1688
MRA for Pulmonary Embolism to Conserve Iodinated Contrast Media During an Acute Supply Chain-related Shortage1Radiology, University of Wisconsin-Madison, Madison, WI, United States, 2Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 3Biomedical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 4Medicine, University of Wisconsin-Madison, Madison, WI, United States, 5Emergency Medicine, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Vessels, MR Value
The closure of GE Healthcare’s Shanghai facility in April 2022 during the COVID-19 lockdown in China led to a major supply chain disruption of iodinated contrast media in North America. In response, our department instituted measures to conserve iodinated contrast, including the use of MRA as an alternative to contrast enhanced CTA to evaluate for pulmonary embolus (PE). Over the period of April through July of 2022, this strategy conserved an estimated 27 liters of iohexol 350 mg/ml. We report our experience on the use of MRA for diagnosis of PE in the general population during this period.Background
The shutdown of a GE Healthcare manufacturing facility in Shanghai, China in April 2022 as a result of the local COVID-19 policy1 led to a major disruption in the supply of iodinated intravenous contrast media products iohexol (OmnipaqueTM) and iodixanol (VisipaqueTM)2. In response, several strategies were proposed to minimize iodinated contrast usage.3–5 Accordingly, our department pivoted to the use of MR angiography (MRA) for the diagnosis of pulmonary embolism (PE) as an alternative to CT angiography (CTA), beginning in May until iodinated contrast supplies were restored by mid-July.The purpose of this study is to report our experience on the use of MRA for the diagnosis of PE in the general population as an alternative to CTA in the setting of an iodinated contrast shortage.
Methods
This HIPAA-compliant, retrospective study was conducted with IRB approval with a waiver of informed consent. Electronic health records (EHR) were searched for CTA and MRA performed for PE from April 1 to July 31 in years: 2019 (pre-pandemic), 2021 (pandemic, before the iodinated contrast shortage) and 2022 (pandemic, during the iodinated contrast media shortage).Our MRA protocol typically includes, localizer, pre-contrast-, (pulmonary) arterial-, early delayed- and low flip angle delayed-phase T1-weighted (T1w) MRA, and fat-saturated T1w spoiled gradient echo (REF blinded). Balanced steady state free precession CINE in a single axial plane was included to determine right heart strain.
Demographics, patient hospital status: inpatient (I), outpatient (O), emergency department (ED) were reviewed; acquisition date/time and exam order time were documented; exam time (time passed between localizer/pre-scan and final MRA sequence/CTA scan as documented in PACS) and order-to-start of exam time (time passed between exam order and localizer/pre-scan) were determined. Radiology reports were reviewed for image quality and PE findings (positive, PE+; negative, PE-).
Statistical analysis was performed using Excel (v16.58, Microsoft) and R (packages table1 v1.4.2, tidyverse v1.301, rstatix v0.7.0). Chi-squared test, one-way ANOVA and Student’s t test were performed. Continuous data are presented as mean ±standard deviation and median [Q1, Q3]. Finally, the total volume of iodinated contrast agent savings was calculated based on the estimated number of CTA exams avoided and the recommended dose for pulmonary angiography6 of 1ml/kg iohexol 350mg/ml. Statistical significance was defined as p<.05.
