1549
Feasibility of MUSE DTI in differentiation of spinal cord injury severity in cervical spondylotic myelopathy
Haoyue Shao1, Xiangyu Tang1, Qiufeng liu1, and Weiyin Vivian Liu2
1Tongji Hospital Affiliated to Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China, 2GE Healthcare, Beijing, China
1Tongji Hospital Affiliated to Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Spinal Cord, Diffusion/other diffusion imaging techniques, cervical spondylotic myelopathy
MUSE (Multiplexed Sensitivity-Encoding) is a novel diffusion weighted imaging with 2 to 3-excitations, phase acquisition step reduction, to achieve high-resolution diffusion imaging, higher signal-to-noise ratio, fewer motion artifacts and magnetic field inhomogeneities. In this study, we applied MUSE-based diffusion tensor imaging to investigate the compression-caused microstructure changes in the spinal cord of each subject. Our results suggested that MUSE-DTI computed parameters (Trace, FA, ADC) have dependable diagnostic values in detecting CSM (cervical spondylotic myelopathy) and that the ADC value is the best indicator of spinal cord compression.Introduction and Purpose
The most frequent type of spinal cord injury is cervical spondylotic myelopathy (CSM). Conventional magnetic resonance imaging (MRI) is the gold diagnosis standard for CSM, but conventional MRI is limited in reflecting the severity of myelopathy and predicting surgical outcomes in patients with CSM. Diffusion tensor imaging (DTI) could reflect microstructural changes in the spinal cord by tracing water molecular diffusion. However, it is challenging to evaluate spinal cord damage in cervical spinal canal stenosis by DTI due to local field inhomogeneity and heterogeneous susceptibility [1]. This study aimed to investigate the clinical diagnosis value of a novel Multiplexed Sensitivity-Encoding Diffusion Tensor Imaging (MUSE-DTI) in patients with CSM.Materials and Methods
Patients: From August 2021 to March 2022, a total of 60 subjects (22-71 years) were enrolled including 26 CSM patients and 34 healthy subjects (25 males and 35 females). The clinical severity of myelopathy of each subject was assessed by the clinical Japanese Orthopaedic Association scale (JOA), Visual Analogue Scale (VAS), and Neck Disability Index (NDI). Imaging: A 3.0T MR scanner (GE, SIGNATM Architect) was used to perform the MUSE-DTI sequence (The imaging parameters were as follows: number of shots=2; field of view=20×0.8mm; slice thickness=4.0mm; spacing=0mm; number of diffusion direction=12; b-value=600sec/mm2; NEX=3) on each subject. The cervical canal stenosis of subjects was classified from grade0 to grade 3 according to the method of