1691
Improved non-contrast-enhanced MR Venography of lower extremities using non-triggered 3D-GRE-EPI.1Philips Japan, Tokyo, Japan, 2Philips Healthcare, Tokyo, Japan, 3Kawanishi City Medical Center, Hyogo, Japan
Synopsis
Keywords: Vessels, Blood vessels, Venography
MRI is one of a promising diagnostic of lower extremity arterial and venous disease, and non-contrast-enhanced MR angiography has an array of specific applications for numerous clinical indications. In this study, we demonstrated non-contrast-enhanced non-triggered 3D gradient-echo echo-planer-imaging (3D-GRE-EPI) can provide high quality MR Venography in lower extremities. Consequently, 3D-GRE-EPI was provided high sharpness, contrast and could distinguish veins and arteries.
Introduction
Venous pathology of the lower extremities is one of critical public health problems with economic and social consequences. Ultrasonography serves as the standard modality for evaluating lower limb swelling, but sometimes it does not adequately assess the pelvic region, and it is difficult in patients exhibiting obesity, oedema, or tenderness. Although contrast-enhanced CT has been widely used in clinical practice, it is an invasive procedure MRI can provide vascular images in any anatomies without contrast enhancement. Previous studies have introduced several non-contrast-enhanced MRA techniques, for example triggered-angiography-non-contrast-enhanced (TRANCE) and steady-state-free-precession (SSFP), for evaluation of venous diseases 1-4. However, such current techniques have some limitations. TRANCE is not robust particularly in patients with arrhythmia due to its unstable cardiac synchronization. Although SSFP theoretically provides high SNR and spatial resolution for vascular imaging, it cannot distinguish arteries and veins consistently.On the other hand, non-contrast-enhanced non-triggered 3D gradient-echo echo-planer-imaging (3D-GRE-EPI) can provide high quality MR arteriogram in lower extremities 5. This technique is applying EPI readout, which enables short acquisition time, and it can acquire arteries and veins separately by modifying the placement of saturation bands like Time-Of-Flight MRA.
In this study, we tried to optimize the scan parameters of non-contrast-enhanced non-triggered 3D-GRE-EPI for venography and compared it with TRANCE and 3D-SSFP. The purpose of this study is to investigate usefulness of 3D-GRE-EPI for MR Venography of lower extremities.
Methods
A total of 3 healthy volunteers were examined on a 1.5T whole-body clinical system (Ingenia, Philips Healthcare). The volunteer obtained informed consent and approved by IRB. For 3D-GRE-EPI, we previously optimized the scan parameters to long TR(> 40ms), and low flip angle (< 10°) for venography.(1) 3D-GRE-EPI: FOV;390mm, voxel size;1.50*1.50*3.00mm3, SENSE;2.8, Slice orientation; Transverse, Scan technique;3D-FFEPI, EPI factor;9, TR;41ms, TE;9.5ms, Flip Angle;10, Fat suppression;proset, MTC;off resonance, NSA;3, Scan duration;2min37sec
(2) TRANCE: FOV;390mm, voxel size;1.50*1.50*3.00mm3, SENSE;3.5, Slice orientation;Coronal, Scan technique;3D-IR-TSE, TSE factor;50, TR;1beat, TE;106ms, TI;150ms, Refocusing Flip Angle;120, cardiac synchronization;trigger, NSA;1, Scan duration;1min51sec (Heart Rate;60)
(3) 3D-SSFP: FOV;390mm, voxel size;1.50*1.50*3.00mm3, SENSE;2.0, Slice orientation; Transverse, Scan technique;3D-balanced-TFE, TFE factor;60, TR;4.0ms, TE;2.0ms, Flip Angle;70, Fat suppression;SPAIR, NSA;1, Scan duration;2min45sec
3D-GRE-EPI and 3D-SSFP were obtained in transverse, TRANCE obtained in coronal and generated Multi Planar Reconstruction (MPR) to transverse. Furthermore, maximum intensity projection (MIP) was generated at all images (Figure 1). Regions of interests (ROIs) were placed on Deep Vein (DV), Superficial Veins (SV), Artery (A), Muscle (M), and Fat (F) at each segment of pelvis, femur and leg. The signal intensity of ROIs was calculated for Contrast Noise Ratio (CNR). We evaluated CNR between the DV and M, SV and F, DV and A on comparison of three techniques. The CNR were calculated using the following formulas, and it was evaluated of using the paired t test (P=0.05).
