1502
Evaluation of Diffusion Kurtosis Imaging in Predicton of Tumor Budding Grade in Rectal Cancer1the First Affiliated Hospital of Dalian Medical University, Dalian, China, 2GE Healthcare (China), Beijing, China
Synopsis
Keywords: Cancer, Quantitative Imaging, tumor budding
This study used diffusion kurtosis imaging (DKI) to predict the tumor budding (TB) grade in rectal cancer. The results showed that the parameters MK, MD and their combination parameter both perform great diagnostic efficiency. DKI could noninvasively predict TB grade of rectal cancer, which is an important prognostic information, and has important guiding significance for clinical treatment.Purpose
To evaluate the value of diffusion kurtosis imaging (DKI) in prediction of tumor budding (TB) grade in rectal cancer.Introduction
Rectal cancer is one of the major causes of cancer-related mortality worldwide. Tumor budding(TB) is an emerging prognostic biomarker which are usually defined as isolated single cancer cells or clusters of up to four cancer cells located at the invasive tumour front. DKI reflect a non-Gaussian phenomenon of water molecules within biologic tissues, This study focuses on the value of diffusion kurtosis imaging (DKI) in predicting tumor budding (TB) grade of rectal cancer.Methods and Materials
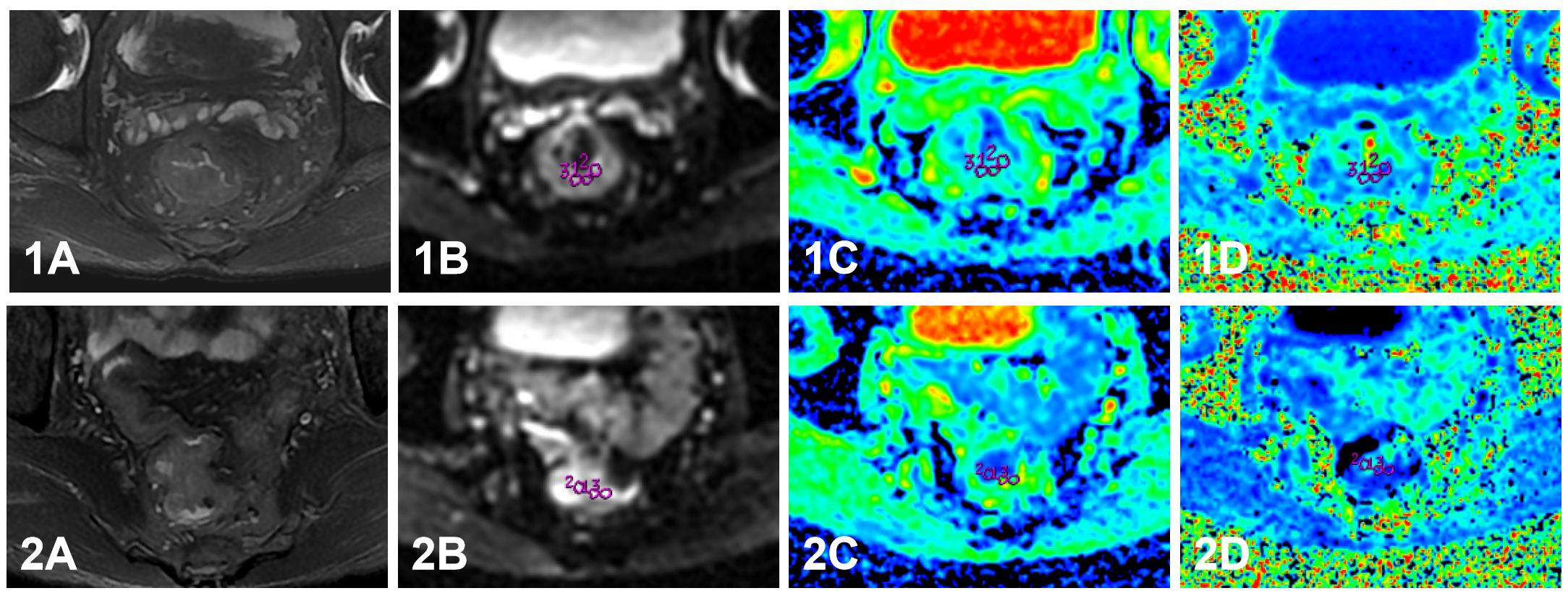
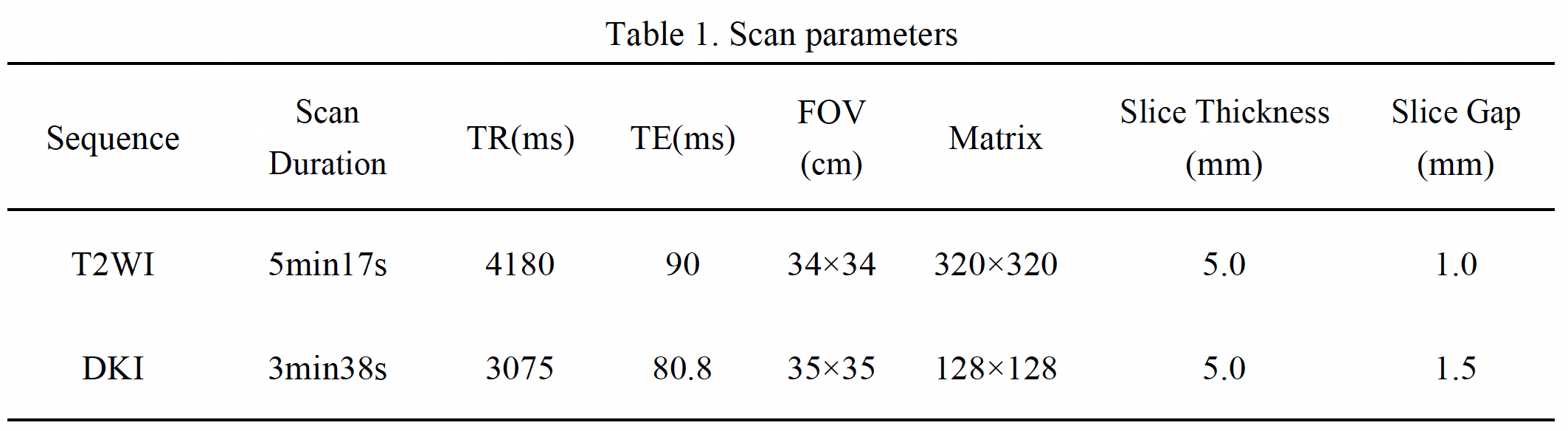
A retrospective analysis was performed on 66 rectal cancer patients confirmed with tumor budding according to their postoperative pathology results. They were divided into group 1 (low and intermediate TB grade; 38 patients; 28 male, 9 female,mean age: 63.50±9.45 years, range: 36-89 years) and group 2 (high TB grade; 28 patients, 19 male, 9 female, mean age: 66.14±8.92 years, range: 44-84 years) according to their TB grades. All participants underwent T2WI、DKI scans on a 3.0T MRI scanne(GE Signa