Results
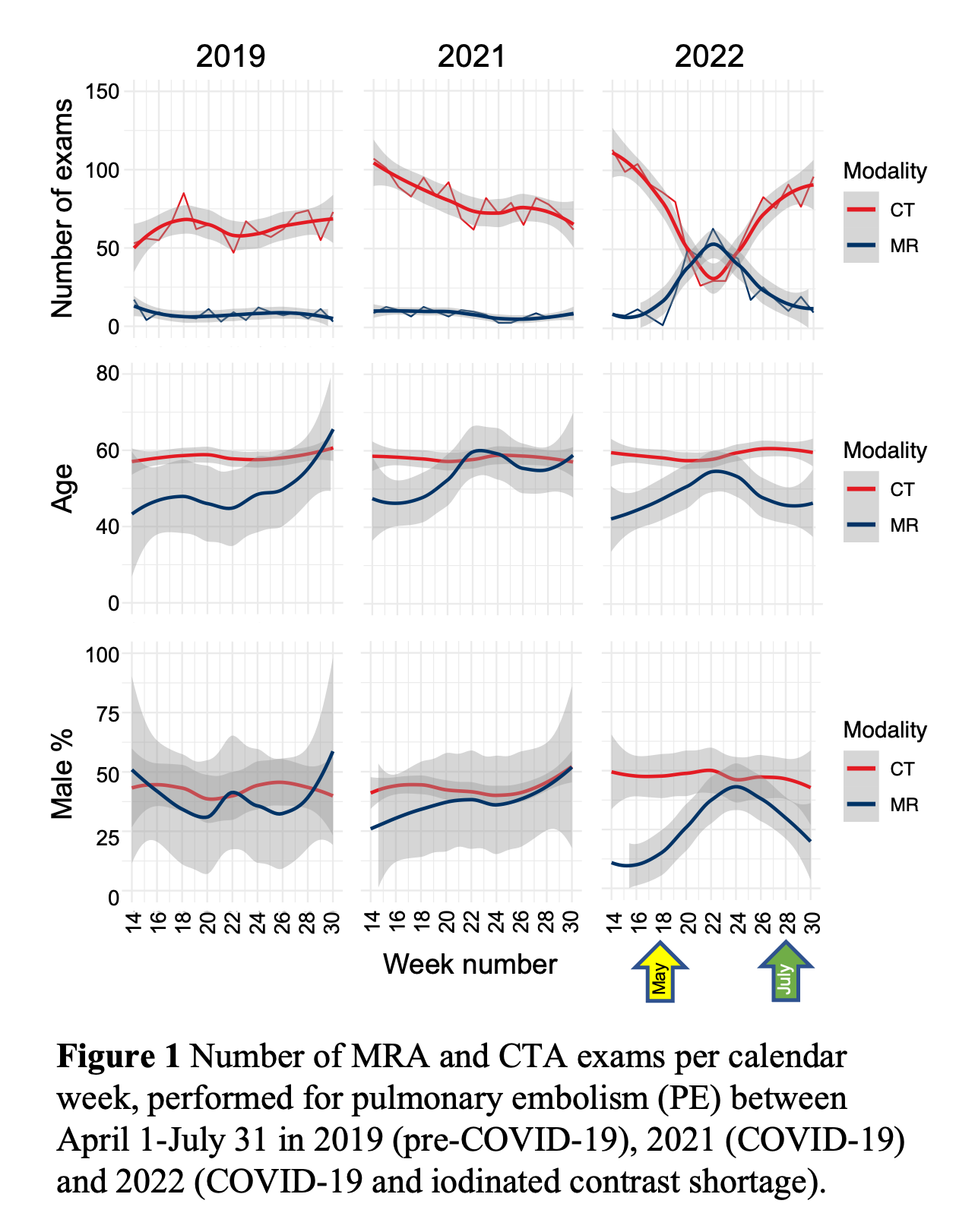
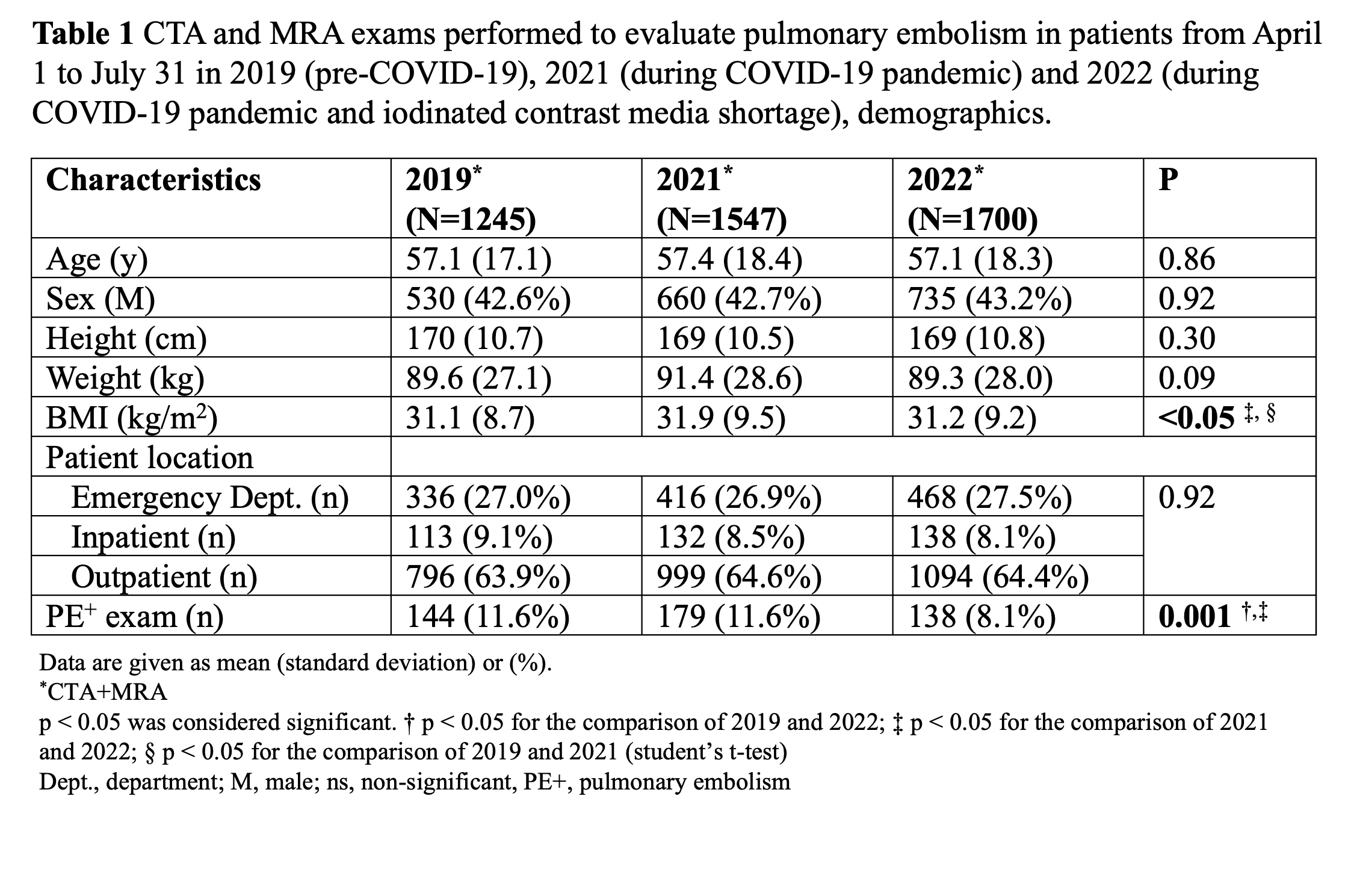
Between April to July, 1245 exams (1111 CTA/134 MRA) were performed in 2019, 1547 exams (1403 CTA/144 MRA) in 2021, and 1700 exams (1282 CTA/418 MRA) in 2022. The age, sex and patient hospital status did not differ significantly between the respective years (Table 1).In comparison to previous years, there was a substantial increase in the number of MRA exams performed in 2022 with a start in early May (Figure 1), with a peak in early June (wk28), and a return to pre-shortage routine beginning in early July and onwards.
There was no difference in sex (p=0.44) with 50/134 (37%), 52/144 (36%) and 134/418 (32%) men, and age (47 ±19, 52 ±21 and 50 ±19 years, p=0.06) for MRA groups in 2019, 2021, and 2022, respectively. However, there was a slight increase in mean age and a concomitant increase in % of males undergoing MRA, during wk18-28 of 2022 during the iodinated contrast shortage (Figure 1).
