1600
Simultaneous multi-slice real-time cardiac MRI at 0.55T1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Division of Cardiology, Department of Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States
Synopsis
Keywords: Low-Field MRI, Low-Field MRI
A standard cine MRI exam typically collects a stack of short-axis slices to cover all left ventricular myocardium and uses electrocardiogram gating and breath-holds. Real-time imaging methods are often used to resolve issues with insufficient gating signal or breath-hold failure. In this work, we demonstrate that real-time SMS cardiac imaging at 0.55T provides sufficient blood-myocardium contrast and regional wall motion evaluation with three-fold acceleration compared to real-time single-band and Cartesian breath-hold ECG-gated cine. We also show an alternative reconstruction approach, clustered locally low rank that can improve image quality.Introduction
Cine cardiac MRI (CMR) is routinely used to evaluate ventricular function, wall motion, and regional wall thickening. It typically uses electrocardiogram (ECG) gating and breath-holds, which can result in compromised image quality for patients with arrhythmias, insufficient gating signal, or inability to comply with breath-hold instructions. Real-time CMR overcomes these issues as no gating or breath-holding is required. A standard CMR cine scan requires a stack of short-axis slices (~9-12 slices, sequentially) to fully evaluate the left ventricular (LV) myocardium. Simultaneous multi-slice (SMS) technique can accelerate the acquisition by a factor of 2-41-2. If more than 3 slices are simultaneously acquired this can provide simultaneous evaluation of 16 out of 17 cardiac segments.In this work, we show blipped-CAIPI bSSFP real-time SMS CMR provides sufficient blood-myocardium contrast and regional wall motion evaluation with three-fold acceleration at 0.55T compared to real-time single-band (SB) and Cartesian breath-hold ECG-gated cine images in four healthy volunteers, including one experiencing premature ventricular contraction (PVC) and two after a short period of exercise. Lastly, we show an alternative reconstruction approach, clustered locally low-rank (cLLR) that can improve overall image quality.
Methods
Data Acquisition:Real-time CMR was performed using a free-breathing blipped-CAIPI SMS bSSFP sequence combined with golden-angle spiral readout2-4. SMS factor was set to 3, and slices were prescribed in the short-axis orientation. Slice gap was set to 24mm to capture basal, mid, and apical sections of LV myocardium5. For comparison, SB real-time images corresponding to the same slice positions were acquired. Temporal resolution was set to 45ms for both.
