1513
Imaging Ascending Aortic Wall Stretch Using Breath-Held Displacement Encoding with Stimulated Echoes MRI: An Intra-scan Reproducibility Study1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2University of Virginia, Charlottesville, VA, United States, 3Surgery, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Vessel Wall, Preclinical, Aortic Strain; DENSE MRI
In vivo assessment of the mechanical properties of the aorta stands to offer valuable information to evaluate and predict the progression of cardiovascular diseases. Displacement encoding with stimulated echoes (DENSE) is a non-invasive phase-contrast MRI technique that has been adapted to measure ascending aortic wall stretch. Previous studies utilizing long respiratory-gated acquisitions are prone to artifacts from residual cardiac or respiratory motion. In this study, we investigated the reproducibility of a novel breath-held aortic DENSE imaging protocol. The proposed breath-held protocol was highly reproducible (COV=3.27% and LCCC=0.97). Finally, the measured aortic stretch followed the expected relationship with age.Introduction
In vivo assessment of the mechanical properties of the aorta stands to offer valuable information to evaluate the progression of cardiovascular diseases and predicting major cardiovascular events and clinical outcomes, independent of traditional risk factors. For example, an increase in aortic stiffness provides direct assessment of the overall cardiovascular risk in asymptomatic hypertensive subjects1, while the stiffness variation in abdominal aortic aneurysms (AAAs) is associated with clinical outcomes including rupture and the need for repair2. Although pulse wave velocity measured by MRI or ultrasound can provide global assessment of aortic stiffness, to date no technique exists that can provide reproducible measurements of local aortic wall mechanical properties.Displacement encoding with stimulated echoes (DENSE) is a non-invasive phase-contrast MRI technique that has been thoroughly validated for measuring myocardial tissue displacement under cardiac loading, from which local stretch or strain can be derived to gauge stiffness3,4. Previous studies have demonstrated the feasibility of adapting DENSE imaging to measure in vivo aortic wall stretch and strain5–7. These have utilized long (>9-10-min) respiratory-gated acquisitions. Given that the aortic wall is thin (1-2.5 mm depending on pathology), even a small amount of residual cardiac or respiratory motion can result in uninterpretable studies, which in our experience can affect up to one half of studies.
The aim of this study was to investigate the reproducibility of a novel breath-held aortic DENSE imaging protocol utilizing outer volume suppression in healthy subjects. Moreover, measurements from the proposed breath-held protocol were compared to a free-breathing DENSE protocol reported in previous studies5 whenever that protocol produced interpretable results. Finally, as a preliminary validation step, we sought to determine if the DENSE-derived aortic wall stretch exhibited the known relationship of aortic stiffness and age.
Methods
In this prospective study, in vivo aortic DENSE was performed on 5 healthy subjects (3 male; age, 39 ± 16 years, range: 22-65 years).Data were acquired at 3T (Skyra, Siemens Healthcare, Erlangen, Germany) for a single imaging plane prescribed orthogonal to the vessel centerline approximately 2 cm above the sinotubular junction. This location matches the typical location of maximum diameter of the ascending aorta in patients with ascending thoracic aortic aneurysms that have been previously studied with free-breathing DENSE5.
For breath-held aortic DENSE, a cardiac-gated DENSE acquisition with outer volume suppression was performed at end-expiration. Imaging parameters were TE=1 ms, TR=12 ms, 8 spiral interleaves/image, 2 spiral interleaves/heartbeat, FOV=180-200 mm2, slice thickness=12 mm and in-plane matrix size=135×135 to 154×154, displacement encoding frequencies of 0.04-0.09 cycles/mm, balanced two-point encoding and two-point complementary spatial modulation of magnetization (CSPAMM) to suppress spurious free induction decays and artifact-generating echoes8,9. The breath-hold time was 18 heartbeats for each displacement encoding direction. Each encoding direction was acquired in single breath-hold, for a total of 3 breatholds per fully-encoded DENSE dataset.
