1687
Simultaneous 3D Whole-Heart Bright-Blood and Black-Blood Imaging with iNAV-based Non-Rigid Motion-Corrected Reconstruction at 0.55T1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 3Millennium Institute for Intelligent Healthcare Engineering, Santiago, Chile, 4MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 5Electrical Engineering Department, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Heart, Low-Field MRI
In this work, we demonstrate the feasibility of free-breathing whole-heart simultaneous bright-blood and black-blood imaging at 0.55T. We implemented an image navigator (iNAV)-based non-rigid motion-corrected 2 heartbeat sequence with 100% respiratory scan efficiency and high-dimensional patch-based low-rank (HD-PROST) denoising. The research sequence was validated on one healthy subject, showing simultaneous 3D visualization of cardiovascular anatomy on bright and black blood images at 0.55T in under 12 minutes scan time.Introduction
Bright-blood and black-blood imaging can be used to enable lumen and vessel wall visualization, which allows assessment of the integrity of the great thoracic vessels and cardiac structures1. Current clinical protocols acquire these contrasts sequentially, in different orientations and with different spatial resolution often resulting in long exams and misregistration artefacts. The simultaneous acquisition of co-registered bright-blood and black-blood images with interleaved T2 preparation (T2-Prep) and Inversion Recovery (IR) prepulses (iT2prep-BOOST) in alternating heartbeats addresses this problem. This approach has been used successfully in conjunction with (iNAV)-based2 non-rigid motion-corrected reconstruction obtaining 100% respiratory scan efficiency at 1.5T3. In this study, we sought to investigate the feasibility of iNAV-based non-rigid motion-corrected 3D BOOST on the latest 0.55T MR scanner generation, which could make BOOST potentially more accessible and affordable.Methods
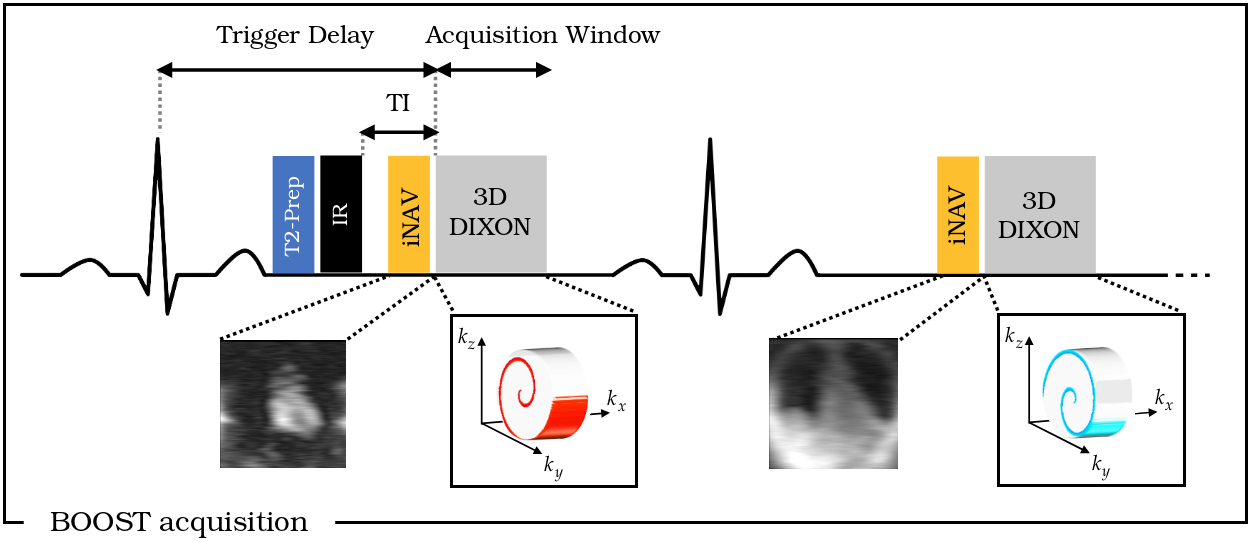
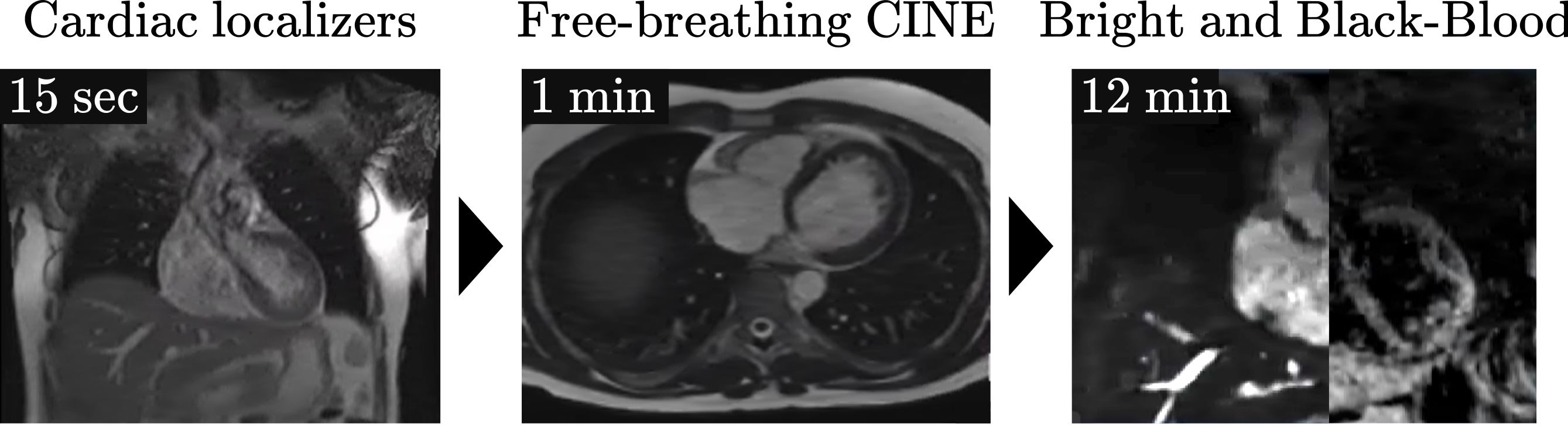