Kang, Y [2]. Data processing: Trace, FA, and ADC value maps were generated by post-processing MUSE-DTI data on the GE workstation. Mann-Whitney U test was used to compare the differences of each parameter value between different grades, and Spearman correlation analysis was used to test the correlation between the DTI parameter values of maximum compression level (MCL) and clinical JOA score, VSA score, NDI score. The efficient of DTI-derived parameters in the diagnosis of spinal cord compression (grades 0 and grade 1 vs grades 2 and grade 3) was tested by the receiver operating characteristic (ROC) curve.Results
Trace values and FA values at MCL showed a decreasing trend from grade 0 to grade 3 while the ADC values at MCL showed an increasing trend with increasing grades. Except for the Trace values between grade 2 and grade 3, the FA values between grade1 and grade 2, and the ADC values between grade 0 and grade 1, significant differences in Trace, ADC, and FA values were found between adjacent groups among grades 0-3 (p<0.05). The clinical JOA score has a significant correlation with the Trace (P=0.000), FA (P=0.001), and ADC (P=0.000) values. The ROC curve model showed a cutoff of ADC at MCL (value of 1153.5mm2/s).Discussion and Conclusion
MUSE DTI can provide more details in reflection of the potential changes of the spinal cord in CSM than conventional gradient echo planar imaging (GRE-EPI). This study found that the ADC value is a good indicator of spinal cord compression. In addition, the spinal cord changes (Trace, FA, and ADC values) at the maximum intervertebral disc herniation in CSM patients were significantly correlated with cervical spondylosis-related symptoms. Therefore, MUSE DTI could be a good bioimaging technique for clinical auxiliary diagnosis of cervical spondylotic myelopathy.Acknowledgements
Thanks to teacher Liu Qiufeng for collecting the patient's image data, and teacher Liu Weiyin for adjusting the parameters of the image sequence.References
1. Shafieizargar B, Jeurissen B, Poot DHJ, den Dekker AJ, Sijbers J. Multi-contrast multi-shot EPI for accelerated diffusion MRI. In: 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC). ; 2021:3869-3872. doi:10.1109/EMBC46164.2021.96300692. Kang Y, Lee JW, Koh YH, et al. New MRI Grading System for the Cervical Canal Stenosis. American Journal of Roentgenology. 2011;197(1): W134-W140. doi:10.2214/AJR.10.5560
Figures
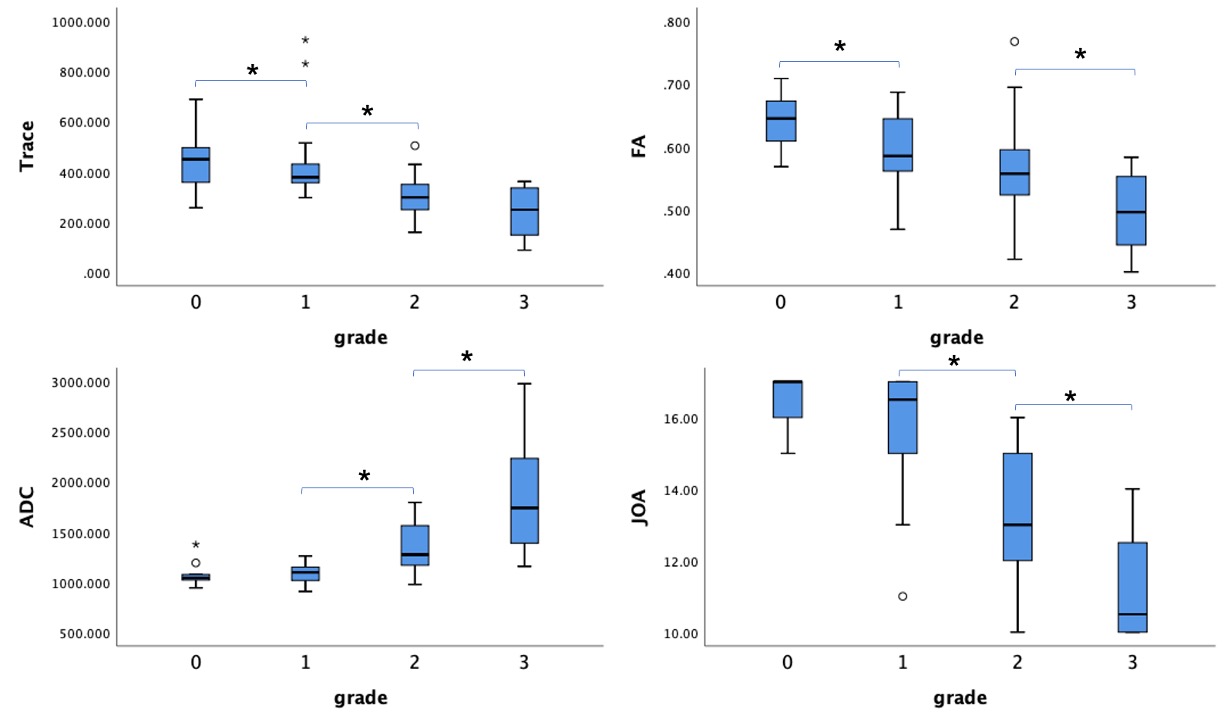
Figure 1 Trace, FA, ADC, and JOA values of compressive spinal cord with different grades (0-3). Noteworthily, the C2/3-C6/7 intervertebral disc levels were reckoned as grade 0 of spinal cord for Trace, FA, and ADC measurements.
