1551
CT-Guided Cervical Spinal Cord and Nerve Root Adhesiolysis for Intractable Hiccup:Based on the evidence of 3.0 T magnetic resonance neuroimaging1Affiliated Hospital of North Sichuan Medical College, Nanchong 637000, Nanchong, China, 2The Fifth People's Hospital of Chengdu, Chengdu, China, 3Second Affiliated Hospital of North Sichuan Medical College,Nanchong 637100, Nanchong, China, 4MR Scientific Marketing, Siemens Healthcare, Shanghai, China, Shanghai, China
Synopsis
Keywords: Head & Neck/ENT, Head & Neck/ENT
The preoperative neuroimaging examination can clearly reflect the abnormalities of cervical intervertebral disc, cervical plexus and brachial plexus, help us understand the potential pathogenesis of intractable hiccup, and improve the efficacy.Introduction
Hiccups are caused by sudden involuntary contractions of the diaphragm and intercostals, followed by temporary closure of the glottis. It can occur in all stages of growth and development, including the fetus, infants, children and adults [1-4]. In most cases, the duration is usually very short, usually no more than 48 hours. In a few cases, hiccups lasting for several days, months or even years, and lasting more than 30 days are called stubborn hiccups [1,2,5]. Obstinate snoring will affect the patient's diet, sleep, therefore, it is very important to quickly and effectively prevent or stop stubborn hiccup. In this study, we aim to evaluate the efficacy and safety of CT guided epidural lysis of spinal nerve root adhesion in the treatment of intractable hiccup, and to evaluate the neuromorphological changes before and after surgery through 3.0T magnetic resonance neuroimaging(MRN), providing reference for clinical application.Materials and Methods
A retrospective cross-sectional evaluation was conducted for this study, which was approved by our hospital, and all patients signed the informed consent form. A total of 41 patients were included in the study. All patients received brachial plexus imaging and CT guided cervical nerve root release before surgery. The MR study were performed on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany; 32 channel head neck joint coil), the scanning parameters of preoperative MR cervical nerve imaging were as follows:3D-SPACE-STIR-COR+C: TR=3500ms, TE=190ms, Slice thicken=1mm, Fov=28x28cm, Acquisition matrix=326x192.Flip angle=18°. The image results were collected and analyzed by wo senior radiologists, and the operation was performed by the same senior doctor. The main data collected included: demographic data (age, sex), chief complaints, Initial symptoms, operation date and MRN imaging results,Intractable hiccup and quality of life score before and after operation,the related complications were also recorded.RESULTS
A total of 34 patients were included in the study. 14 males and 20 females; The average age was (45.2 ± 5.4) years, ranging from 36 to 74 years old; The course of disease was 3 months to 12 years, with an average of (3.4 ± 0.4) years. All patients presented with long-term hiccup (more than 3 months), of which 27 patients had discomfort in neck and shoulder, scapula or upper limbs.In 34 patients, MRN was positive in all patients, including cervical disc herniation or abnormal nerve signal. The positive rate of cervical disc herniation was 100% (34/34), and the positive rate of abnormal MRN signals was 47.05% (16/34). The incidence of hiccup at 1 week, 1 month, 3 months and 6 months after operation was significantly lower than that before operation.The effective rates were 82.35% (28/34), 88.24% (30/34), 97.06% (33/34) and 97.06% (33/34), respectively. At 3 and 6 months after operation, the components of SF-36 increased (P < 0.05). The main complication was transient subcutaneous swelling of neck, which was relieved within 3 days. Intraoperative hypertension occurred in 3 cases, and transient heart rate decreased significantly in 2 cases. All patients had no severe complications such as massive hemorrhage or death. The changes of cervical plexus and brachial plexus before and after operation were compared by MRN analysis. After 3 months, 85.29% (29/34) patients had changes in MRI, suggesting that the possible mechanism of intractable hiccup was related to the changes of cervical nerve.Discussion
Obstinate hiccup is not a fatal disease, but it often brings patients great trouble and leads to a significant decline in the quality of life. The treatment effect is different, which may be due to insufficient preoperative evaluation, especially the lack of imaging data. In this study, we determined the abnormalities of the cervical plexus and brachial plexus through 3.0T magnetic resonance neuroimaging, and then achieved good results through the neurolysis of the cervical plexus and brachial plexus. Through careful analysis of the patient's imaging and clinical data, we believe that the pathological mechanism of obstinate hiccups may be cervical spondylosis. Prolonged cervical disc herniation can lead to spinal neuropathy, especially at the C3-5 segment, because they only constitute the phrenic nerve.Conclusion
It is necessary to carry out MRI evaluation for patients with intractable hiccup, which is helpful to have a deeper understanding of the pathogenesis of intractable hiccup and to determine the treatment target. In the future, more image sequence research may find some patients with negative results earlier.Acknowledgements
The authors would like to thank Dr. Anup Bhetuwal for revising the article.References
1. Leung, AKC; Leung, AAM; Wong, AHC; et al. Hiccups: A Non-Systematic Review. CURR PEDIATR REV. 2020-01-01;16(4):277-284.