Intra-scan reproducibility of the breath-held DENSE protocol was evaluated by acquiring two sets of scans separated by 10 min. In between the two scans, either a 10-min free-breathing DENSE scan as previously described5 or a 10-min of other imaging (not used in this study) was acquired.
For both breath-held and free-breathing DENSE, encoding was performed at the time of maximal aortic distension at end-systole as determined by standard CINE MRI performed at the target level of the aorta (i.e., time of maximal ascending aorta distension). Displacement readout was performed 350-400 ms later, in diastole, in order to quantify the wall stretch between systole and diastole. A purpose-built post-processing software was used to derive the aortic wall stretch based on the acquired displacements.
Results
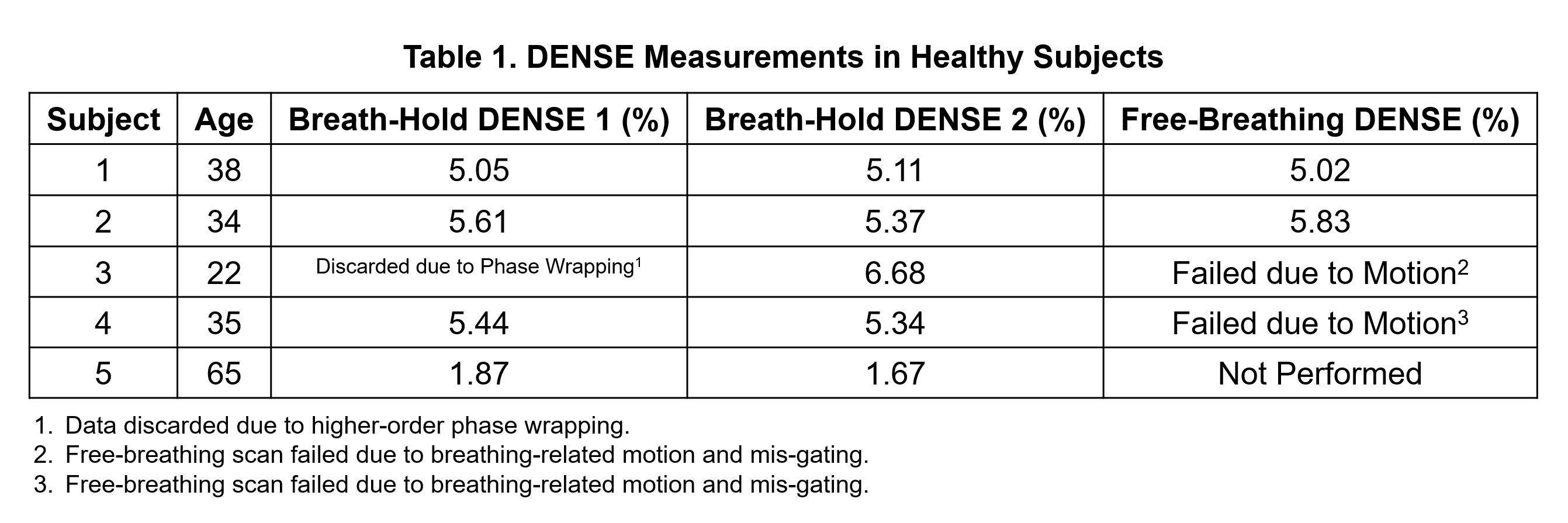
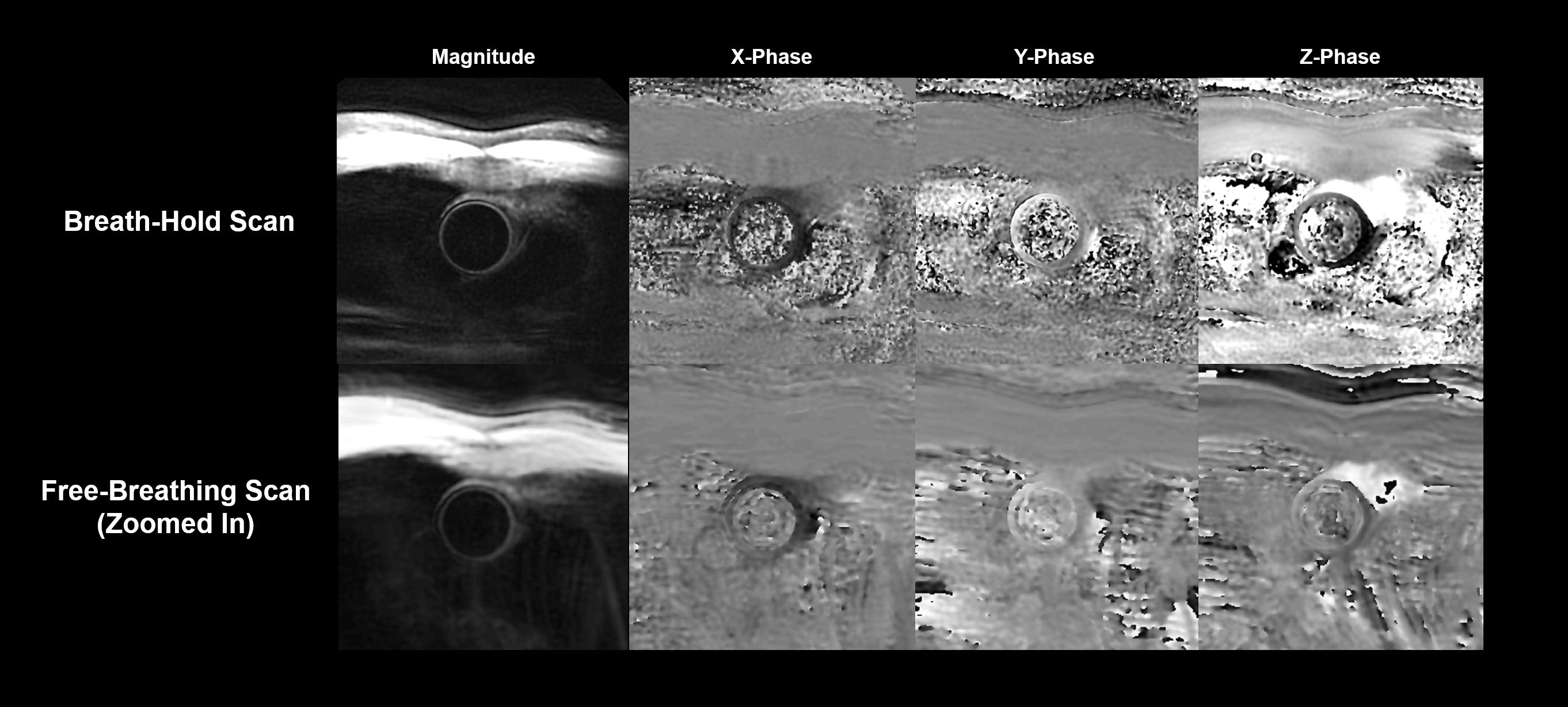
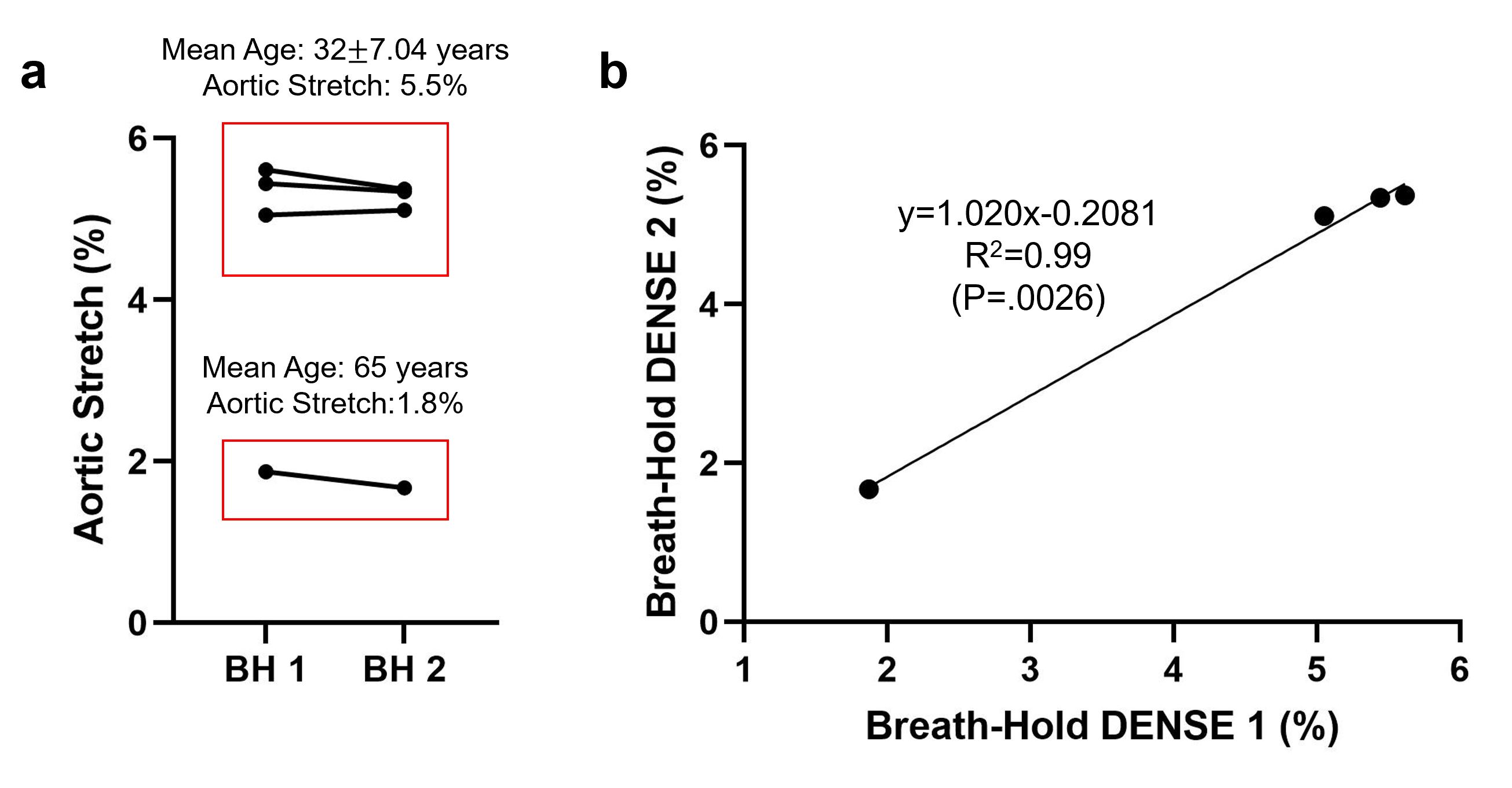
Table 1 provides DENSE measurements for each subject. One breath-held measurement was discarded due to phase wrapping. Free-breathing DENSE was successfully performed in two subjects. Figure 1 demonstrates the breath-held and free-breathing aortic DENSE measurements in one subject.Across all subjects, the aortic stretch was 4.49±1.76% in the first breath-held acquisition, and 4.38±1.80% in the second, with a difference of 0.12±0.13%. Figure 2a shows the DENSE-derived aortic stretch variation between the two repeated breath-held measurements. A significant linear correlation was observed between the two breath-held DENSE acquisitions (Figure 2b, slope=1.02; Pearson r=0.9974; P=.0026). The coefficient of variation (CoV) was 3.27%, and the Lin’s concordance correlation coefficient (LCCC) was 0.97, suggesting high reproducibility of the proposed breath-held aortic DENSE technique. For the 2 subjects with a successful free-breathing DENSE, the difference between the breath-held mean measurement and free-breathing measurement of stretch was 0.20±0.19%.