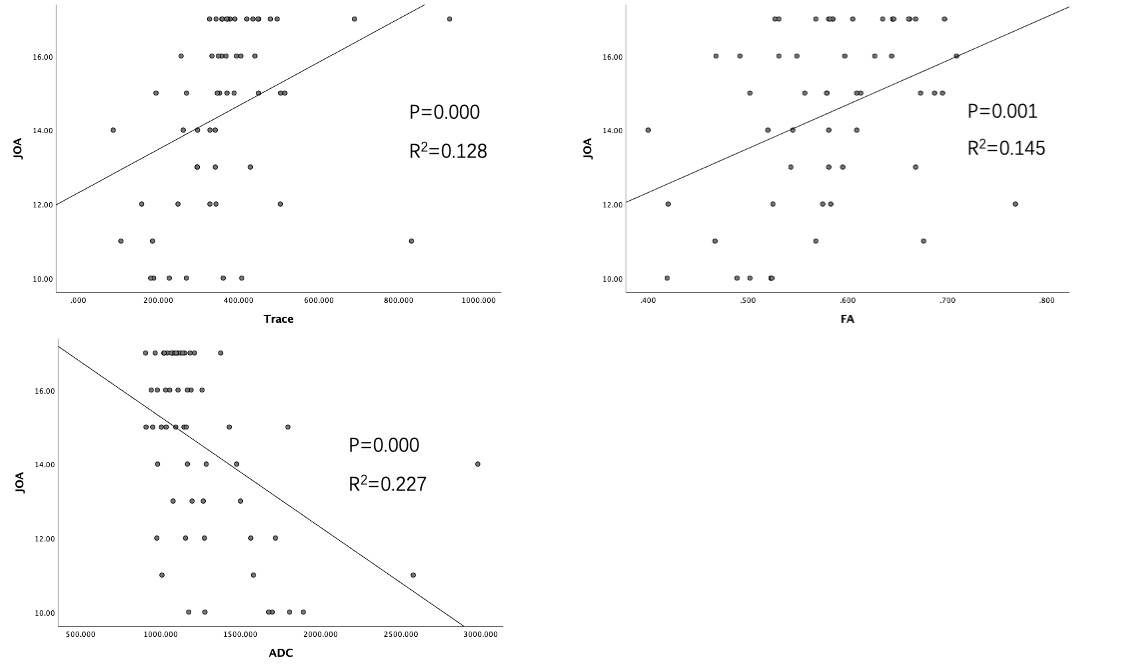
Figure 2 The correlations between DTI-derived parameters (Trace, FA and ADC values) and the JOA scores and compressive spinal cord with different grades (0-3). Noteworthily, the C2/3-C6/7 intervertebral disc levels were reckoned as grade 0 of spinal cord for Trace, FA, and ADC measurements.
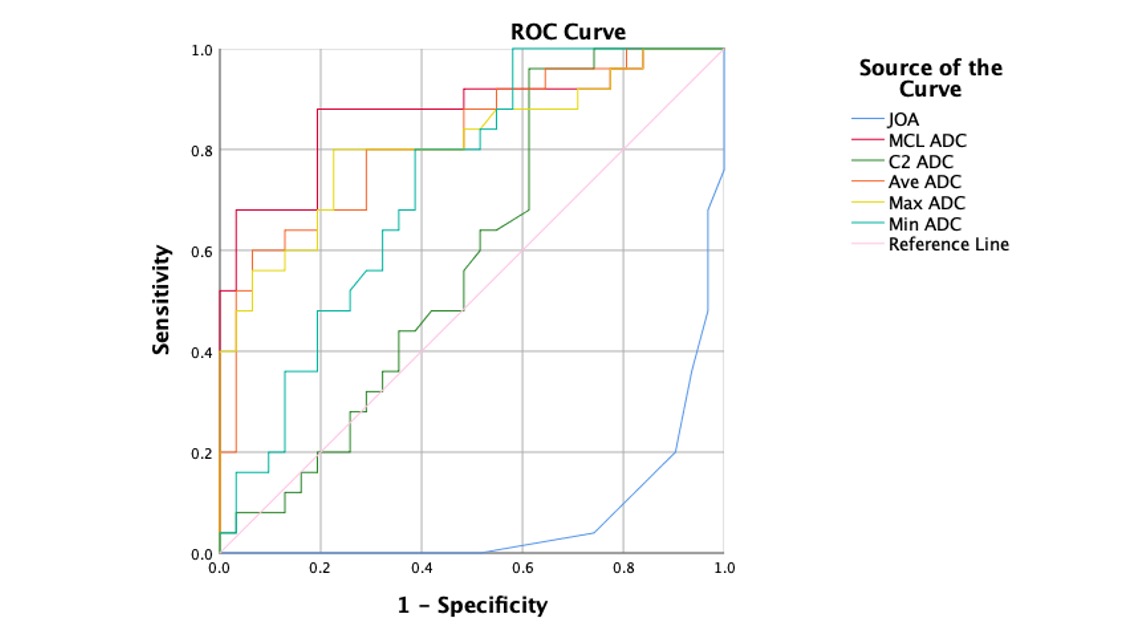
Figure 3 ROC curves showed the diagnosis performance of ADC values and JOA score in distinguishing different grades of CSM.
DOI: https://doi.org/10.58530/2023/1549