatively evaluate the clinical feasibility of spiral-based TOF-MRA(MRAspiral) in terms of acceleration of data acquisition and imaging performance, with reference to the routine use of TOF-MRA with C-SENSE=4 (MRACS=4) in our hospital.Methods
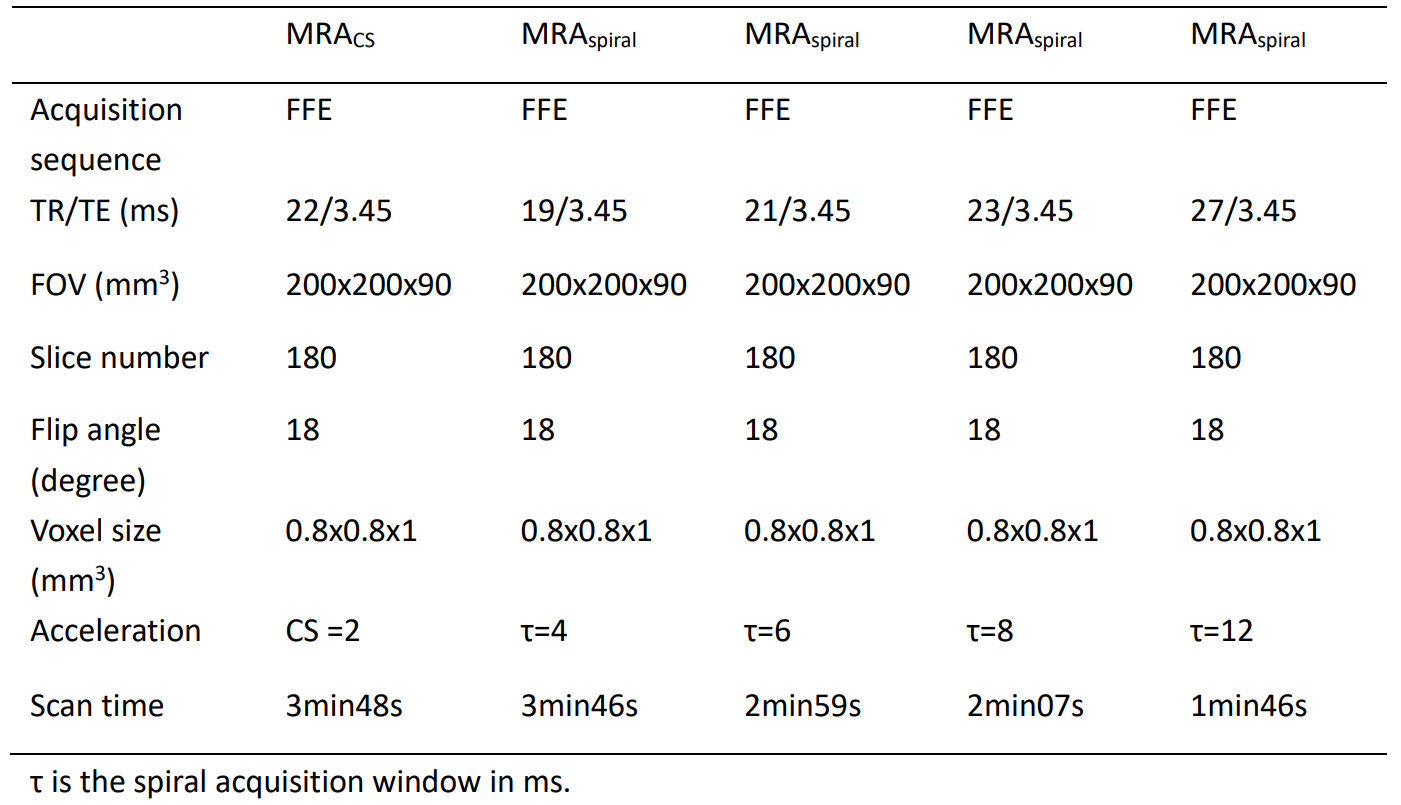
From May 22, 2021 to October 27, 2021, 29 patients with suspected cerebrovascular disease, MRACS=4 and MRAspiral (τ=4, 6, 8, 12 ms, respectively, where τ is the acquisition window for spiral imaging) sequences were prospectively collected on an 3.0T MR system (Ingenia CX, Philips Healthcare, Best, the Netherlands), and the parameters used is presented in table 1. The regions of interest (ROIs) were drawn on proximal and distal segment of posterior cerebral artery (PCA), anterior cerebral artery (ACA), middle cerebral artery (MCA). Contrast ratio (CR) values were calculated with corpus callosum as the background. Image quality and diagnostic feasibility were qualitatively analyzed by two experienced radiologists. Paired sample T test was performed for qualitative and quantitative analysis in each MRAspiral sequence compared with MRACS=4.Results