$$CNR=\frac{\mid SI_{a}-SI_{b}\mid }{\sqrt{(SD_{a}{})^2+(SD_{b})^2}}$$
SIa,b and SDa,b are defined as the mean signal intensity (SI) and standard deviation (SD) measured in the ROIs. Image quality for the visualization of veins were compared to the source, MPR and MIP images. It was scored by observers (three radiographer with more 10 years of MRI experience) in consensus on a four-point Likert scale regarding sharpness, contrast and separate of arteries and veins (1=unacceptable, 2=poor, 3=good, 4=excellent), furthermore, evaluated of using the Wilcoxon signed-rank test (P=0.05).
Results and Discussions
The CNR compared to 3D-GRE-EPI and TRANCE, 3D-SSFP is shown in Figure2. The CNR of DV and M in pelvis was significantly higher on TRANCE than 3D-GRE-EPI, Although the other parts were no significant difference. DV and A in all parts were significantly higher on 3D-GRE-EPI than 3D-SSFP, and the other CNR were no significant difference. 3D-GRE-EPI is same level of CNR of vein signals compared to other technique, in healthy volunteer with sinus rhythm. Although, 3D-GRE-EPI can be distinguish arteries and veins without any triggering. The results of visualization of image quality are shown in Figure 3. The all of 3D-GRE-EPI visual scored same level or higher than TRANCE and 3D-SSFP. In Addition, we obtained good image quality of venography of whole lower extremities in healthy volunteer (Figure 4). Consequently, 3D-GRE-EPI was provided high sharpness, contrast and could distinguish veins and arteries.Conclusion
Non-contrast-enhanced, non-triggered 3D-GRE-EPI might be useful technique of MR venography of lower extremities with high robustness.Acknowledgements
The authors thank them for valuable assistance in this study :
Shouichi Andou RT, Ken Ohno RT, Kawanishi City Medical Center, Hyogo, Japan
References
1. Huang, Yao-Kuang, Tseng, Yuan-Hsi, Lin, Chih-Hung, et al. "Evaluation of venous pathology of the lower extremities with triggered angiography non-contrast-enhanced magnetic resonance imaging". BMC Medical Imaging 19, no.1 (17 Dec.2019): 1-9. doi:10.1186/s12880-019-0395-4.
2. Chen, Chien-Wei, Ting, Hua, Chen, Pang-Yen, et al. "Usefulness of triggered non-contrast-enhanced magnetic resonance angiography in assessing lower extremity venous disease". Medicine 100, no.20 (21 May.2021): e25809. doi:10.1097/MD.0000000000025809.
3. Koizumi, Jun, Hashimoto, Takeshi, Myogin, Kazunori, et al. "Angiography for the Lower Limb Diseases including Venous Thromboembolism". The Japanese Journal of Phlebology 21, no.1 (2010): 17-27. doi:10.7134/phlebol.21-1-17.
4. Tutar, Burcin, Kantarci, Fatih, Cakmak, Osman Serdal, et al. "Assessment of deep venous thrombosis in the lower extremity in Behçet’s syndrome: MR venography versus Doppler ultrasonography". Internal and Emergency Medicine 14, no.5 (1 Aug.2019): 705-711. doi:10.1007/s11739-019-02040-4.
5. Komaki, Shinsuke, Kida, Katsuhiro, Hayashi, Yukako, et al. "Non-electrocardiogram-gated and Non-contrast-enhanced Magnetic Resonance Angiography of the Lower Limb Arteries Using Three-dimensional MultishotT1-weighted…". Nihon Hoshasen Gijutsu Gakkai zasshi 78, no.4 (2022): 333-341. doi:10.6009/jjrt.2022-1239.