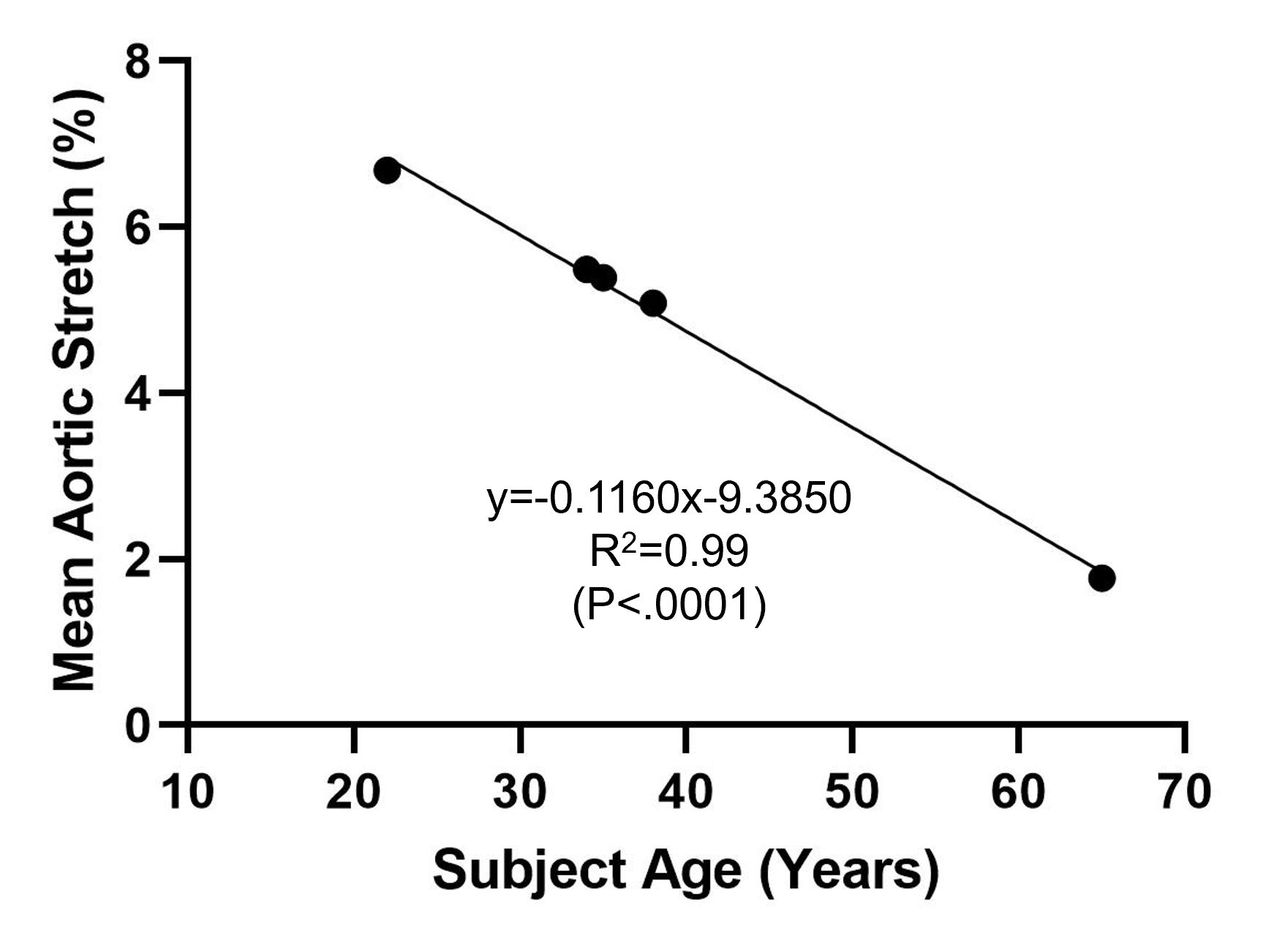
With regards to the association of the observed stretch and age, higher mean aortic stretch was observed in young subjects (mean age=32±7 years) when compared to a subject at 65 years, suggesting higher aortic compliance among the young subjects. Finally, the DENSE-derived aortic stretch significantly correlated to subjects’ age with a Pearson correlation coefficient r=0.9983 as shown in Figure 3 (P<.0001).