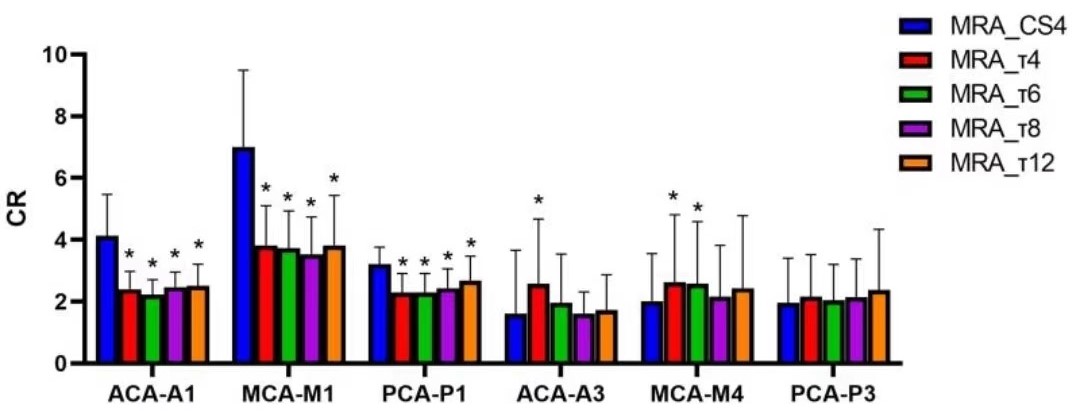
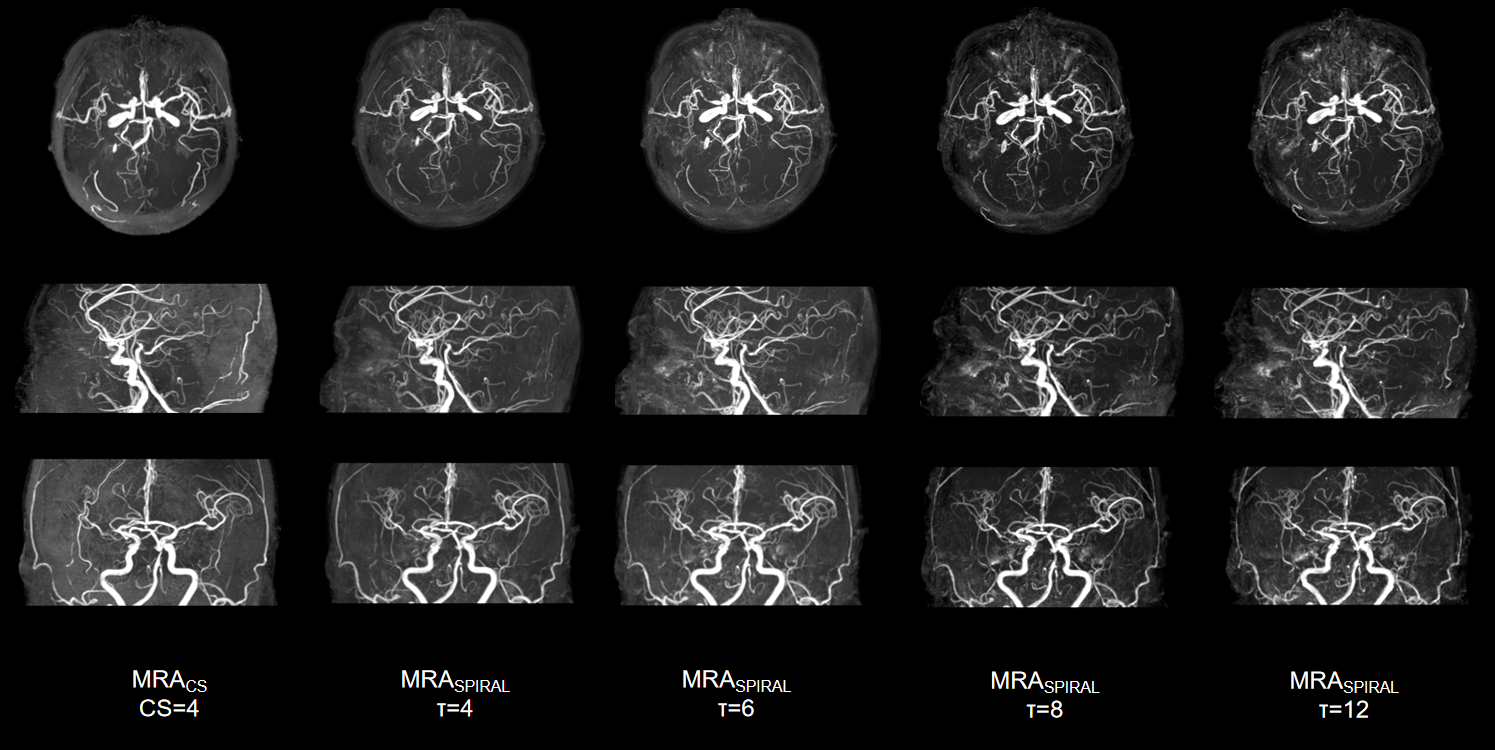
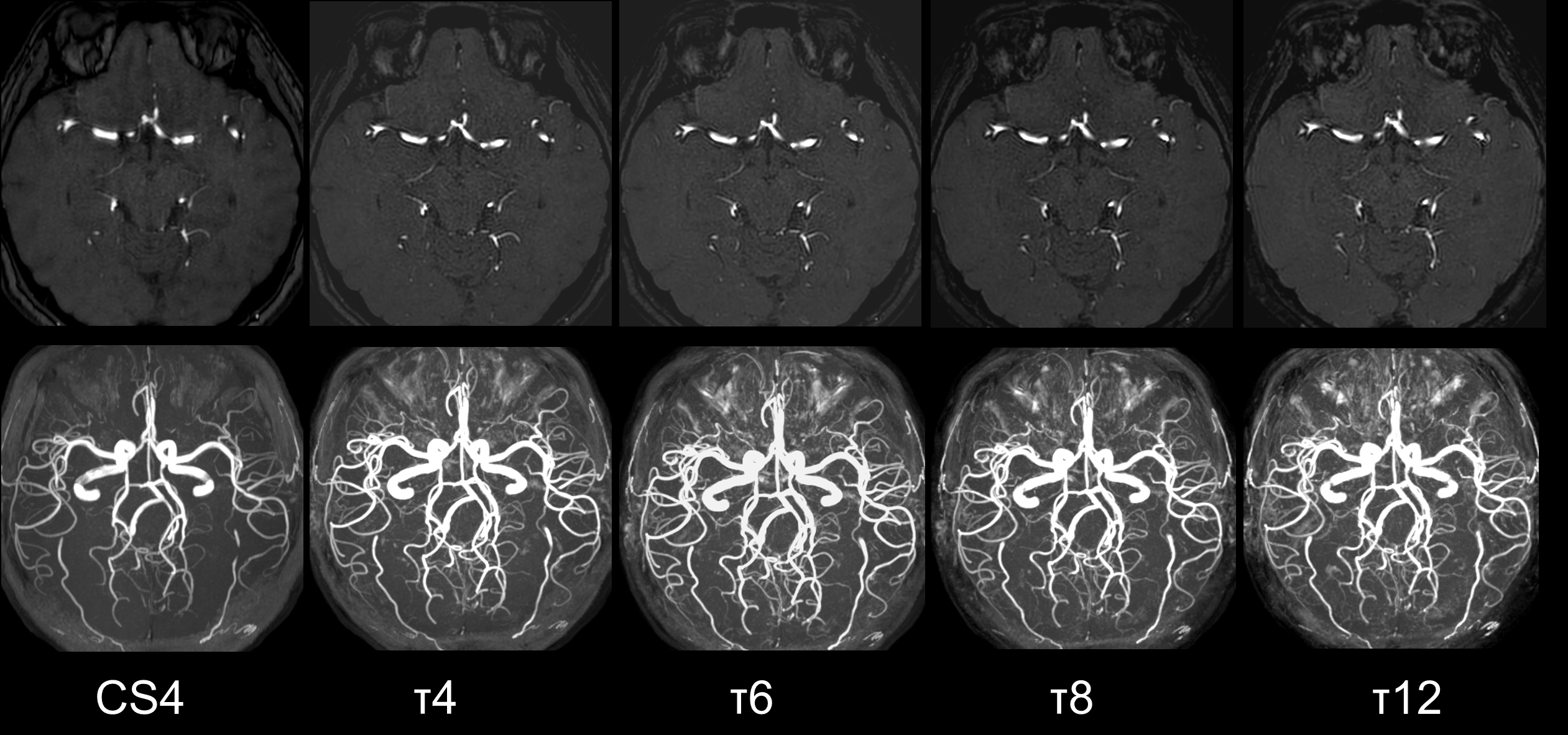
The quantitative results showed that PCA-P1, ACA-A1, MCA-M1 of MRAspiral sequence with different τ values had a lower CR than that in MRACS (all P <0.005). In the distal segment, CRMCA M4 in τ=4 and τ=6 of MRAspiral (τ4: 2.63±2.18, P=0.044; τ6: 2.58±2.01;p=0.01) were significantly higher than that in MRACS (2.00±1.55). However, CRMCA-M4 in MRAspiral with τ=8 andτ=12 were not different with MRACS=4 (all P>0.05). There was no significant statistical difference of CRACA-A3, CRPCA-P3 in MRAspiral with different τ values compared with MRACS=4 (P >0.05)(figure 1). MRAspiral with τ=4 and τ=6 had a better vessel visualization than that of MRAcs=4. MRAspiral with τ=12 had a worse vessel visualization in both proximal and distal MCA compared with MRACS=4 (all P<0.05). MRAspiral with τ=8 was not significantly different from MRACS=4 in vessel visualization (P>0.05) (table 2). Figure 2 and Figure 3 shows brain TOF-MRA images with different acceleration factors in a 76 years old patient with headache and in a 45 years old patient with vertigo.Conclusion
MRAspiral with τ=4 (3min46s) and MRAspiral with τ=6 (2min59s) can improve the vessel visualization of distal intracranial vessels compared with MRACS=4 (3min48s). MRAspiral with τ=8 (2min7s) can significantly reduce the acquisition time by 44.3% with an accessible image quality for arteries visualization.Acknowledgements
No acknowledgement found.References
1. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007 Dec;58(6):1182-95.
2. Geerts-Ossevoort L, de Weerdt E, Duijndam A, et al. Compressed SENSE. Speed done right. Every time. Philips Healthcare, Netherlands, 2018. https://philipsproductcontent.blob.core.windows.net/assets/ 20180109/619119731f2a42c4acd4a863008a46c7.pdf.AccessedMay1, 2020
3. Ding J, Duan Y, Zhuo Z, et al. Acceleration of Brain TOF-MRA with Compressed Sensitivity Encoding: A Multicenter Clinical Study. AJNR Am J Neuroradiol. 2021,42(7):1208-1215.
4. Lin Z, Zhang X, Guo L, Wang K, Jiang Y, Hu X, Huang Y, Wei J, Ma S, Liu Y, Zhu L, Zhuo Z, Liu J, Wang X. Clinical feasibility study of 3D intracranial magnetic resonance angiography using compressed sensing. J Magn Reson Imaging. 2019 Dec;50(6):1843-1851.
5. Greve T, Sollmann N, Hock A, Hey S, Gnanaprakasam V, Nijenhuis M, Zimmer C, Kirschke JS. Highly accelerated time-of-flight magnetic resonance angiography using spiral imaging improves conspicuity of intracranial arterial branches while reducing scan time. Eur Radiol. 2020 Feb;30(2):855-865.
6. Sartoretti E, Sartoretti-Schefer S, van Smoorenburg L, Binkert CA, Gutzeit A, Wyss M, Sartoretti T. Spiral 3D time-of-flight MR angiography for rapid non-contrast carotid artery imaging: Clinical feasibility and protocol optimization. Phys Med. 2022 Jan;93:20-28.
Figures