1685
Whole-heart NCMRA Using Single-Breath-Hold TFE EPI at 3T:Comparison with 3D-mDixon TFE Coronary MRA on Healthy Volunteers1Central Hospital Affiliated to Shandong First Medical University, Jinan, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Heart, Cardiovascular
Non-contrast-enhanced whole-heart coronary MRA(NCMRA) is a noninvasive modality for the detection of coronary artery disease. 3D-mDixon with compressed SENSE has been used in clinical practices but was limited to its scanning time of approximately 5-15 minutes. The EPI technique could shorten the scan time in MRI acquisition. The study aimed to evaluate the image quality of single breath-hold TFE-EPI NCMRA and 3D-mDIXON NCMRA with compression SENSE in healthy volunteers. The results showed there was no significant difference in image contrast between the LM, RCA proximal, and LAD proximal. The single breath-hold TFE-EPI sequence might have its own unique advantages.
Introduction
Coronary MRA (CMRA), which is safe, noninvasive, radiation-free, and iodine-free, has gradually emerged as an alternative imaging option for detecting coronary artery stenosis [1-2].Moreover, compared with CCTA, CMRA is not affected by the blooming artifacts from calcification.NCMRA have been widely used for coronary MRA, and their high diagnostic accuracy for the detection of significant coronary arterial disease (CAD) has been reported [3-4]. In addition, the previous report suggested the usefulness of single breath-hold NCMRA with turbo field echo (TFE) technique [5-6]. They reported that the single-breath hold technique could shorten the total scan time(Scanning time: approximately 18S) and reduce the influence of respiratory motion. When inadequately suppressed, epicardial fat can obscure visualization of the coronary arteries. To produce a good quality depiction of coronary arteries, modified-Dixon (3D-mDixon) has been used to suppress fat tissue for CMRA. 3D-mDixon compressed SENSE NCMRA is a promising noninvasive and radiation-free technique to detect clinically significant coronary stenosis at 3.0 T in patients with suspected CAD[7]. We aimed to investigate the feasibility of the whole heart NCMRA using a single breath-hold TFE EPI sequence at 3T MRI under compression SENSE (CS 4) in healthy volunteers.Materials and Methods