Conclusion
The proposed breath-hold aortic DENSE protocol is highly reproducible with a coefficient of variation of 3.27%. In the limited number of cases where a free-breathing DENSE acquisition was successfully acquired, aortic stretch differed compared to the free-breathing aortic DENSE protocol by 0.2%. Finally, the measured aortic stretch followed the expected relationship with age10.Acknowledgements
No acknowledgement found.References
1. Laurent S, Alivon M, Beaussier H, Boutouyrie P. Aortic stiffness as a tissue biomarker for predicting future cardiovascular events in asymptomatic hypertensive subjects. Ann Med. 2012;44(sup1):S93-S97. doi:10.3109/07853890.2011.653398
2. Dong H, Raterman B, White RD, et al. MR Elastography of Abdominal Aortic Aneurysms: Relationship to Aneurysm Events. Radiology. 2022;304(3):721-729. doi:10.1148/RADIOL.21232
3. Aletras AH, Ding S, Balaban RS, Wen H. DENSE: Displacement Encoding with Stimulated Echoes in Cardiac Functional MRI. J Magn Reson. 1999;137(1):247-252. doi:10.1006/JMRE.1998.1676
4. Zhong X, Spottiswoode BS, Meyer CH, Kramer CM, Epstein FH. Imaging three-dimensional myocardial mechanics using navigator-gated volumetric spiral cine DENSE MRI. Magn Reson Med. 2010;64(4):1089-1097. doi:10.1002/MRM.22503
5. Haraldsson H, Hope M, Acevedo-Bolton G, et al. Feasibility of asymmetric stretch assessment in the ascending aortic wall with DENSE cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2014;16(1):6. doi:10.1186/1532-429X-16-6
6. Iffrig E, Wilson JS, Zhong X, Oshinski JN. Demonstration of circumferential heterogeneity in displacement and strain in the abdominal aortic wall by spiral cine DENSE MRI. J Magn Reson Imaging. 2019;49(3):731-743. doi:10.1002/JMRI.26304
7. Wilson JS, Taylor WR, Oshinski J. Assessment of the regional distribution of normalized circumferential strain in the thoracic and abdominal aorta using DENSE cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2019;21(1):59. doi:10.1186/s12968-019-0565-0
8. Kim D, Gilson WD, Kramer CM, Epstein FH. Myocardial Tissue Tracking with Two-dimensional Cine Displacement-encoded MR Imaging: Development and Initial Evaluation. Radiology. 2004;230(3):862-871. doi:10.1148/radiol.2303021213
9. Zhong X, Spottiswoode BS, Cowart EA, Gilson WD, Epstein FH. Selective suppression of artifact-generating echoes in cine DENSE using through-plane dephasing. Magn Reson Med. 2006;56(5):1126-1131. doi:10.1002/MRM.21058
10. Hickson SS, Butlin M, Graves M, et al. The Relationship of Age With Regional Aortic Stiffness and Diameter. JACC Cardiovasc Imaging. 2010;3(12):1247-1255. doi:10.1016/j.jcmg.2010.09.016
Figures