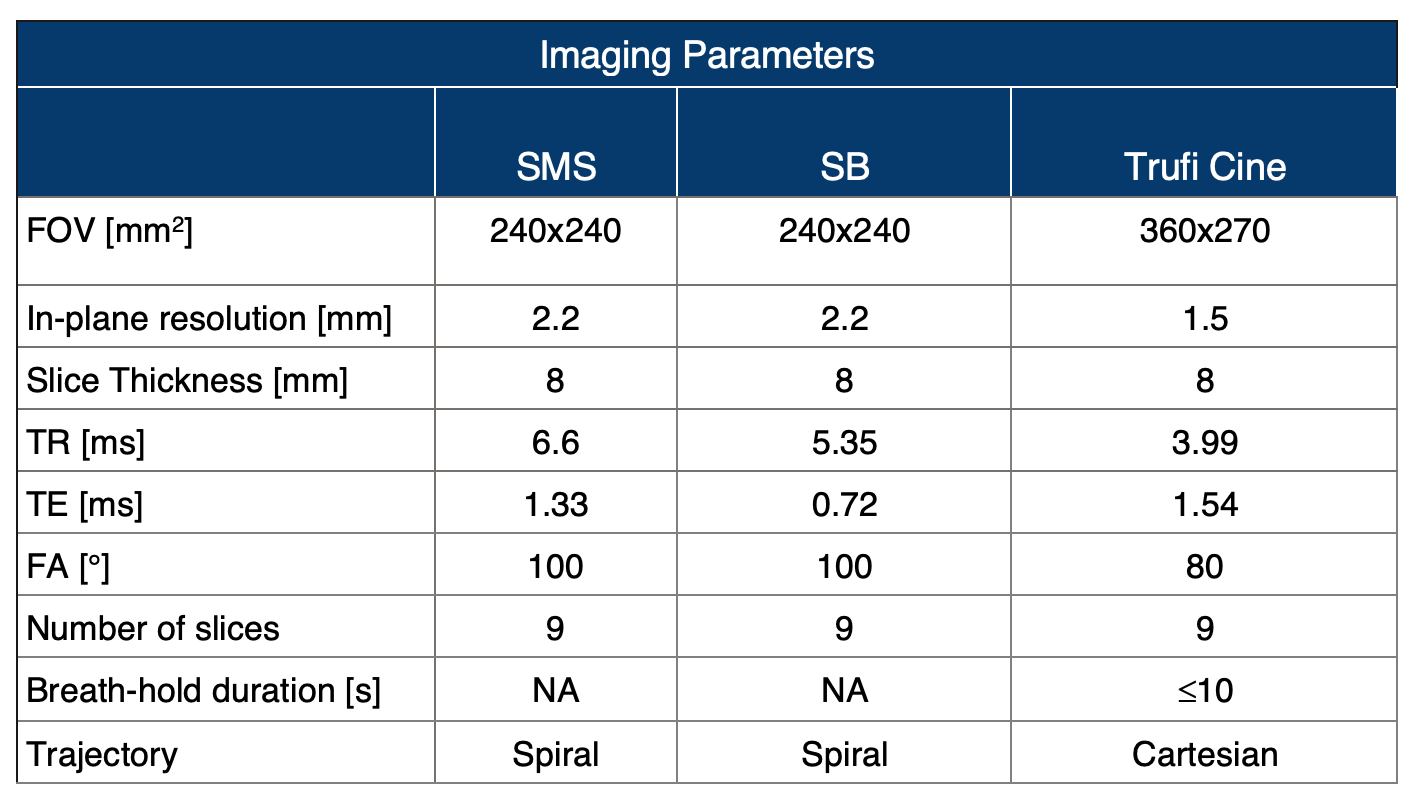
Experiments were performed on a 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers, Germany) equipped with high-performance shielded gradients (45mT/m amplitude, 200T/m/s slew rate)6. Real-time imaging was performed using RTHawk system (HeartVista Inc., CA)7. Four healthy volunteers (2F/2M, age 25±4) were scanned, after providing written informed consent, under a protocol approved by our Institutional Review Board. In two volunteers imaging was also performed after a short exercise using an in-bore cardio step-module (Ergospect, Austria). Breath-hold, ECG-gated Cartesian cine were acquired using product sequence, bSFFP Cine, available on scanner. For real-time imaging, a flip angle of 100o was experimentally chosen to maximize blood-myocardium contrast8. Imaging parameters are listed in Table1.
Reconstruction and Analysis:
Online reconstruction was used for Cartesian cine images. For real-time cine images (SB and SMS) a spatiotemporal constrained reconstruction (STCR)9 was used and for after-exercise images another approach, cLLR was implemented which solves the following optimization,
$$\arg\min_m\lVert Am-d\rVert^2_2+\lambda_t\left\lVert\sqrt{(\nabla_tm)^2+\epsilon}\right\rVert_1+\sum_{j=1}^{N}\sum_{i=1}^{K}\lambda_t\left\lVert\sqrt{\big(\nabla_t\mathcal{P}_{i,j}(m)\big)^2+\epsilon}\right\rVert_1+\sum_{j=1}^{N}\sum_{i=1}^{K}\lambda_*\left\lVert\mathcal{P}_{i,j}(m)\right\rVert_*$$ where $$$m$$$ is the image-series to be reconstructed, $$$A$$$ is encoding matrix, $$$d$$$ is multi-coil k-space data, $$$\lVert.\rVert_*$$$ is nuclear norm, $$$\mathcal{P}_{i,j}$$$ is an operator that forms dynamic image-series $$$m$$$ into $$$N$$$ patches ($$$n_x\times n_y\times t$$$), and divides each patch into $$$K$$$ clusters along $$$t$$$, where 2D patches ($$$n_x\times n_y$$$) within a cluster have similar motion state. Lastly, $$$\lambda_t$$$ and $$$\lambda_*$$$ are the temporal and locally low-rank regularization parameters. The cost function was solved by an ADMM algorithm. Both reconstructions used gradient impulse response function corrected spiral trajectory10. Parameter selection was performed qualitatively for SCTR (spatial and temporal regularization), and heuristically for cLLR (number of clusters $$$K$$$, regularization terms $$$\lambda_t$$$, $$$\lambda_*$$$, patch size $$$n_x,n_y$$$ ) in a small range of values. Analysis was performed qualitatively.