This study was approved by the institutional review board, and all participants gave written informed consent.The 22 healthy volunteers all underwent whole heart NCMRA examination on a 3.0T MR scanner (Ingenia Elition, Philips, Netherland) with two sequenceS : a 3D -mDixonTFE based on a certain compression acceleration factor of compressed SENSE 4 (CS4) and a TFE-EPI sequence(Table 1). Images were analyzed subjectively and objectively analysis: Objective analysis was performed by measuring the CR values of the image separately for the two sequences. Subjective analysis was performed by scoring the images for image quality for both sequences. Two experienced radiologists (with more than 5 years of experience in CMR) were blinded to assess CMRA independently. For vessels with a score of 2 and above, a region of interest (ROI) was drawn on the same plane vessel section and interventricular septum. The signal contrast (CR) between coronary and myocardial was assessed and calculated as \mu_{tissue1} where and \mu_{tissue2} are the ROI - based mean signal intensities of 2 specific tissues , with \sigma_{tissue1} and \sigma_{tissue2} as the corresponding variances. A different diagnosis between the two radiologists was solved with consensus reading. We used a 4-point subjective scale for qualitative image analysis: 4, excellent (vessel well depicted with sharply defined borders); 3, good (vessel adequately visualized with only mildly blurred borders); 2, fair (coronary vessel visible, but low confidence in the diagnosis due to moderately blurred borders); and 1, poor (coronary vessel barely seen or obscured by noise)(Fig.1). We subdivided the RCA into 3 segments (proximal, middle), the LAD into 3 segments (main, proximal, and middle), and the LCX into 2 segments (proximal and middle). We defined these segments as follows: #1 (in AHA, same as the following), RCA proximal; #2, RCA middle;#5, LAD main; #6, LAD proximal; #7, LAD middle; #11, LCX proximal; and #13, LCX middle. All image quality assessments were based on source images in axial orientation. (Fig.1).We adopted the image score of reader 1 and compared inter-observer agreement with reader 2.Results
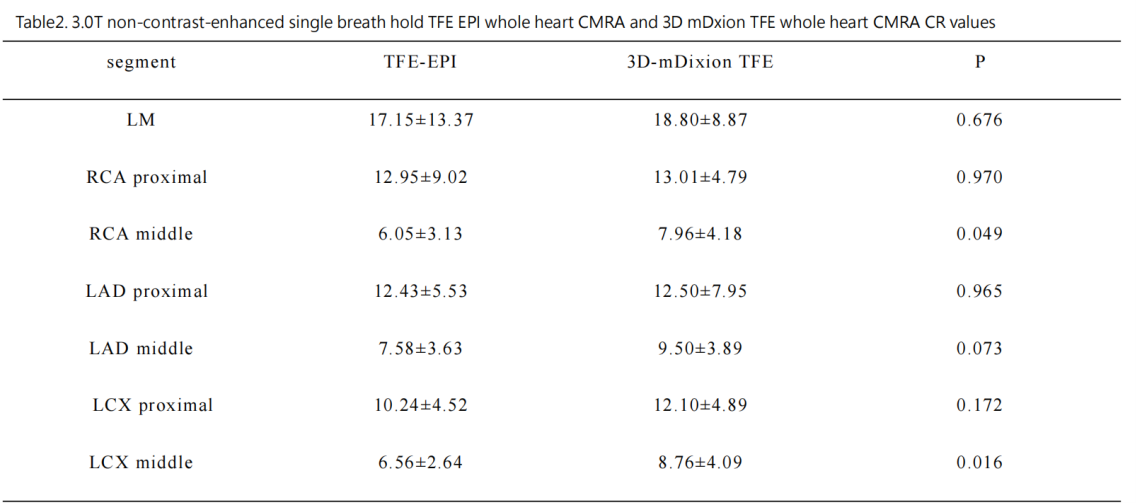
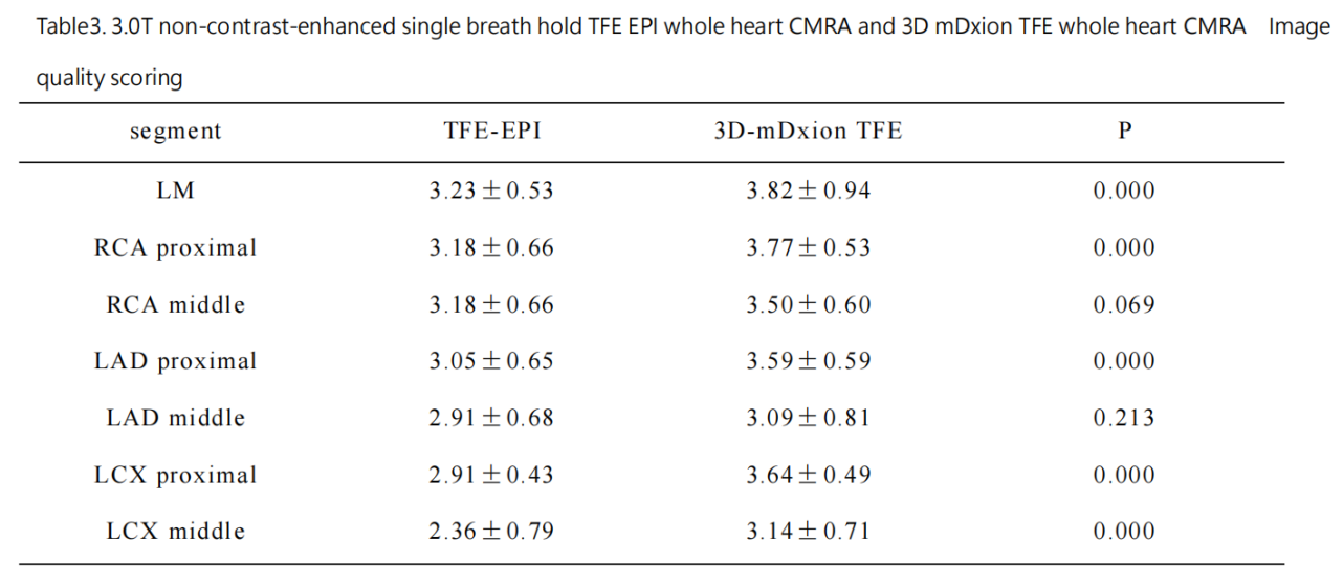
Twenty-two patients were included in this study. The objective score of image quality by 3.0T non-contrast-enhanced single breath hold TFE-EPI whole heart CMRA was 4 points (32 segments 20.78% ), 3 points (88 segments 57.14%), 2 points (32 segments 20.78%), 1 point (2 segments 1.3%). The objective score of image quality by 3D-mDixon TFE whole heart NCMRA has subjectively scored 4 points (89 segments 57.78%), 3 points (51 segments 33.12%), 2 points (51 segments 33.2%), 1 point (0 segments 0%) points. 3.0T non-contrast-enhanced single breath hold TFE EPI whole heart CMRA and 3D mDixon TFE had the differences between the middle RCA and the middle LCX segments in the objective score of whole heart CMRA coronary arteries. They were statistically significant (P < 0.05), while the remaining segments were not(Table 2). 3.0T nonenhanced single breath hold TFE EPI whole heart CMRA and 3D- mDixon whole heart CMRA coronary objective scores were statistically significant (P < 0.05) except for the RCA middle segment, LAD middle segment (Table 3).Discussion & Conclusion
