1596
Multi-reader evaluation of real-time MRI of the actively moving wrist at 0.55 Tesla1Radiology, University of California Davis, Sacramento, CA, United States, 2Radiology, Stanford University, Palo Alto, CA, United States, 3University of Southern California, Los Angeles, CA, United States, 4Siemens Medical Solutions, Malvern, PA, United States, 5Orthopaedic Surgery, University of California Davis, Sacramento, CA, United States
Synopsis
Keywords: Joints, Skeletal, Real-time imaging; Wrist Kinematics; Dynamic imaging.
We acquired real-time MRI of the actively moving wrist in humans utilizing a high-performance 0.55T system. Resulting images and associated static wrist scans were assessed by two expert readers blinded to acquisition parameters. Our results show that images acquired at a high temporal resolution of 12.6 ms per frame demonstrate minimal image degradation compared to images acquired at temporal resolution of 100 ms or higher, and enable improved characterization of wrist motion. These benefits support further studies to assess high-performance 0.55T systems for the evaluation of dynamic dysfunction of the wrist.Introduction
MRI is commonly employed in the evaluation of wrist pathology, with assessment relying primarily on static scans [1, 2]. In previous work we demonstrated the utility of 3T MRI for imaging the actively moving wrist to overcome shortcomings of the static scans for assessing wrist kinematics [3, 4]. However, image artifacts arising from the relatively slow acquisition rate and magnetic field susceptibility frequently obscured critical wrist structures [3, 5]. To address these limitations, we conducted a human study utilizing a high-performance 0.55T system for obtaining real-time (RT) scans of the actively moving wrist and static scans of the wrist in the neutral position. The resulting images were evaluated by two expert readers independently, providing qualitative and quantitative assessments of image quality and specific imaging features of interest for assessing wrist dysfunction.Methods
Scan were performed using a whole body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate). The study cohort consisted of 5 participants (3 men and 2 women, median age (range) = 46 (31-59) years). The dominant wrist for each participant was scanned. Participants lay in the “superman position” with one arm placed on spine RF coil (below) and 6-channel surface coil (above), in a configuration that did not restrict wrist range of motion. Using the localizer acquisition, a coronal slice showing the scapholunate (SL) interval was prescribed. Each participant performed two wrist maneuvers (radial/ulnar deviation and the clenched fist maneuver) during RT-MRI acquisition utilizing their full, active range-of-motion at a natural speed. These maneuvers are of significance in the evaluation of dynamic wrist dysfunction. A 2D spiral balanced steady-state free-precession (bSSFP) sequence was implemented within the RTHawk real‐time imaging platform (HeartVista, Inc., Los Altos, CA, USA). Imaging parameters were: in-plane resolution = 1.38x1.38 mm2, slice thickness = 8 mm, field-of-view = 18x18 cm2, TR / TE= 12.70/0.78 ms, readout duration = 8.38 ms, sampling interval = 2 µs, flip angle = 70º. Thirteen spiral-out sampling scheme and temporal bit-reversed orders of spiral interleaves was used. Localization, imaging, and reconstructions were performed using the real-time console while MRI data were analyzed from off-line reconstructed images. The temporal finite-difference constrained reconstruction implemented using the Berkeley Advanced Reconstruction Toolbox was used. For static imaging of the immobilized wrist in the neutral position, the acquisition involved a T1-weighted 3D pulse sequence with voxel size: 0.61×0.61×0.60 mm3, and 2D proton-density weighted (coronal) and T1-weighted (coronal and axial) turbo spin echo acquisitions with in-plane resolutions of 0.31×0.31 and 0.25×0.25 mm2, and slice thicknesses of 2.50 and 3.00 mm, respectively. The RT images were assessed by two experienced readers, a fellowship-trained musculoskeletal radiologist with 25 years of post-training experience, and a PhD scientist with expertise in musculoskeletal kinematics and wrist imaging for 15 years, independently. First, the