1592
Portable MRI for major sporting events – a case study on the MotoGP World Championship1Tesoro Imaging SL, Valencia, Spain, 2Institute for Instrumentation in Molecular Imaging (i3M), Universitat Politècnica de València, Valencia, Spain, 3Institute for Instrumentation in Molecular Imaging (i3M), CSIC, Valencia, Spain, 4Physio MRI SL, Valencia, Spain
Synopsis
Keywords: Low-Field MRI, Low-Field MRI, Portable MRI, Sport event MRI
Here we study the potential MR value of a low-field portable system for use in major sporting events, specifically in the Motorcycle Grand Prix held in Valencia (Spain) between November 3rd and 6th, 2022. The system was transported in a small truck, installed in the main surgery room of the circuit medical facilities, and operational around 30 minutes after arrival. Overall, 15 subjects were scanned in four days, with a total of 21 extremity acquisitions. This work demonstrates that portable MRI machines can aid the diagnostic capabilities of medical staff in sporting events and competitions.Introduction
Low-field MRI scanners can be designed to be low cost and small footprint, since the main evolution field B0 can be generated by permanent or resistive, rather than superconducting, magnets [1]. Yokeless magnets furthermore allow for lightweight and portable designs [2]. The scope of applications enabled by truly portable MRI technologies is immense and largely unexplored. These include: new in-hospital functionalities [3], such as bedside and point-of care scans, outpatient services, in emergency rooms, intensive care units, etc.; out-of-hospital scans [4], such as for residential and hospice care, small clinics, rural areas, penitentiaries, sports clubs, school facilities, etc.; and outdoor applications [5], e.g. in field hospitals, NGO and military camps, sports events, etc.We recently demonstrated the capabilities of a new low-field extremity scanner, designed to be extremely portable and which was used indoors, outdoors and for the first time at a patient’s residence [5,6]. In this work we study the potential MR value of this system for use in major sporting events, specifically in the Motorcycle Grand Prix held in the Ricardo Tormo Racing Circuit in Valencia (Spain) between November 3rd and 6th, 2022.
Methods
The portable scanner (Fig. 1, [5]) is based on a Halbach magnet made with a discrete array of around 5,000 NdFeO magnets, generating a B0 of around 72 mT homogeneous down to 3,000 ppm over a spherical field of view of 20 cm and 75 ppm for 10 cm. The complete system, including electronics and the wheeled mounting structure, weighs < 250 kg and runs from a standard wall power outlet.The system was transported in a small truck, installed in the main surgery room of the circuit medical facilities, and operational around 30 minutes after arrival. Overall, 15 subjects were scanned in four days, including racers (1), track marshals (2), medical staff (4), safety car drivers (1), helicopter pilots (1), event organization staff (1), race control staff (1) and engineers (4). We acquired 3D RARE images (T1-weighted and STIR) of the subjects’ wrists (1 injured, 4 healthy), knees (6 injured, 4 healthy) and ankles (3 injured, 3 healthy), for a total of 21 acquisitions. All subjects were adults and provided written informed consent for this study. Ethical approval was obtained from the Ethics Committee (CEIm) of La Fe Hospital in Valencia (CEIm-F-PE-01-16, research agreement number 2022-187-1).
Results
Wrist scans. A subject who had suffered an accident two weeks before the race reported pain in their right wrist. Following the established protocols, they were subject to an X-ray radiograph (Fig. 2c), which revealed no lesion. They were then scanned in our low-field system, where a 3D T1-weighted RARE acquisition also showed no anomaly (Fig. 2a), but the STIR scan featured a bright volume between the scaphoid, trapezium and trapezoid bones (Fig. 2b), indicating a possible synovitis as judged by the traumatologist in charge at the medical center. For comparison, we scanned the right wrists of four healthy volunteers. None of them showed a bright region between the wrist bones (Fig. 2d).Knee scans. We scanned six knees with different pathologies, some of them diagnosed before the MotoGP event. The circuit medical staff were able to identify a bone marrow edema in one of them, gonarthrosis in another, the results of an intervention on the cruciate ligaments on another (Fig. 3a), and a Baker cyst on another. Nothing was apparent on the remaining two acquisitions, one performed on a patient with a meniscus fracture on the right knee (previously diagnosed on a 1.5 T scanner), the other on a patient reporting pain but so far undiagnosed. Besides, we scanned four healthy knees, which showed no anomalies on our reconstructions.