The main findings of our study could be summarized as follows: (1) the 3T nonenhanced single breath hold TFE-EPI sequence had a significantly shorter scan time than the 3D -mDixon TFE for whole heart NCMRA scanning(18s VS 5-8 minutes), which might reduce the respiratory motion artifacts. (2) In the objective evaluation, the 3T non-enhanced single breath hold TFE EPI sequence and 3D-mDixon TFE sequence did not show a difference in image contrast between the LM,RCA proximal , LAD proximal. (3) In subjective evaluation, the 3D mDixon TFE sequence had higher image quality scores than that of the single breath-hold TFE-EPI sequence in the left main trunk and proximal coronary artery. Thery were no statistically significant differences in the left anterior descending segment and middle left circumflex artery.It might show that the single breath-hold TFE-EPI sequence might have its own unique advantages in these segments(For example, patients with poor breath holding)(Fig 2). The sample size in this study was small and further studies need to expand the sample size further to explore.Acknowledgements
No acknowledgement found.
References
1 Kim WY, Danias PG, Stuber M, et al.Coronary magnetic resonance angiography for the detection of coronary stenoses[J]. N Engl J Med.2001;345(26):1863-9.
2 Schuijf JD, Bax JJ, Shaw LJ, et al Meta analysis of comparative diagnostic performance of magnetic resonance imaging and multislice computed tomography for noninvasive coronary angiography[J]. Am Heart.2006;151(2):404-411.
3 Kato S, Kitagawa K, Ishida N, et al Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial[J]. J Am Coll Cardiol, 2010;56(12): 983-991.
4 He Y, Pang J, Dai Q, et al Diagnostic performance of self navigated whole heart contrast enhanced coronary 3T MR angiography[J]. Radiology, 2017;283(3):923.
5 Iyama Y , Nakaura T , Kidoh M, et al Single-breath-hold whole-heart coronary MRA in healthy volunteers at 3.0-T MRI. Springerplus 2014;3:667.
6 Yuji Iyama, Takeshi Nakaura, Y asunori Nagayama, et al Single-Breath-Hold Whole-heart Unenhanced Coronary MRA Using Multi-shot Gradient Echo EPI at 3T: Comparison with Free-breathing Turbo-field-echo Coronary MRA on Healthy Volunteers[J].Magn Reson Med Sci 2018;17:161–167 .
7 Hongfei Lu, MDy, Jiajun Guo, MDy, et al .Assessment of Non-contrastenhanced Dixon Water-fat Separation Compressed Sensing Whole-heart Coronary MR Angiography at 3.0 T: A Single-center Experience[J].Academic Radiology,Acad Radiol,2022 ;29 Suppl 4:S82-S90.
