1506
Demonstration of Intracranial Aneurysm Healing after Endovascular Coiling Evaluated by 3D T1 SPACE Magnetic Resonance
Sho-Jen Cheng1, Xue-Zhe Lu2, and Yi-Hsin Wang1
1Department of Medical Imaging, Taipei Medical University Hospital, Taipei, Taiwan, 2Siemens Healthcare Limited, Taipei, Taiwan
1Department of Medical Imaging, Taipei Medical University Hospital, Taipei, Taiwan, 2Siemens Healthcare Limited, Taipei, Taiwan
Synopsis
Keywords: Vessel Wall, Vessels
Angiography is a gold standard tool in the follow-up of the treated aneurysms to identify if there is aneurysm recanalization need further management. Despite non-invasive MR-based assessments be reported, the pathological changes of aneurysm on MRI was not clear. In this study, we employed three-dimensional variate flip angle MRI to evaluate the endothelial healing in ten cases with intracranial aneurysms after endovascular management. HRVWI routinely demonstrate the enhancement pattern of the aneurysmal neck not only the aneurysmal wall in both cross-sectional and time-serial follow up, increasing our confidence in making the decision whether to retreat or not.Introduction
Coil embolization is one of the main treatment of intracranial aneurysms in recent decades1. While coil embolization has been shown to be safe and effective in the occlusion of the aneurysmal sac, recanalization of the treated aneurysm, resulting in retreatment, occurs in approximately 10%–20% of cases2,3. Understanding of healing following coil embolization is essential to improving patient outcomes. Angiography is a gold standard tool in the follow-up of the treated aneurysms to identify if there is aneurysm recanalization need further management. and the barrier between aneurysm and artery formatted after coil embolization4. Optical coherence tomography was also used in human subject to evaluate the healing of vascular5.Although above invasive imaging techniques could provide reliable information about vessel healing after coil embolization, noninvasive assessment was still explored in order to decrease risk of patient and workload of postprocedural following up6. Wall enhancement in vessel wall magnetic resonance imaging (MRI) could possibly serve as an imaging marker for completed aneurysm healing and a lower risk for reperfusion. Therefore, incorporating MRI in the follow-up after embolization detect delayed aneurysm healing and determine completed aneurysm healing after coiling. The wall enhancement of aneurysms was reported for risk stratification in previous study7.
However, most publication focused only on the enhancement of aneurysmal wall and cavities. In this study, we employed three-dimensional variate flip angle MRI to evaluate the endothelial healing in the neck of intracranial aneurysms after endovascular management and investigate the ability to be a routine assessment.
Method
The study population involved ten patients after aneurysmal coiling in different intracranial vascular territories. The patients have cerebral aneurysms after endovascular management in the 6-12 month-period for one year.The images were acquired on a MAGNETOM 3T scanner (Siemens Healthcare, Erlangen, Germany) with a 64-channel head & neck coil. High-resolution vessel wall imaging (HRVWI) was done by 3D T1-weighted SPACE in a 4 cm transverse slab with following parameters: TR/TE= 800/21 ms, bandwidth = 460 Hz/pixel, slice thickness = 0.6 mm, FOV = 180X162 mm, voxel size=0.6X0.6 mm with interpolation. The HRVWI and routine time-of-flight MRA were obtained before and after injection of gadolinium chelate (10 mL gadoteric acid; Dotarem, Guerbet, Marans, France), acquisition time of single sequences was 5 minutes and 33 seconds.
The overall image quality of vessel wall MR images was visually evaluated by experienced neuroradiologist to identify the enhancing barrier at the aneurysmal neck with grade 0 to 3 demonstrated in figure 1. The healing process of the aneurysms would be evaluated and compared to the gold standard cerebral angiographic findings and routine time-of-flight MRA.