Figures
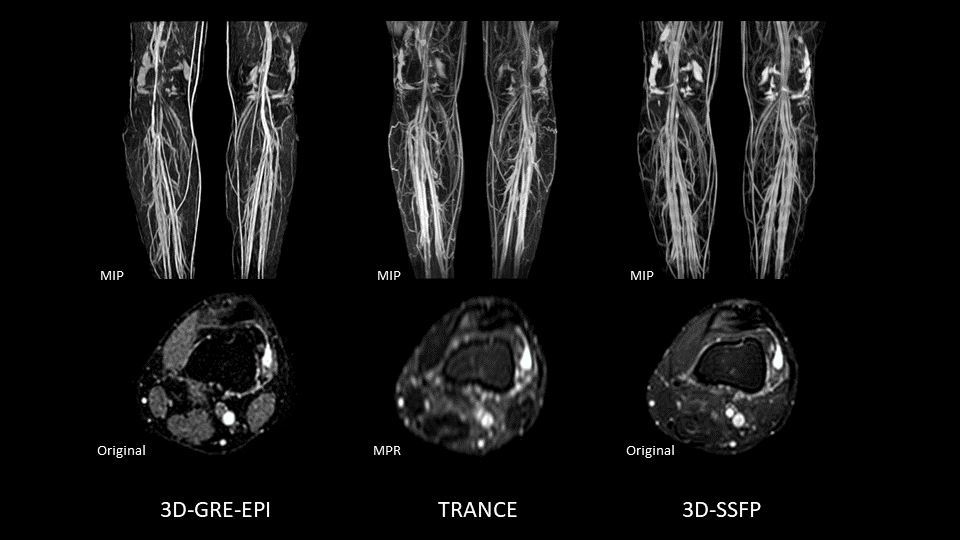
Figure 1.
The images of each scan technique of MR Venography of lower extremities. 3D-GRE-EPI and 3D-SSFP were obtained in transverse, TRANCE obtained in coronal and generated Multi Planar Reconstruction (MPR) to transverse. Furthermore, maximum intensity projection (MIP) was generated at all images.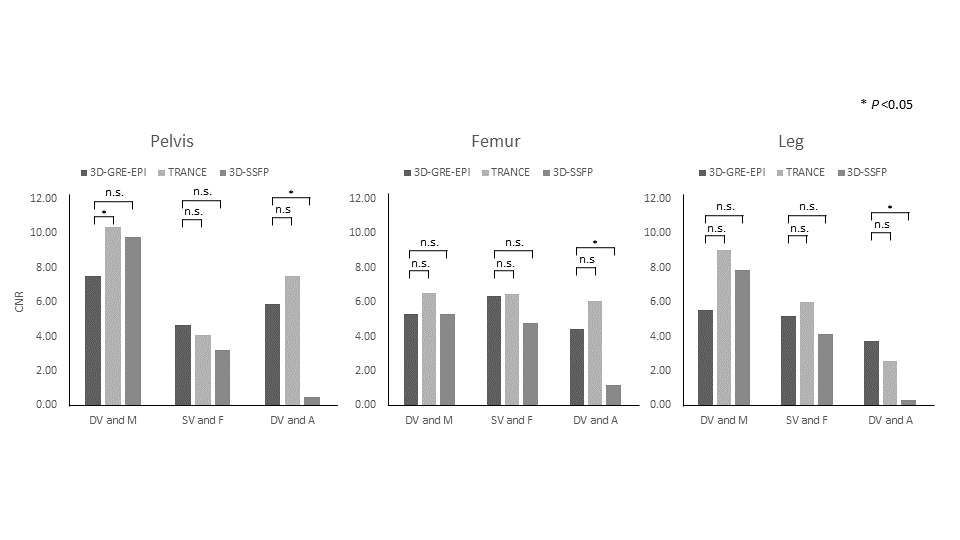
Figure 2.
The Result of CNR compared of 3D-GRE-EPI and TRANCE, 3D-SSFP. The CNR of DV and M in pelvis was significantly higher on TRANCE than 3D-GRE-EPI, Although the other parts were no significant difference. DV and A in all parts were significantly higher on 3D-GRE-EPI than 3D-SSFP, and the other CNR were no significant difference.