The proposed accelerated whole-heart BOOST framework was performed in one healthy subject on a 0.55T scanner (MAGNETOM Free.Max, Siemens Healthcare, Erlangen, Germany) using a 3D DIXON research sequence with an undersampled variable-density cartesian trajectory with spiral-like profile order (VD-CASPR). T2 preparation (T2-Prep) and Inversion Recovery (IR) pre-pulses were applied before the acquisition in the first heartbeat, whereas no preparation was included in the second heartbeat. A 2D iNAV3 preceded each spiral-like arm acquisition to enable beat-to-beat 2D translational motion correction and respiratory binning of the 3D datasets resulting in 100% respiratory scan efficiency (Fig.1). Estimated bin-to-bin non-rigid 3D motion fields are then incorporated into a non-rigid motion-compensated reconstruction4. Motion-compensated reconstruction was performed with iterative SENSE (itSENSE) with and without high-dimensional patch-based low-rank denoising (HD-PROST)5. Water-fat separation of the two acquired contrasts was performed, followed by direction subtraction to obtain the black-blood volume. Acquisitions parameters included: FOV = 307 x 307 x 115 mm, resolution = 1.6 mm3, flip-angle = 8 deg, TR = 9.4 ms, TE1 = 1.87 ms, TE2 = 6.47 ms, T2-Prep duration = 50 ms, IR TI = 155 ms, 4x acceleration, resulting in a total scan time of ~12 min. Shimming box, REST slab location, and trigger delay were set following the steps described in Fig. 2. Free-breathing 2D CINE was performed to determine the subject-specific trigger delay (mid-diastole) and acquisition window (~120ms).Results
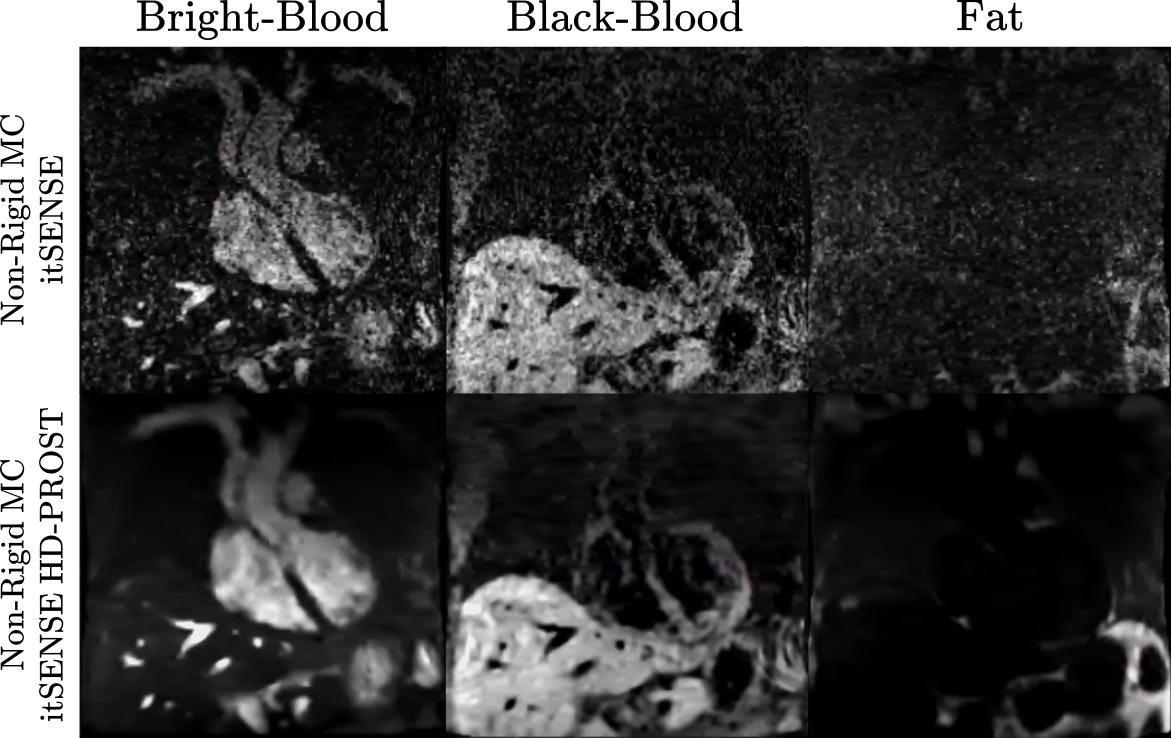
Non-rigid motion-corrected (MC) itSENSE reconstructions with and without HD-PROST denoising are shown in Fig.3. The non-rigid MC itSENSE reconstruction exhibit low SNR at low field. The proposed approach greatly increases image quality due to the further incorporation of HD-PROST denoising, which partially compensates for low SNR at low field. The use of DIXON readouts generates good water, and fat separations (Fig.3). This can be challenging at lower fields as the fat and water peaks are closer together (in frequency), thus making fat suppression harder for spectrally selective pulses like Fat Saturation or SPAIR. A video going through coronal slices for the healthy subject is shown in Figure 4.Conclusions