Figures
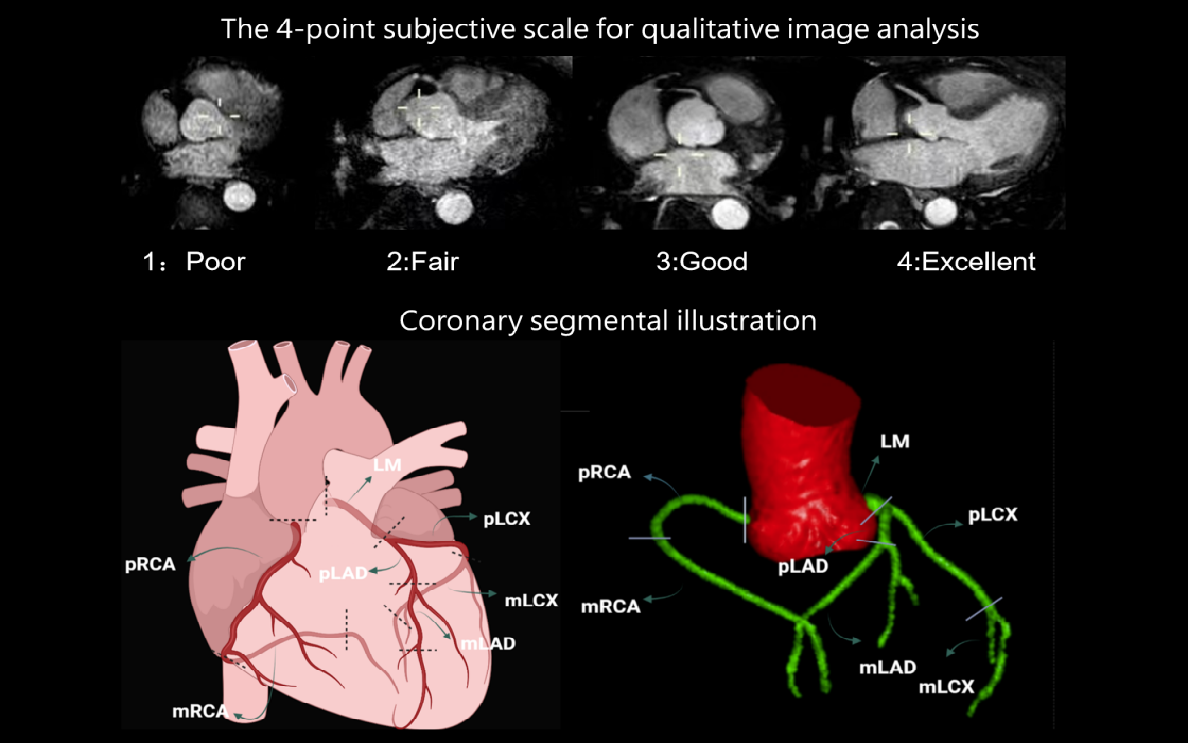
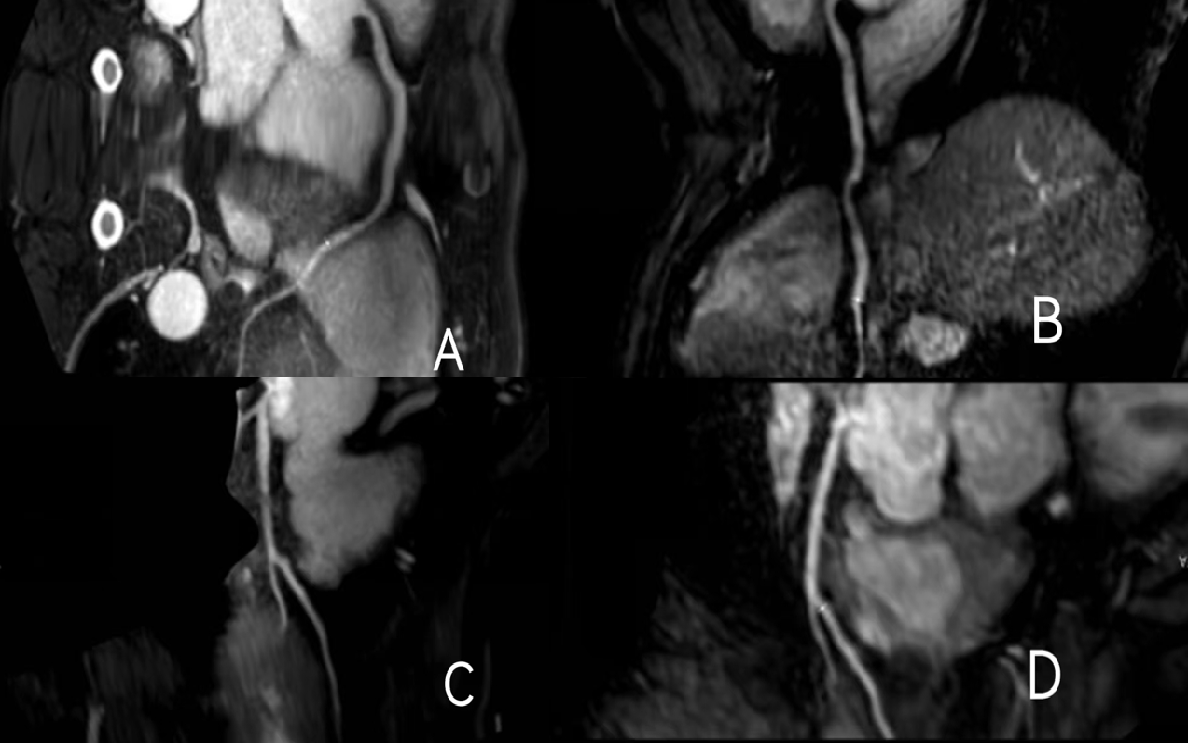
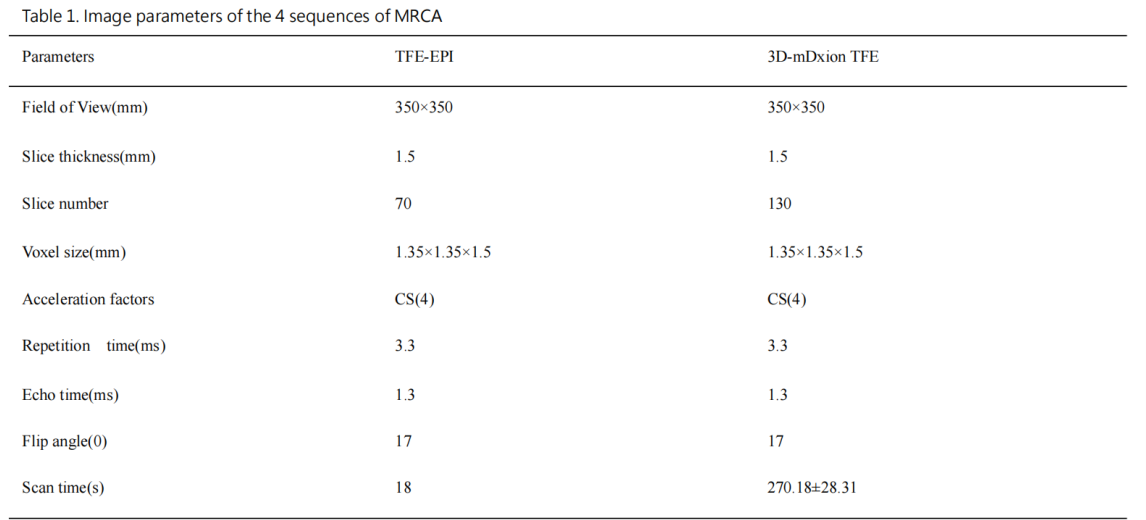
Image parameters of the 4 sequences of MRCA
Data are presented as mean±SD for normally distributed continuous variables, and median (interquartile range) for non-normally distributed continuous variables.
Data are presented as mean±SD for normally distributed continuous variables, and median (interquartile range) for non-normally distributed continuous variables.