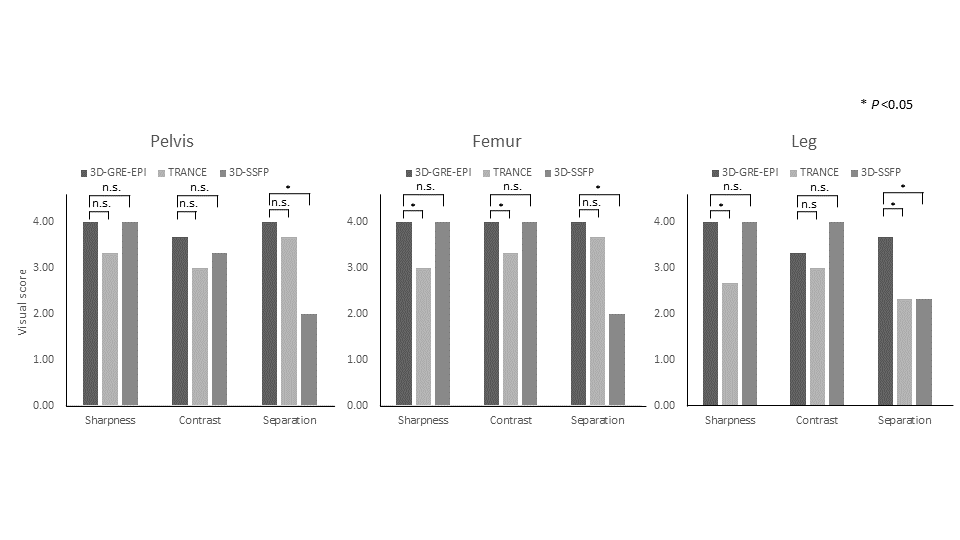
Figure 3.
The results of visualization of image quality. The all of 3D-GRE-EPI visual scored same level or higher than TRANCE and 3D-SSFP.
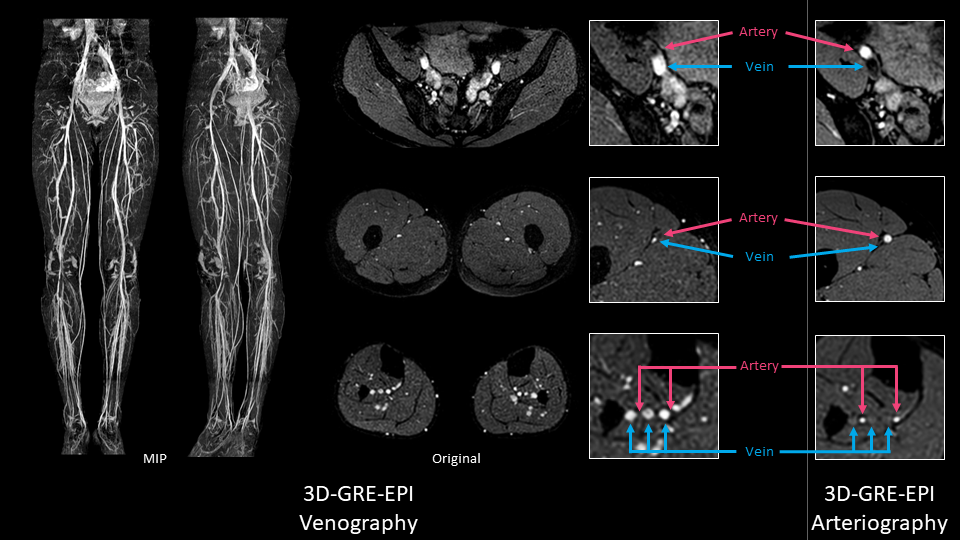
Figure 4.
Non-contrast-enhanced MR Venography of whole lower extremities using non-triggered 3D-GRE-EPI. The images shown the venous signal well visualized from proximal to distal, and high sharpness, contrast and could distinguish veins and arteries. Right hand side is MR Arteriography using non-triggered 3D-GRE-EPI, it was obtained because of visualizing running of the arteries.