1562
A Cohort Study of Spinal Cord Diffusivity After Treatment of Cervical Spondylotic Myelopathy with Instrumented Spinal Fusion
Kevin Koch1 and Andrew S Nencka1
1Radiology, Medical College of Wisconsin, Milwaukee, WI, United States
1Radiology, Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
Keywords: Spinal Cord, Spinal Cord
This study analyzed spinal cord diffusivity in CSM subjects treated with metallic spinal fusion decompression. Metal-artifact-suppressed diffusion-weighted MRI were collected on 38 CSM subjects and 25 controls. Diffusivity was analyzed as a function of cohort and level instrumentation (instrumented, non-instrumented, and adjacent segment). In addition, the impact of mJOA symptom scores and duration since the fusion procedure on diffusivity were modeled. Multi-linear mixed effects models accounted for demographic variations and multiple-measures (at different cord levels) within each subject. The results of the study identified consistent reductions in diffusivity due to the presence of fusion instrumentation.Introduction
Cervical spondylotic myelopathy (CSM) of the spinal cord is the most common cause of spinal dysfunction in adults [1]. CSM is the result of degenerative wear and stress on the spinal cord and is often treated with metallic hardware used to decompress the spinal cord. The present study provides the first large-cohort post-treatment diffusion MRI analysis of CSM patients treated with such instrumented decompression procedures.Study Hypotheses:
- Routine decompression using metallic instrumentation reduces diffusivity relative to controls and non-instrumented levels in CSM subjects.
- Diffusivity measures within the spinal cord with track with post-surgical symptom score measures.
Methods
Subjects:1. Post-surgical CSM (n=38) treated with metallic instrumented fusion.
- Imaged between 3 and 36 months post-surgery.
- No other known spinal cord disease or injury.
- Symptoms were recorded using Modified Japanese Orthopaedic Association Scale (mJOA) assessment [2].
- Characteristics: male/female: 19/19, age: 59.3+/-3.6, BMI: 29.5+/-1.7, MJOA: 14.5+/-1.0, time post-operation: 17.8+/-3.4 months2)
- Adults with no known spinal cord disease, injury, or symptoms.
- Characteristics: male/female: 12/13, age: 56.4+/-2.2, BMI: 28.3+/-2.7
MRI Evaluation:
MRI was performed at 3 Tesla on a 70 cm bore high-performance clinical imaging platform. A 21-channel vendor-provided head-neck-unit was utilized for signal reception. T1 and T2 weighted 3D-Multi-Spectral Images (3D-MSI) [3] were utilized for metal-artifact suppressed morphological imaging. 3D-MSI were collected with 1.2 mm isotropic resolution, using 2x2 auto-calibrated parallel imaging, echo times of 8/60 ms, and repetition times of 0.8/2.5 s for respective T1/T2 weighted image acquisitions.
A prototype 2D-MSI PROPELLER-based diffusion weighted (DW) sequence (DW-MSI) [4] and commercially available reduced field-of-view single-shot echo-planar DW method were utilized for diffusion-measurements of the spinal cord. With both methods, axially oriented slice packages of 3 to 5 mm slices were collected at 3 stations spanning the cervical spine at 2.5mm x 2.5mm in plane resolution, using echo times of 56 ms and repetition times of 4s . A single b=0 image was acquired and 3 orthogonal diffusion-weighted images were acquired with a b-value of 600 m/s2. A total of 822 axial cord measures were collected across C1-C7/T1 in the 38 CSM and 25 control subjects.
Statistical Analysis:
After cord segmentation utilizing the open-source Spinal-Cord Toolbox [5], apparent diffusion coefficient (ADC) values of the cord were computed using mono-exponential models, then statistically modeled as a function of cohort (i.e. CSM vs control), vertebral level, decompressed (instrumented) level (yes/no), adjacent segment level (to instrumentation) (yes/no) age, BMI, cord area, duration between fusion surgery and imaging exam, and MJOA score. Statistical tests were performed using linear mixed effects (LME) modeling with subject index modeled as a random effect. Twelve separate models of cord ADC were computed to probe key questions related to the study hypotheses. Modeling was performed in R using the lme4 library and model analysis utilized the afex library to provide hypothesis test results using likelihood ratio tests.