2. Rouse, S; Wodziak, M; Intractable Hiccups.CURR NEUROL NEUROSCI. 2018-06-22;18(8):51.
3. Chang F, Lu C. Hiccup: mystery, nature and treatment. J Neurogastroenterol Motil. 2012;18:123–30.
4. Wilcox SK, Garry A, Johnson MJ. Novel use of amantadine: to treat hiccups. J Pain Symptom Manag. 2009;38(3):460–5.
5. Friedman NL. Hiccups: a treatment review. Pharmacotherapy 1996;16(6):986-995.
Figures
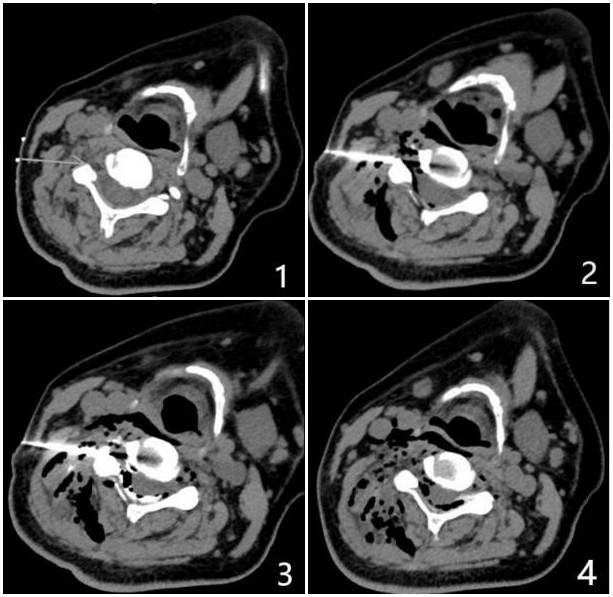

Figure 2. Male, 38 years old, with intractable hiccup for 3 months, 3.0 T MR brachial plexus imaging showed that the signal of the left fourth cervical nerve was obviously increased.
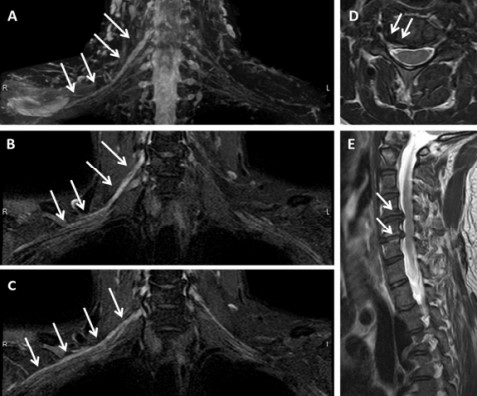
Figure 3. MRN examination of brachial plexus in cervical spondylotic radiculopathy. (A, B, C) coronal T2-TDEAL images; (D) Axial T2WI showed that the right intervertebral foramen of C4/5 intervertebral disc protruded; (E) T2WI sagittal position; The signal of right C5 and C6 nerve roots and corresponding segments of brachial plexus was significantly higher than that of left side (long arrow A, B, C). At right C4/5 and C5/6, herniation of intervertebral disc and stenosis of corresponding intervertebral foramen can be seen (short arrows D, E).
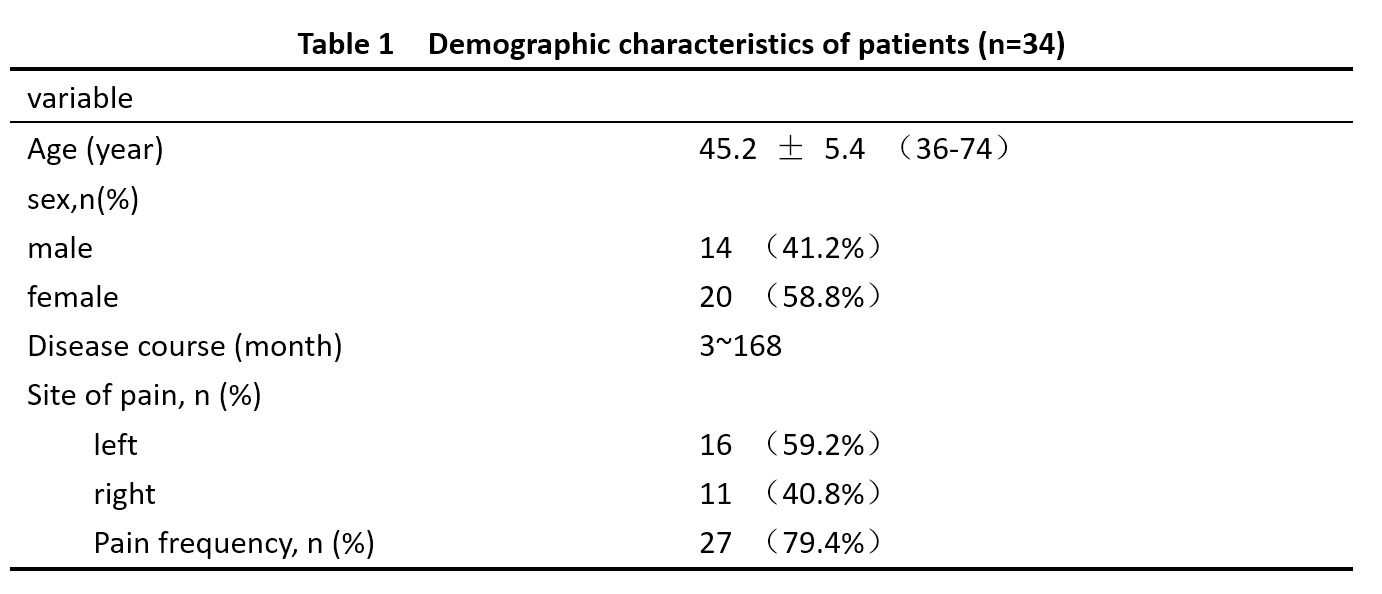
Table 1 Demographic characteristics of patients (n=34)