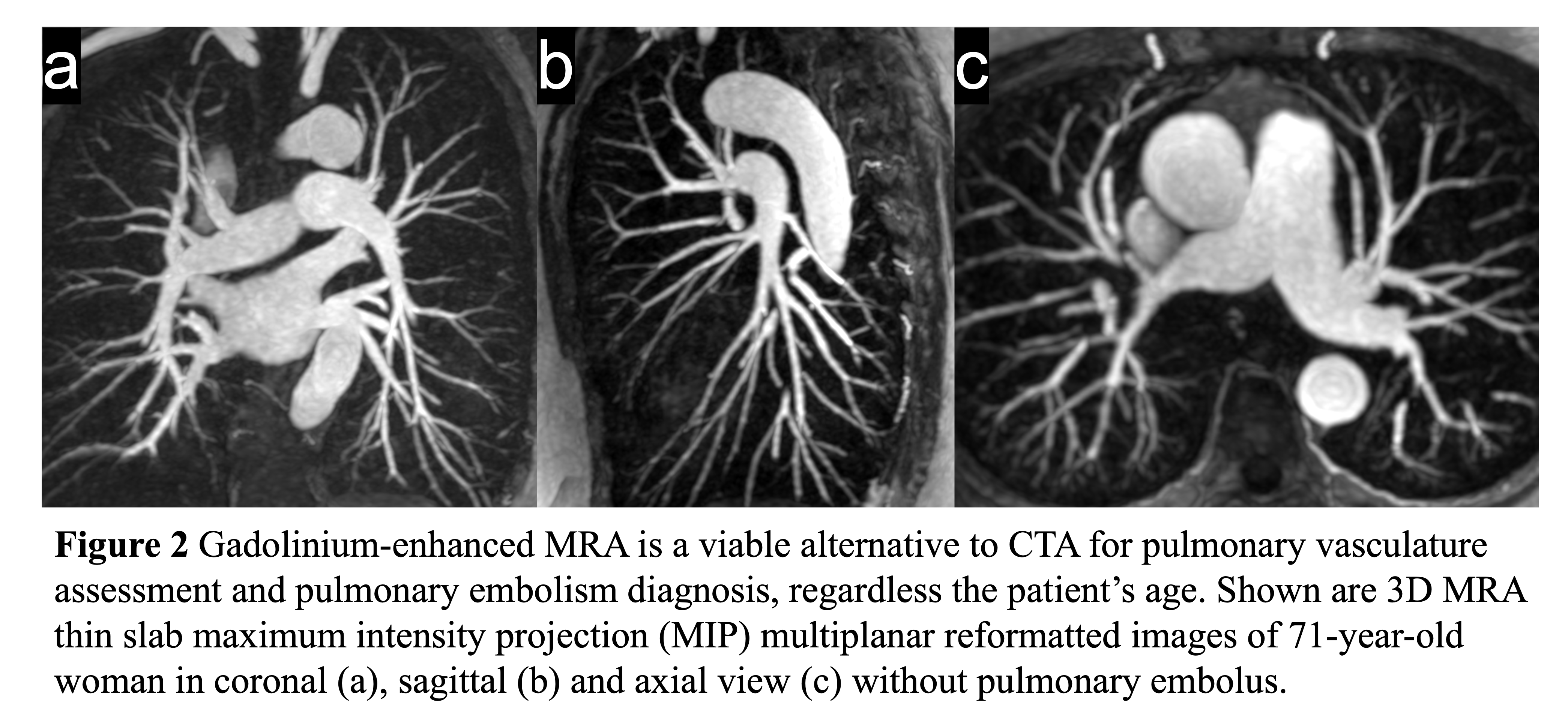
Overall, there was an estimated growth in CTA volume/year of 13% (for the period April-July). The use of MRA (Figure 1 and 2) as an alternative to CTA in 2022 resulted in an estimated savings of 27L of iohexol, equivalent to 218 bottles of iohexol 350mg/ml (125ml each).