Results
Figure1 compares real-time SMS and SB images to breath-hold ECG-gated Cartesian cine images. SMS images provide sufficient blood-myocardium contrast and regional wall motion evaluation with three-fold acceleration, however, there is relatively low distinction between the lateral wall and the lung cavity compared to SB images and Cartesian cine images.Figure2 shows SMS and SB real-time images of a volunteer experiencing PVCs during the study. Irregular beats are highlighted in line-intensity plots. In SMS images, PVC is captured in apical, mid, and basal short-axis slices at the same time without synchronization.
Figure3 shows SMS real-time images using STCR reconstruction in resting-state and after-exercise. Resting-state images with different heartbeats in (a) and (c) show that reconstruction is agnostic to the heartbeat. However, image quality degrades in (b) after-exercise images, suggesting increased physiological motion (heartbeat, respiratory, etc.) cannot be recovered with this approach alone.
Figure4 shows a comparison of STCR and cLLR reconstructions on SMS real-time using the same volunteer data in resting and after-exercise. While STCR gives acceptable image quality for resting-state, initial results suggest that cLLR can possibly elevate image quality for both resting-state and exercise.
Discussion
SMS real-time image quality was acceptable and could capture wall motion during irregular heartbeats in 16 (out of 17) myocardial segments simultaneously. There was relatively low distinction between the lateral wall and the lung cavity, making it more challenging to evaluate lateral segments. It has been demonstrated that the STCR can be used for SMS real-time imaging, and this approach is agnostic to the cardiac rhythm. However, the range of physiological motion that can be recovered with this reconstruction is shown to be limited. cLLR can possibly address these issues and improve the distinction in the lung cavity and recover increased physiological motion.Conclusion
Real-time SMS CMR at 0.55T provides sufficient blood-myocardium contrast and regional wall motion evaluation with three-fold acceleration at 0.55T compared to real-time SB and Cartesian breath-hold ECG-gated cine. Further investigation is needed to determine diagnostic confidence.Acknowledgements
We acknowledge funding from the National Institutes of Health (R21-HL159533), American Heart Association (#903839), and National Science Foundation (#1828736), and research support from Siemens Healthineers. We thank Andrew Cheng for lending us the in-bore cardio step module, and Mary Yung for research coordination.References
1. Nazir
MS, Neji R, Speier P, et al. Simultaneous multi-slice (SMS) balanced steady-state free precession first-pass myocardial perfusion cardiovascular magnetic
resonance with iterative construction at 1.5 T.J Cardiovasc Magnetic Resonance.
2018;20:84.
2. Price AN, Cordero-Grande L, Malik SJ, Hajnal JV. Simultaneous multislice imaging of the heart using multiband balanced SSFP with blipped-CAIPI. Magnetic Resonance in Medicine. 2020;83(6):2185-2196. doi:10.1002/mrm.28086
3. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An Optimal Radial Profile Order Based on the Golden Ratio for Time-Resolved MRI. IEEE Trans Med Imaging. 2007;26(1):68-76. doi:10.1109/TMI.2006.885337
4. Feng L. Golden-Angle Radial MRI: Basics, Advances, and Applications. Journal of Magnetic Resonance Imaging. 56: 45-62. doi:10.1002/jmri.28187
5. Cerqueira MD, Weissman NJ, et al. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart. Circulation. 2002;105(4):539-542. doi:10.1161/hc0402.102975
6. Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
7. Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med BiolSoc. 2004;2004:1048-1051
8. Tian Y, Cui SX, Lim Y, Lee NG, Zhao Z, Nayak KS. ‘Contrast-optimal simultaneous multi-slice bSSFP cine cardiac imaging at 0.55 Tesla’. Magnetic Resonance in Medicine.
9. Tian Y, Mendes J, Pedgaonkar A, Ibrahim M, Jensen L, Schroeder JD, Wilson B, DiBella EVR, Adluru G. Feasibility of multiple-view myocardial perfusion MRI using radial simultaneous multi-slice acquisitions. PLoS One 2019;14(2):e0211738.
10. Campbell-Washburn AE, Xue H, Lederman RJ, Faranesh AZ, Hansen MS. Real-time distortion correction of spiral and echo planar images using the gradient system impulse response function. Magnetic Resonance in Medicine. 2016;75(6):2278-2285. doi:10.1002/mrm.25788
11. Tian, Y. et al. (2021) ‘Aliasing artifact reduction in spiral real-time MRI’, Magnetic Resonance in Medicine, 86(2), pp. 916–925. Available at: https://doi.org/10.1002/mrm.28746.
Figures