Result
Ten patients aneurysmal coiling follow up in three month after intervention or later. The enhancements of aneurusm was summarized in table 1. Nine treated aneurysms shoewed moderate to good aneurysmal wall enhancement in HRVWI, four treated aneurysm presented good aneurysmal neck enhancement, two presented thin moderate enhancement, three presented thin mild enhancement, and one persistent defect at the aneurysmal neck. Small residual neck was found in three patients in angiographic follow up.The 6 month following up of case 8 revealed clear enhancement of aneurysm on HRVWI after contrast median injection while time-of-flight MRA showed susceptibility effect in aneurysm. The angiographic result later confirmed no evidence of recanalization in the enhanced aneurysmal neck as showed in figure 2.
Serial HRVWI in case 5 demonstrated persistent good enhancing aneurysmal sac and wall in figure 3. The enhancement pattern of the aneurysmal neck changed from moderate enhancement to good enhancement. The minimal recanalization sac at the aneurysmal neck remained stationary and the aneurysm remained stable in the last three follow-up showed in figure 4.
Discussion and Conclusion
In this study, we evaluated the diagnostic value of HRVWI in the following-up after endovascular management and found HRVWI routinely demonstrate the enhancement pattern of the aneurysmal neck not only the aneurysmal wall in clinical patients.Angiographic follow up is gold standard for coiled aneurysms. In the angiographic study, the size of the recanalized aneurysmal neck is the most important factor deciding whether to retreat or not. Neointima was found a few months after on coiling and stent management in previous histopathologic studies8,9. The growth of vascularized tissue into an implanted coil mass or flow diverter due to inflammation or healing was described in previously publication on the enhancement of post-contrast time-of-flight MRA 10. In our series. MRA and HRVWI were joined as non-invasive follow-up tools. The enhancement of the aneurysmal wall and neck could be present superiorly on VWI with less affected by susceptibility effect in comparison to time-of-flight MRA. Nevertheless, routine MRA still provide the information while recanalization occurred. The good enhancement of aneurysmal neck might be a non-invasive sign that the endothelial healing occurred while evaluating the recanalization and reintervention.
In conclusion, HRVWI provided endothelial changes in aneurysmal neck besides routine MRA and angiographics after aneurysm treatments, increasing our confidence in making the decision whether to retreat or not.
Acknowledgements
No acknowledgement found.References
- Brinjikji W, Lanzino G, Rabinstein AA, et al. Age-related trends in the treatment and outcomes of ruptured cerebral aneurysms: a study of the Nationwide Inpatient Sample 2001–2009. AJNR Am J Neuroradiol. 2013;34:1022-27.
- Crobeddu E, Lanzino G, Kallmes DF, et al. Review of 2 decades of aneurysm-recurrence literature. Part 1. Reducing recurrence after endovascular coiling. AJNR Am J Neuroradiol. 2013;34:266-70
- Crobeddu E, Lanzino G, Kallmes DF, et al. Review of 2 decades of aneurysm-recurrence literature. Part 2. Managing recurrence after endovascular coiling. AJNR Am J Neuroradiol. 2013;34:481-85.
- Gonzalez NR, Patel AB, Murayama Y, Viñuela F. Angiographic evidence of aneurysm neck healing following endovascular treatment with bioactive coils. American journal of neuroradiology, 2005;26(4):912-914.
- Guerrero BP, Pacheco CD, Saied A, Joshi K, Rodríguez C, Martínez-Galdámez M, Lopes DK. First human evaluation of endothelial healing after a pipeline flex embolization device with shield technology implanted in posterior circulation using optical coherence tomography. Neurointervention. 2018;13(2):129.
- Larsen N, Flüh C, Madjidyar J, Synowitz M, Jansen O, Wodarg F. Visualization of Aneurysm Healing. Clinical neuroradiology. 2020;30(4):811-815.
- Larsen N, Von Der Brelie C, Trick D, Riedel CH, Lindner T, Madjidyar J, Flüh C. Vessel wall enhancement in unruptured intracranial aneurysms: an indicator for higher risk of rupture? High-resolution MR imaging and correlated histologic findings. American Journal of Neuroradiology. 2018;39(9):1617-1621.