Results
Exemplary sample images of an instrumented fusion CSM subject are provided in Figure 1.Figure 2 provides the linear mixed effects results of Model 1, which regressed cord ADC against the demographic and morphological data elements available within the control cohort. These results showed strong inverse relationships between ADC and BMI and vertebral level, which were carried through as predictors in all ensuing models.
Figure 3 provides the results of the remaining 11 LME models. Following the results of Model 1, vertebral level and BMI strongly correlated with ADC in all models. In addition, the CSM data showed a reduction in ADC relative to controls for the entire cervical cord (Model 2, p=0.005) and instrumented levels (Model 3, p=0.004). The non-instrumented levels (neglecting adjacent segments) did not show a statistically significant difference (Model 4, p =0.107) from controls, while the adjacent segments showed a trending reduction which was slightly above the significance threshold (Model 5, p= 0.069). Within the CSM cohort, only the adjacent segment vs non-instrumented showed a mild significant trend, with adjacent segments having reduced ADC (Model 8, p=0.046). Finally, the only correlation with clinical metrics was between post-operative duration and adjacent segment ADC, with the adjacent segments having reduced ADC at further post-operative MRI examination visits (Model 12, p=0.031).
Discussion
Though previous studies have shown reductions of diffusivity in CSM patients treated with decompression surgical procedures [6,7,8] the use of single-shot echo planar imaging methods hindered their ability to perform DW measurements at levels that were decompressed using metallic instrumentation.Utilizing recently developed multi-spectral diffusion-weighted MRI techniques, the present study has revealed substantial reductions in diffusivity within the post-surgical CSM spinal cord at levels at and adjacent to fusion instrumentation. This confirms the hypothesis that diffusivity of the spinal cord is reduced in post-surgical CSM patients at and near levels of metallic instrumented spinal fusion.
The present study was not targeted towards subjects with failed surgical interventions (evidenced by the high MJOA scores). Future studies within cohorts with unresolved CSM symptoms may help establish the value of DW-MSI for regional assessment of failed decompression after fusion management of CSM.
Acknowledgements
This work was supported by the Department of Defense Congressionally Directed MedicalResearch Program, Spinal Cord Injury Research Program, award number W81XWH1910273.Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense.References