readers scored the images based on a 5-point Likert scale (1: ‘extremely poor’; 2: ‘poor’; 3: ‘average’; 4: ‘good’; and 5: ‘excellent’) [6]. Second, two imaging features, the SL and the capitotriquetral (CT) interval, were evaluated from the images. The scoring was based on a 3-point scale: (1: not visualized, 2: visualized but not well-defined, and 3: well-defined [7]). The static scans were assessed based on the same 5-point Likert and 3-point scales. Further, visualization of joint distention, sharpness of joint borders, and the ability to assess triangular fibrocartilage complex (TFCC) tears was evaluated. Each of these factors was graded poor, fair, good or very good based on criteria described by Andreisek et al [8].Results
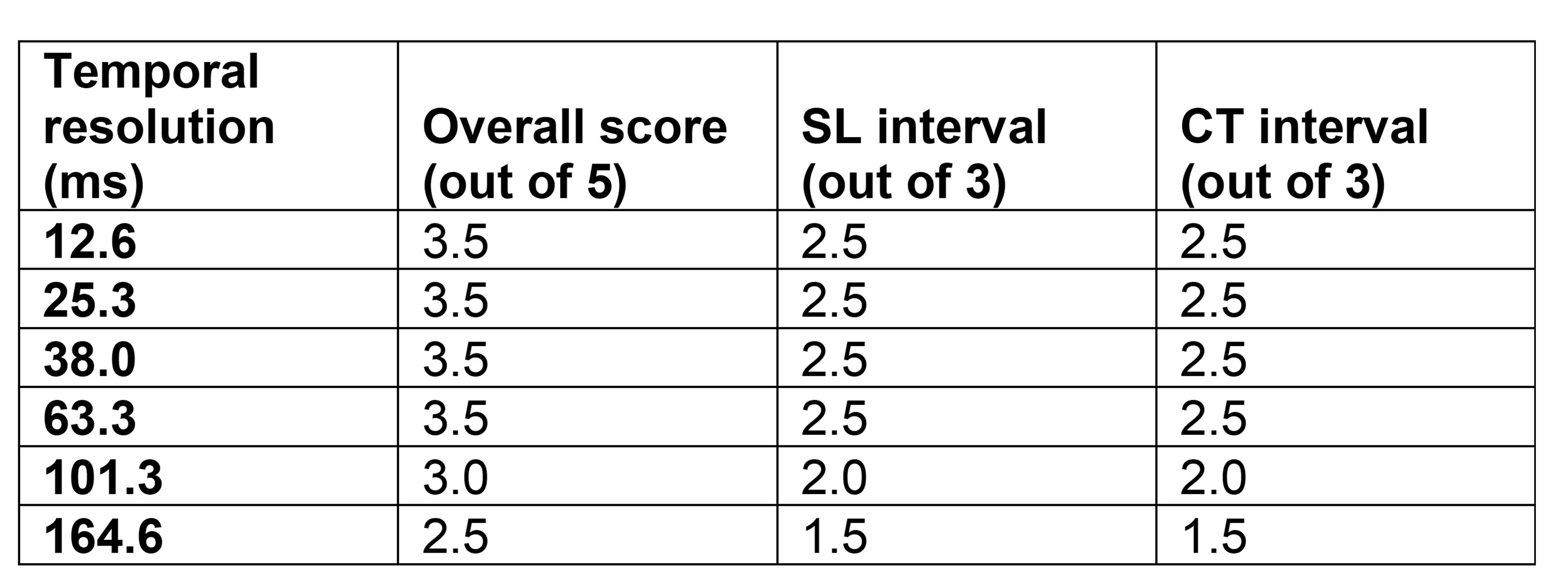
From static images, the wrist bones were visualized clearly in the T1-weighted acquisition (Figure 1). The proton density-weighted acquisition demonstrated TFCC anatomy and the SL ligament (Figure 1). All static scans were rated good to very good and diagnostic. For the radial-ulnar deviation maneuver, reader scores of RT-MRI scans with temporal resolution of less than 100 ms were higher than those with temporal resolutions greater than 100 ms (p<0.05), Table 1. For the clenched fist maneuver, however, there were no differences in reader scores with changes in temporal resolution. With finer temporal resolution, images showed reduced motion blurring and a sharper boundary between the scaphoid and lunate or capitate and triquetrum, indicating an improved ability to quantify changes to the SL and CT interval over the range of motion (Figures 2, 3). Furthermore, visualization of the changes in the SL and CT interval with temporal resolution down to 12.6 ms was possible with minimal degradation in image quality during the wrist maneuvers.Discussion and Conclusions
Our results demonstrate the feasibility of a high-performance 0.55T MRI system in assessing tissues of the moving wrist during the performance of a wrist maneuvers relevant to wrist dysfunction. Images down to a temporal resolution of 12.6 ms showed minimal degradation in image quality compared to images with temporal resolutions of greater than 100 ms and allowed improved visualization of joint motion. These benefits combined with other advantages of low-field imaging make it a promising technology to evaluate further for assessing wrist biomechanics and dynamic dysfunction. Future studies will include more subjects with and without wrist pathology and evaluation of 0.55T-specific acquisition strategies for the moving wrist.Acknowledgements
We acknowledge grant support from the National Science Foundation (#1828736) and research support from Siemens Healthineers.References
[1] R. L. Leake, M. K. Mills, H. Allen, A. M. Crawford, P. H. Kobes, and M. Soltanolkotabi, "MRI of the Wrist Ligaments," Topics in Magnetic Resonance Imaging, vol. 29, no. 5, pp. 209-220, 2020.
[2] C. A. Tiegs-Heiden and B. M. Howe, "Imaging of the Hand and Wrist," Clinics in Sports Medicine, vol. 39, no. 2, pp. 223-245, 2020.
[3] R. D. Boutin et al., "Real-time magnetic resonance imaging during active wrist motion--initial observations," PLoS One, vol. 8, no. 12, p. e84004, 2013.
[4] S. S. Henrichon et al., "Dynamic MRI of the wrist in less than 20 seconds: normal midcarpal motion and reader reliability," Skeletal Radiol, vol. 49, no. 2, pp. 241-248, Feb 2020.
[5] C. B. Shaw et al., "Real-time three-dimensional MRI for the assessment of dynamic carpal instability," PLoS One, vol. 14, no. 9, p. e0222704, 2019.
[6] S. Partovi et al., "Image quality assessment of automatic three-segment MR attenuation correction vs. CT attenuation correction," (in eng), Am J Nucl Med Mol Imaging, vol. 3, no. 3, pp. 291-9, 2013.
[7] S. D. Sharma, C. L. Fong, B. S. Tzung, M. Law, and K. S. Nayak, "Clinical image quality assessment of accelerated magnetic resonance neuroimaging using compressed sensing," Investigative Radiology, vol. 48, no. 9, pp. 638-645, 2013.
[8] G. Andreisek, S. R. Duc, J. M. Froehlich, J. Hodler, and D. Weishaupt, "MR arthrography of the shoulder, hip, and wrist: evaluation of contrast dynamics and image quality with increasing injection-to-imaging time," AJR Am J Roentgenol, vol. 188, no. 4, pp. 1081-8, Apr 2007.
Figures