- Kallmes DF, Ding YH, Dai D, Kadirvel R, Lewis DA, Cloft HJ. A new endoluminal, flow-disrupting device for treatment of saccular aneurysms. Stroke. 2007;38(8):2346-2352.
- Dai D, Ding YH, Kelly M, Kadirvel R, Kallmes D. Histopathological findings following pipeline embolization in a human cerebral aneurysm at the basilar tip. Interventional Neuroradiology. 2016;22(2):153-157.
- Corrêa DG, Cadete RA, da Cruz LH. Vessel Wall Enhancement in Treated Unruptured Aneurysms. American Journal of Neuroradiology. 2018;39(12):E129-E130.
Figures
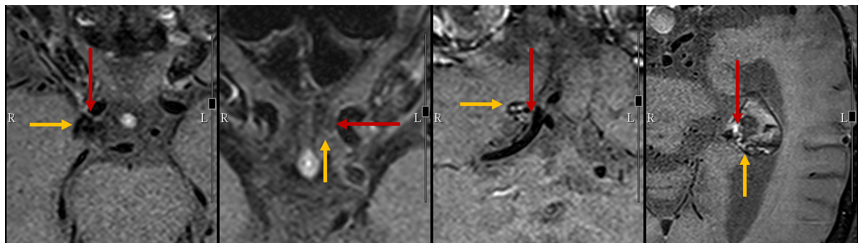
Figure 1. The
enhancement was evaluated on aneurysmal neck (red arrow) and aneurysmal wall (yellow
arrow) on post-contrast vessel wall imaging with grade 0: no enhancement, grade
1: poor enhancement, grade 2: moderate enhancement, grade 3: good enhancement. Multiple
planner reconstruction was employed to access the long-axis plane of aneurysm.
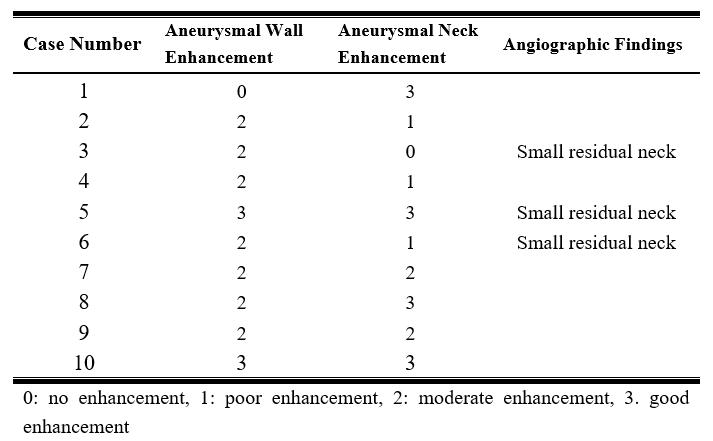
Table 1. The visualization assessment of enhancement on aneurysms in all cases.
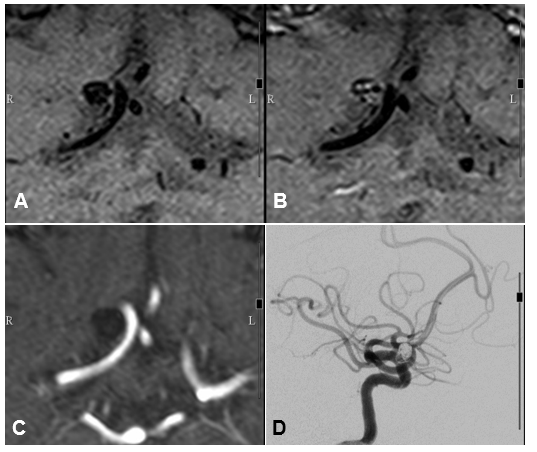
Figure
2. HRVWI before (A) and after (B) contrast median injection demonstrated
moderately enhancing aneurysmal (grade 2) wall but good enhancement (grade 3)
at the aneurysmal neck indicating sufficient neogrowth of the fibrovascular
tissue in 6 months follow-up, 3D time-of-flights MRA (C) showed no evidence of
recanalization but blooming magnetic susceptibility effect of the coils. Follow-up
angiogram (D) also showed no evidence of recanalization.