- Tracy, J. A. and Bartleson, J. (2010). Cervical spondylotic myelopathy. The Neurologist 16, 176–187
- Tetreault Lindsay, Kopjar Branko, Nouri Aria, et al. The modified Japanese OrthopaedicAssociation scale: establishing criteria for mild, moderate and severe impairment inpatients with degenerative cervical myelopathy European Spine Journal. 2017;26:78–84.
- Koch, K. M., Brau, A. C., Chen, W., Gold, G. E., Hargreaves, B. A., Koff, M., et al. (2011). Imaging near metal with a MAVRIC-SEMAC hybrid. Magnetic Resonance in Medicine 65, 71–82. doi:10.1002/mrm. 22523
- Koch, K. M., Bhave, S., Gaddipati, A., Hargreaves, B. A., Gui, D., Peters, R., et al. (2018). Multispectral diffusion-weighted imaging near metal implants. Magnetic Resonance in Medicine 79, 987–993
- Leener, B. D., LA ̃ ©vy, S., Dupont, S. M., Fonov, V. S., Stikov, N., Collins, D. L., et al. (2017). Sct: Spinal cord toolbox, an open-source software for processing spinal cord {MRI} data. NeuroImage 145, Part A, 24 – 43. doi:https://doi.org/10.1016/j.neuroimage.2016.10.009
- Sato, T., Horikoshi, T., Watanabe, A., Uchida, M., Ishigame, K., Araki, T., et al. (2012). Evaluation of cervical myelopathy using apparent diffusion coefficient measured by diffusion-weighted imaging. American Journal of Neuroradiology 33, 388–392
- Ma, X., Han, X., Jiang, W., Wang, J., Zhang, Z., Li, G., et al. (2018). A follow-up study of postoperative dcm patients using diffusion mri with dti and noddi. Spine 43, E898–E904
- Rajasekaran, S., Kanna, R. M., Chittode, V. S., Maheswaran, A., Aiyer, S. N., and Shetty, A. P. (2017). Efficacy of diffusion tensor imaging indices in assessing postoperative neural recovery in cervical spondylotic myelopathy. Spine 42, 8–13
Figures
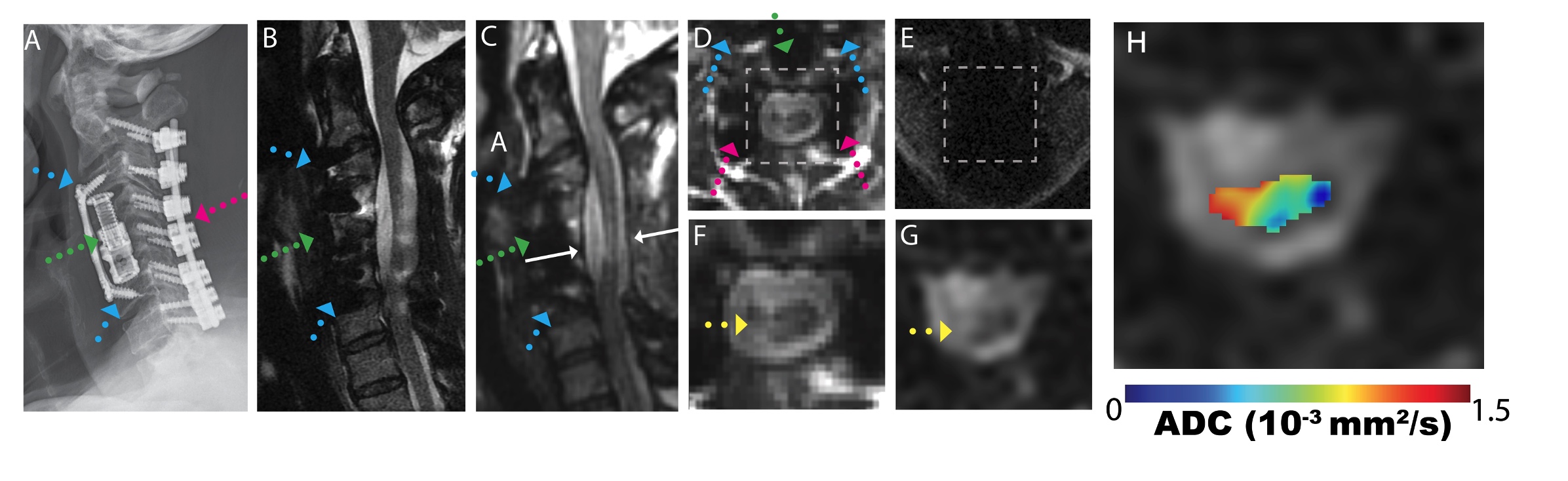
Figure 1: A) Radiograph illustrating fusion hardware (blue, green, and pink arrows) with CSM subject. B) Conventional MARS FSE/TSE T2 weighted image, demonstrating substantial image distortions near the metal hardware. C) Isotropic (1.2 mm) 3D-MSI T2 weighted image with minimal image artifacts. D) Axial reformat of isotropic 3D-MSI, indicated by white arrows in (C). E) Conventional single-shot b=0 EPI image=, F) zoomed 3D-MSI T2w image in across box indicated in (D). ,G) DW-MSI b=0, and H) DW-MSI ADC . Yellow arrows indicate region of hyperintense T2w signal within the cord.
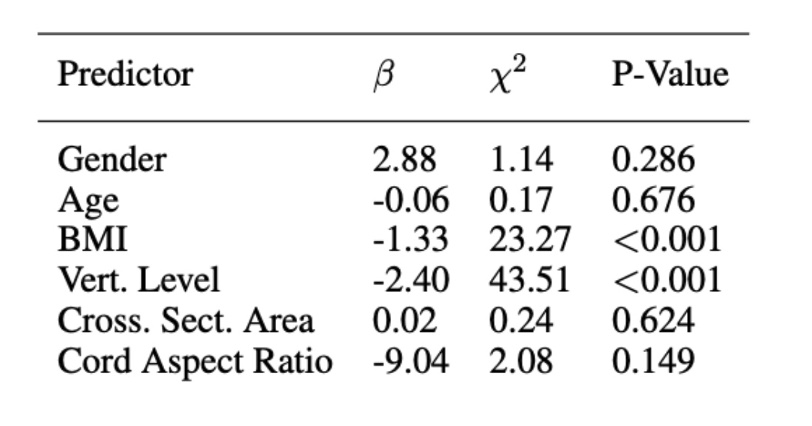
Figure 2. LME results of Model 1, regressing demographic and morphological data elements against cord ADC in un-instrumented asymptomatic participants. LME results are reported as beta coefficients, with chi-squared results and p-values derived from maximum likelihood tests of the computed models.