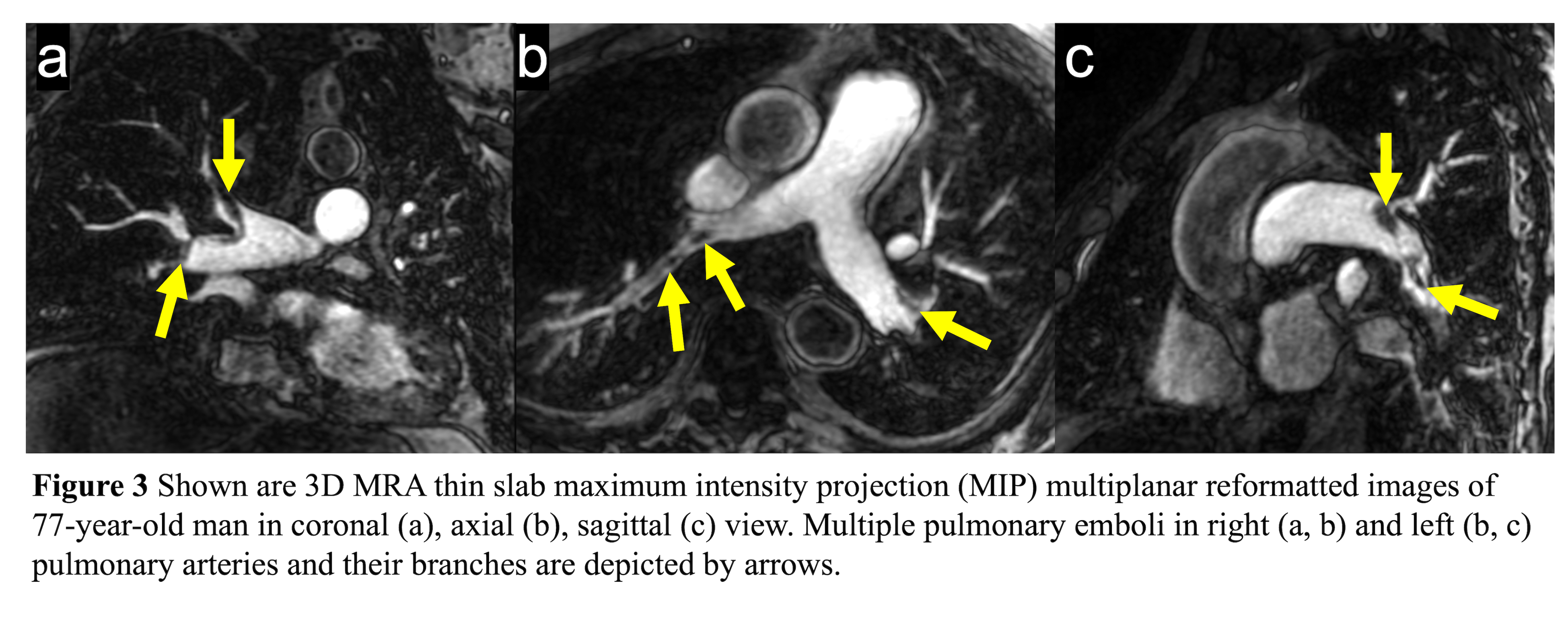
Overall, there was a lower prevalence of PE+ patients (CTA+MRA) in 2022, with 8.1% in 2022 vs. 11.6% in 2019 and 2021 (p=0.001, Table 1). The number of PE+ MRA exams (Figure 3) were similar with 9/134 (6.7%) in 2019, 11/144 (7.6%) in 2021 and 24/418 (5.7%) in 2022, p=0.7.