In this work, we demonstrated a first proof of concept of iNAV-based whole-heart simultaneous bright-blood and black-blood imaging at 0.55T in ~12 min scan time, generating co-registered lumen and wall visualization of cardiac structures. Future work will focus on further parameter optimization to increase the quality of the images, and evaluation in healthy subjects and patients with cardiovascular disease.Acknowledgements
This work was supported by the following grants: (1) EPSRC P/V044087/1 and EP/S022104/1, (2) BHF programme grant RG/20/1/34802, (3) Wellcome/EPSRC Centre for Medical Engineering (WT 203148/Z/16/Z), (4) Millennium Institute for Intelligent Healthcare Engineering ICN2021_004, (5) FONDECYT 121074, 1210637 and 1210638, (6) IMPACT, Center of Interventional Medicine for Precision and Advanced Cellular Therapy, ANID FB210024, (7) PhD program in Biological and Medical Engineering of the Pontificia Universidad Católica de Chile.References
1. Henningsson, M., Malik, S., Botnar, R., Castellanos, D., Hussain, T. and Leiner, T. (2022), Black-Blood Contrast in Cardiovascular MRI. J Magn Reson Imaging, 55: 61-80. https://doi.org/10.1002/jmri.2739
2. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012;67(2):437–45.
3. Milotta, G, Ginami, G, Cruz, G, Neji, R, Prieto, C, Botnar, RM. Simultaneous 3D whole-heart bright-blood and black blood imaging for cardiovascular anatomy and wall assessment with interleaved T2prep-IR. Magn Reson Med. 2019; 82: 312– 325. https://doi.org/10.1002/mrm.27734
4. Cruz G, Atkinson D, Henningsson M, et al. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2017;77(5):1894-1908.
5. Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med. 2019 Jun;81(6):3705-3719. doi: 10.1002/mrm.27694. Epub 2019 Mar 4. PMID: 30834594; PMCID: PMC6646908.
Figures