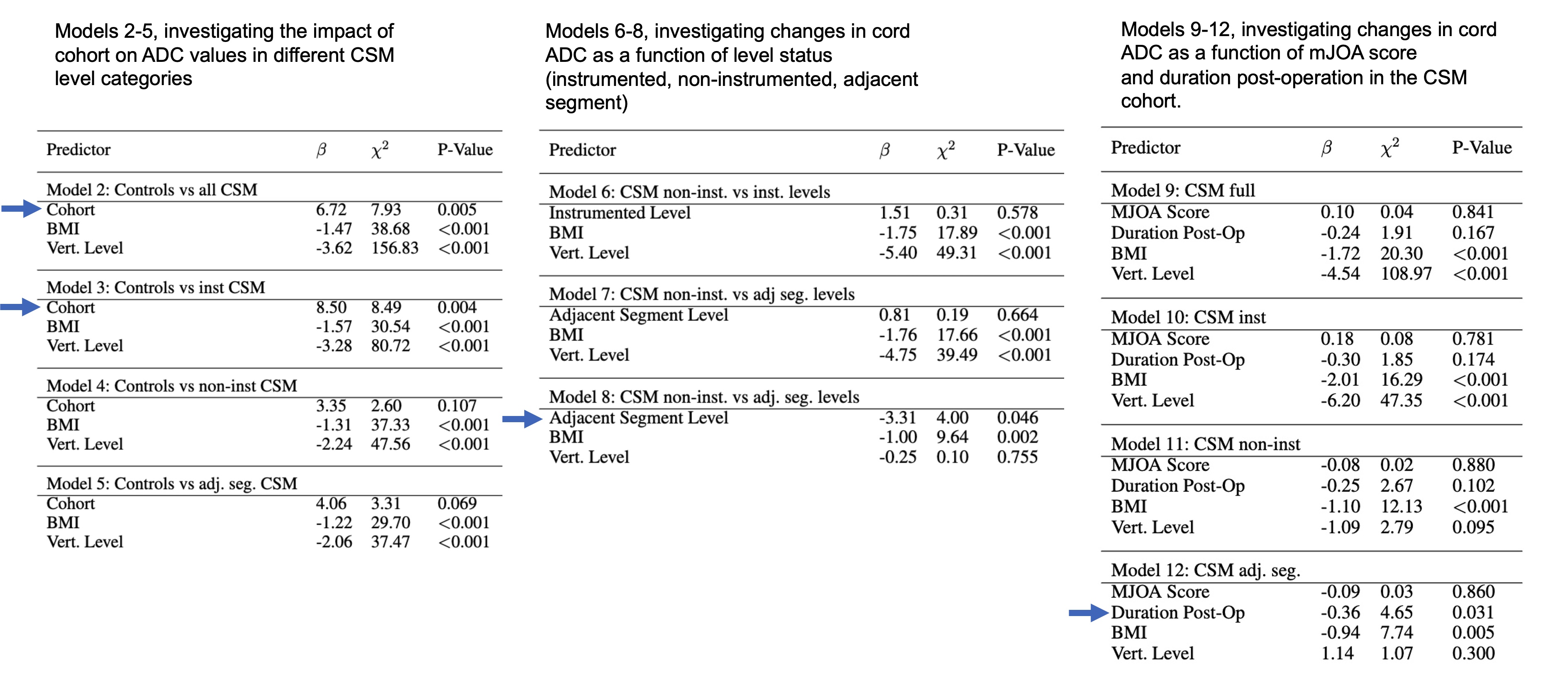
Figure 3. Results of LME modeling across and within cohorts. LME results are reported as beta coefficients, with chi-squared results and p-values derived from maximum likelihood tests of the computed models. Key findings related to study hypotheses are indicated with blue arrows.
DOI: https://doi.org/10.58530/2023/1562