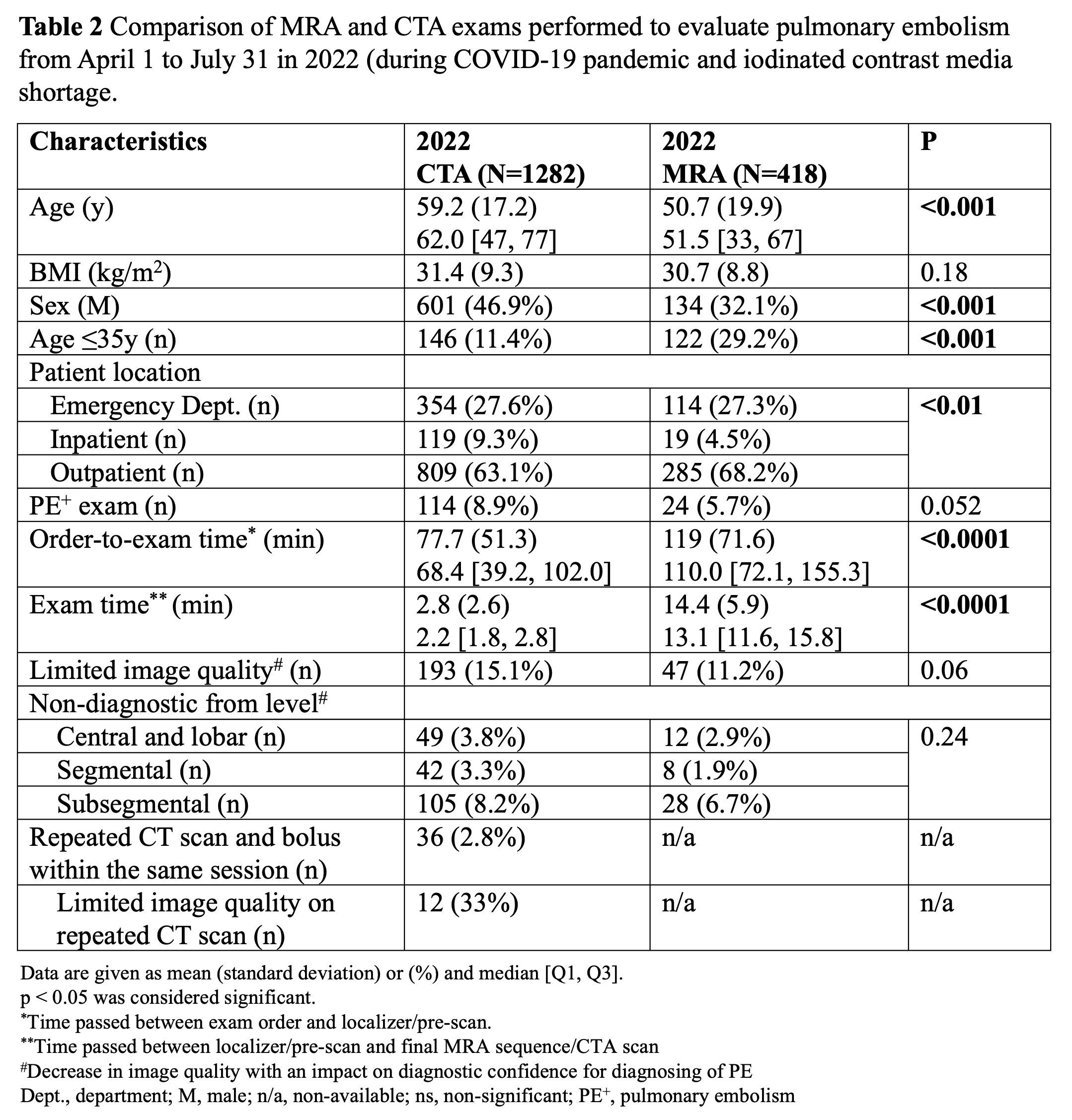
The time elapsed between the order request and the start of the exam was 68min [39, 102] for CTA and 110min [72, 155] for MRA. The CTA and MRA exam-time were 2min [1.8, 2.8] and 13min [11.6, 15.8], respectively. The number of PE+ exams in 2022 did not differ between the CTA and MRA, and image quality performance was similar between the two modalities (Table 2).