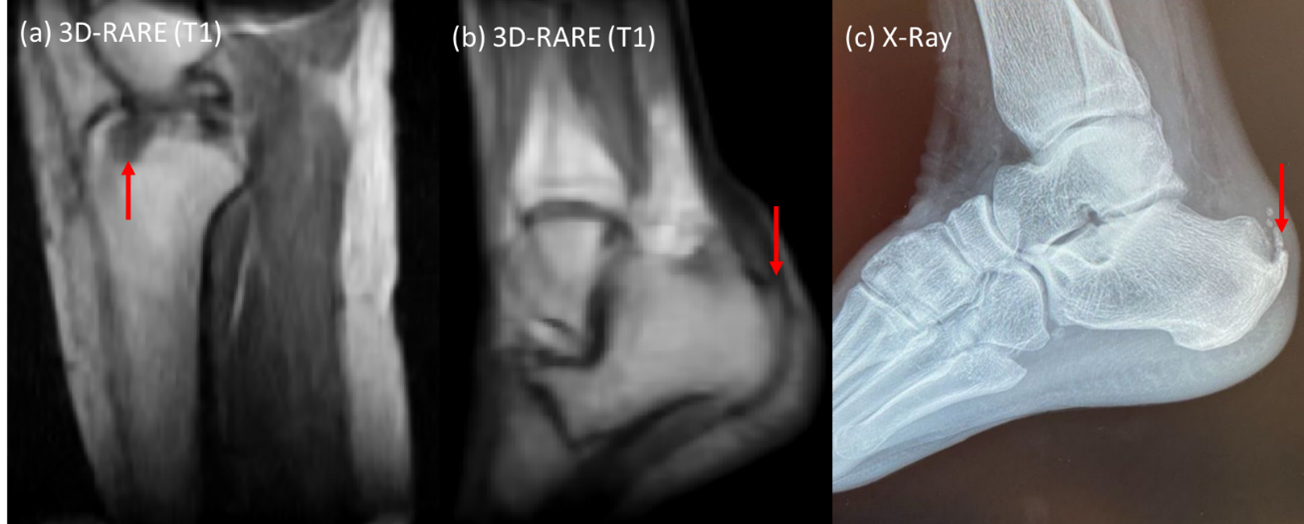
Ankle scans. We scanned three injured and three healthy ankles. Two injuries were diagnosed as Haglund’s deformities and visible in our low-field scans by the circuit medical staff (Fig. 3b-c). The last injury was due to a bone fracture which had been previously operated and fixed with metallic screws and plates. This was also apparent in our MRI reconstructions.
Discussion/Conclusion
This work demonstrates that portable MRI machines can aid the diagnostic capabilities of medical staff in sporting events and competitions. Out of eight low-field acquisitions on previously diagnosed lesions, only one was not detected by the circuit experts that evaluated our images. This corresponds to a meniscus fracture, which may require higher spatial resolution than we currently achieve. Furthermore, we were able to detect a synovitis in the wrist which would have otherwise gone unnoticed to the MotoGP medical staff. Finally, no anomalies were detected in the scans performed on reportedly healthy volunteers.Acknowledgements
We acknowledge all anonymous volunteers for their participation, and Dr. MD Enrique Gastaldi, MD Vicente Vila and MD Ángel Charte for evaluating the low-field reconstructions. This work was supported by the Ministerio de Ciencia e Innovación of Spain (PID2019-111436RBC21), the European Union (IDIFEDER/2021/004), Generalitat Valenciana (CIPROM/2021/003) and Agència Valenciana de la Innovació (INNVA1/2022/4).References
[1] Marques, José P., Frank F.J. Simonis, and Andrew G. Webb, ‘Low‐field MRI: An MR Physics Perspective’, Journal of Magnetic Resonance Imaging, 49 (2019), 1528–42
[2] O’Reilly, Thomas, Wouter M. Teeuwisse, Danny Gans, Kirsten Koolstra, and Andrew G. Webb, ‘In Vivo 3D Brain and Extremity MRI at 50 MT Using a Permanent Magnet Halbach Array’, Magnetic Resonance in Medicine, 2020, mrm.28396
[3] Sheth, Kevin N., Mercy H. Mazurek, Matthew M. Yuen, Bradley A. Cahn, Jill T. Shah, Adrienne Ward, and others, ‘Assessment of Brain Injury Using Portable, Low-Field Magnetic Resonance Imaging at the Bedside of Critically Ill Patients’, JAMA Neurology, 78 (2021), 41–47
[4] Deoni, Sean C.L., Paul Medeiros, Alexandra T. Deoni, Phoebe Burton, Jennifer Beauchemin, Viren D’Sa, and others, ‘Development of a Mobile Low-Field MRI Scanner’, Scientific Reports 2022 12:1, 12 (2022), 1–9
[5] Guallart-Naval, Teresa, José M. Algarín, Rubén Pellicer-Guridi, Fernando Galve, Yolanda Vives-Gilabert, Rubén Bosch, and others, ‘Portable Magnetic Resonance Imaging of Patients Indoors, Outdoors and at Home’, Scientific Reports 2022 12:1, 12 (2022), 1–11
[6] Guallart-Naval, Teresa, Thomas O’reilly, José M Algarín, Ruben Pellicer-Guridi, Yolanda Vives-Gilabert, | Lincoln Craven-Brightman, and others, ‘Benchmarking the Performance of a Low-Cost Magnetic Resonance Control System at Multiple Sites in the Open MaRCoS Community’, NMR in Biomedicine, 2022, e4825
Figures