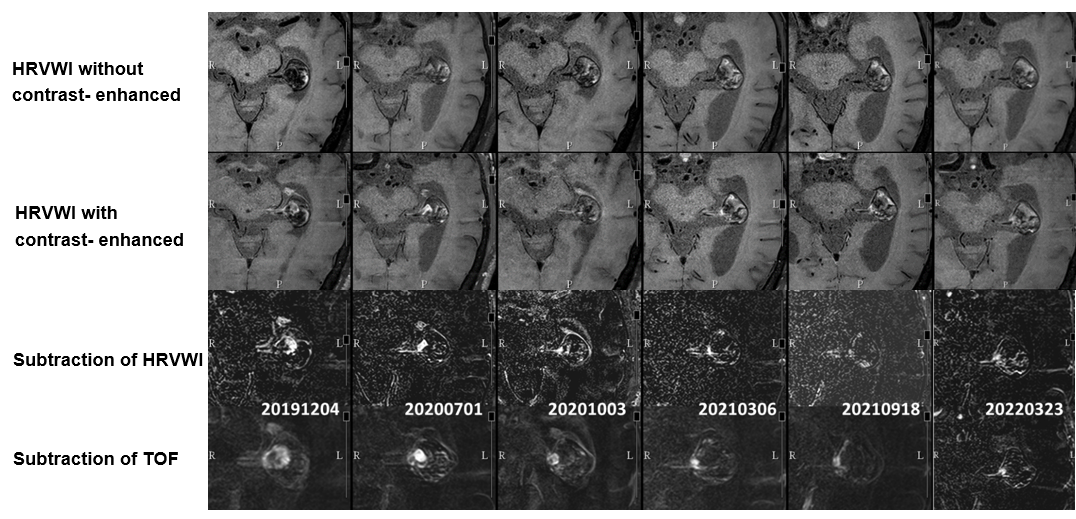
Figure 3. Serial follow-up HRVWI demonstrated
anerusymal wall enhancement and aneurysmal neck enhancement and decreased size
of the recanalized aneurysmal neck. Small residual aneurysmal neck is noted at
the last three follow up series. The subtraction images of the
contrast-enhanced and unenhanced HRVWI demonstrated the enhanced portion
clearly. The subtrationimages of enhanced and unenhanced 3D time-of-flight
source images at the corresponding slice of the HRVWI demonstrated minimal
residual neck.
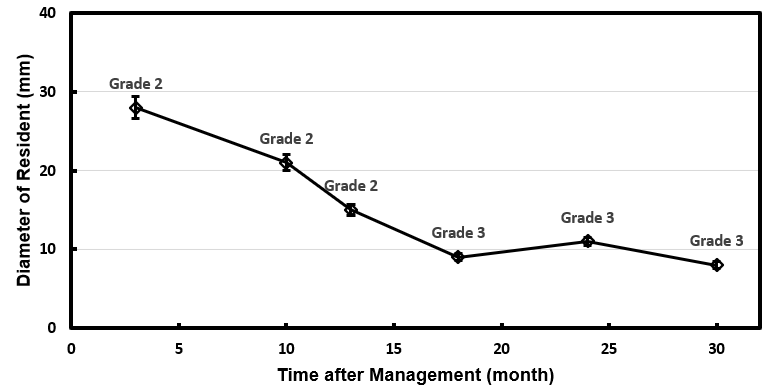
Figure 4. The
diameter recanalization resident changed throughout the time after management.
The aneurysm remained stable in the last three follow-up while the aneurysm
neck presented good enhancement (grade 3).
DOI: https://doi.org/10.58530/2023/1506