Discussion
Initially, it was believed that the iodinated contrast shortage caused by the COVID-19 lockdown in Shanghai could be resolved within weeks. However, it took five months before one of the contrast media, iodixanol, was removed from the FDA shortage list, while iohexol (limited availability of some of the products as of 10/12/2022) has remained on the list.2MRA is an established method for diagnosis of PE7 and can be performed within as little as 5-8 min.8,9 However, its use is often restricted to younger patients (ionizing-radiation protection), patients allergic to contrast media or pregnant patients.7,9 In this work we successfully demonstrated the feasibility of pulmonary MRA for the diagnosis of PE use in the general population as an alternative to CTA during an acute iodinated contrast media shortage.
Conclusion
A timely pivot to pulmonary MRA for diagnosis of PE, from CTA, helped to mitigate the impact of the pandemic related iodinated contrast shortage of 2022.Acknowledgements
The authors wish to acknowledge support from GE Healthcare and Bracco Diagnostic who provide research support to the University of Wisconsin. Dr. Reeder is the Fred Lee Sr. Endowed Chair of Radiology. Dr Lubner’s spouse works for Elephase Bio.References
1. GE Healthcare update on iodinated contrast media. Press release. doi:https://www.ge.com/news/press-releases/ge-healthcare-update-on-iodinated-contrast-media
2. FDA Drug Shortages. Current and Resolved Drug Shortages and Discontinuations Reported to FDA. Published online September 30, 2022. doi:https://www.fda.gov/drugs/drug-safety-and-availability/drug-shortages
3. Davenport MS, Chu P, Szczykutowicz TP, Smith-Bindman R. Comparison of Strategies to Conserve Iodinated Intravascular Contrast Media for Computed Tomography During a Shortage. JAMA. 2022;328(5):476. doi:10.1001/jama.2022.9879
4. Grist TM, Canon CL, Fishman EK, Kohi MP, Mossa-Basha M. Short-, Mid-, and Long-term Strategies to Manage the Shortage of Iohexol. Radiology. 2022;304(2):289-293. doi:10.1148/radiol.221183
5. Reeder SB, Hess CP, Zaharchuk G, Moy L, on behalf of the ISMRM. Magnetic Resonance Imaging as an Alternative to Contrast‐Enhanced Computed Tomography to Mitigate Iodinated Contrast Shortages in the United States: Recommendations From the International Society for Magnetic Resonance in Medicine. Magnetic Resonance Imaging. 2022;56(3):655-65. doi:10.1002/jmri.28282
6. Highlights of prescribing information Omnipaque. www.accessdata.fda.gov. Accessed 10/27/2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/018956s101lbl.pdf
7. Benson DG, Schiebler ML, Nagle SK, François CJ. Magnetic Resonance Imaging for the Evaluation of Pulmonary Embolism: Topics in Magnetic Resonance Imaging. 2017;26(4):145-151. doi:10.1097/RMR.0000000000000133
8. Schiebler ML, Nagle SK, François CJ, et al. Effectiveness of MR angiography for the primary diagnosis of acute pulmonary embolism: Clinical outcomes at 3 months and 1 year: Effectiveness of MRA for PE Primary Diagnosis. J Magn Reson Imaging. 2013;38(4):914-925. doi:10.1002/jmri.24057
9. Starekova J, Nagle SK, Schiebler ML, Reeder SB, Meduri VN. Pulmonary MRA During Pregnancy: Early Experience With Ferumoxytol. J Magn Reson Imaging. 2022 Oct 31. doi: 10.1002/jmri.28504. Epub ahead of print. PMID: 36315131.
Figures