HDXT) before surgery. Detailed scan parameters were listed in Table 1. The DKI images were post-processed using FuncTool software on AW4.6 workstation. Three region of interests (ROIs) were put on the largest slice of tumors, avoiding bleeding, necrosis, and cystic degeneration. Statistical analyses were carried out with SPSS 26.0 (IBM) and MedCalc 11.4. The Shapiro–Wilk test was used to determine whether the variables were normally distributed. Mann-Whitney U test or Independent Sample t-test was used to compare the differences between two groups. Logistic regression and receiver operating characteristic (ROC) curve analyses were performed to evaluate the diagnostic efficiency of the parameters. Differences in the area under the curves (AUCs) of different parameters were compared using the DeLong test.Results
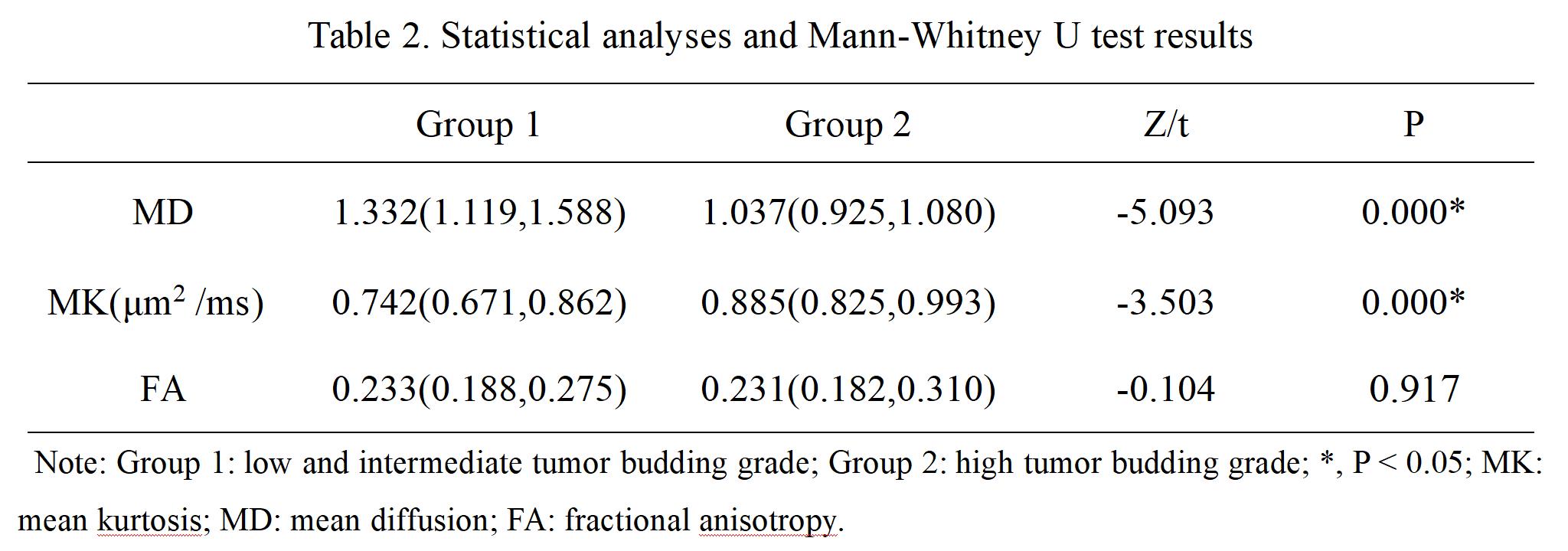
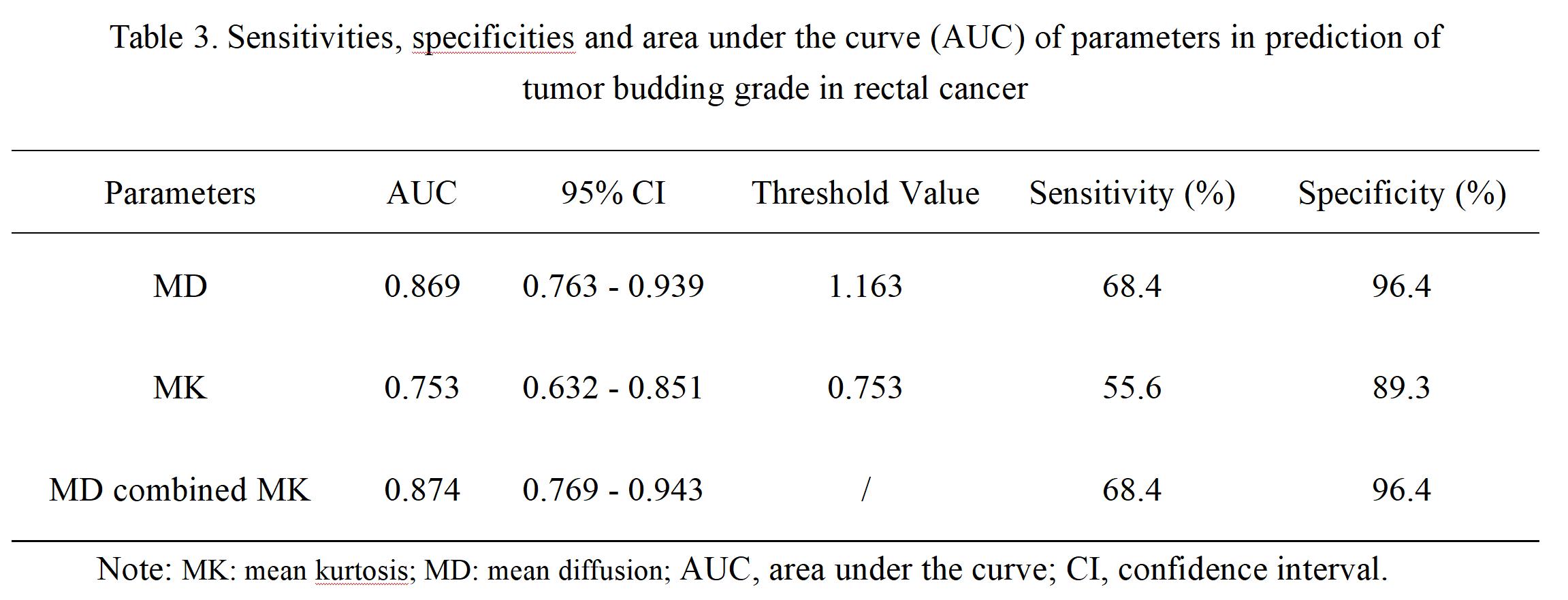
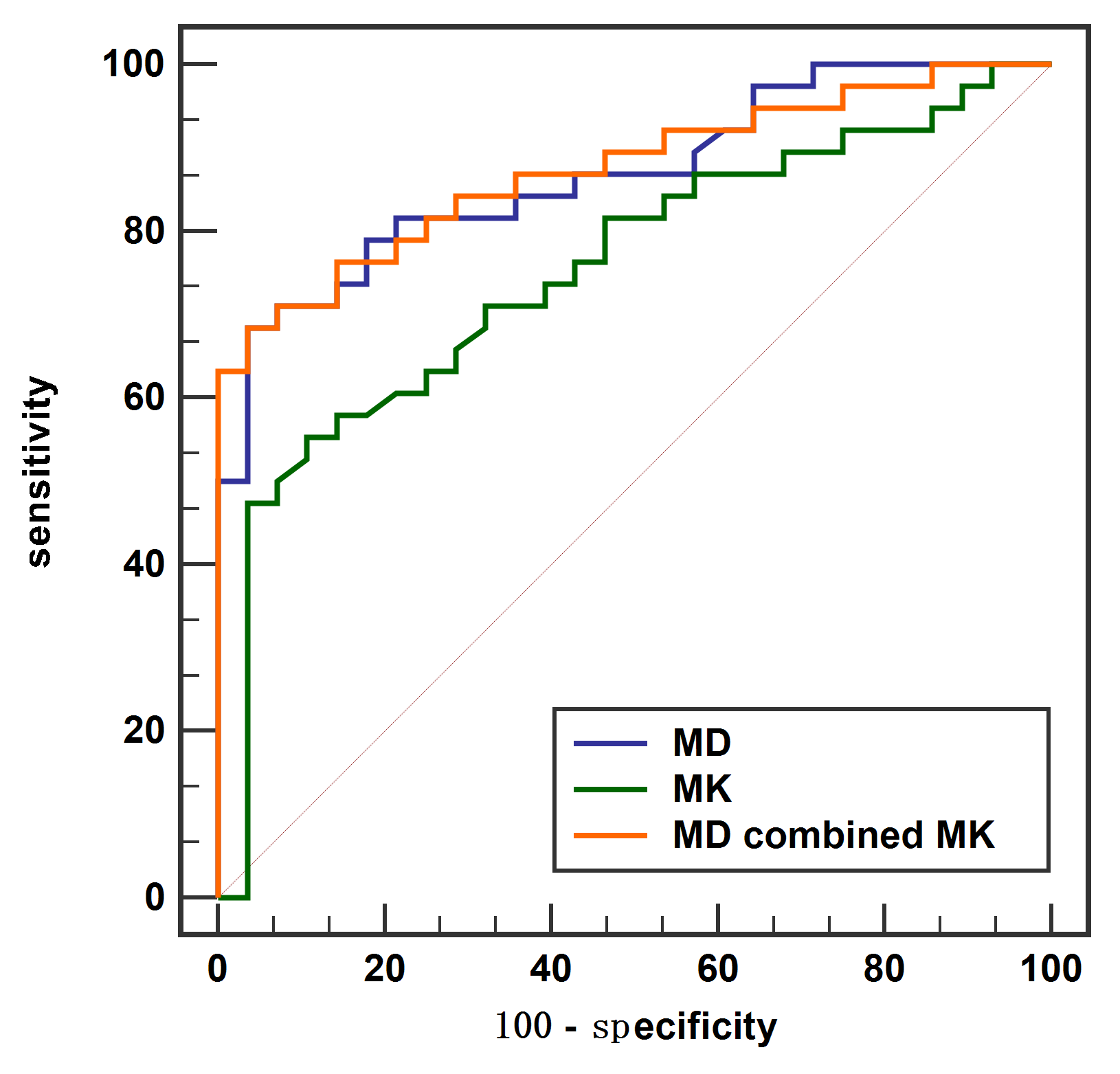
Group 1 had significantly lower mean kurtosis (MK) values and higher mean diffusion (MD) values than group 2 (P < 0.05)(Table 2). There was no difference of fractional anisotropy (FA) values between two groups. The AUC values for the ROC analyses of MK and MD values for differentiation two groups was 0.753 and 0.869, respectively (Figure 2). The AUC value of combined parameter was 0.874, with a sensitivity of 68.4% and specificity of 96.4% (Table 3). The combination of MD and MK did not improve the diagnostic efficiency than single parameters.Discussion
A large number of previous studies have shown that TB has a high value in the prognosis of patients with colorectal cancer, and can reflect the invasiveness of the tumor to a certain extent [1]. Group 1 had significantly lower MK value than group 2, which might be related to the complexity of the microstructure in low and intermedium budding group (such as cell density, cell atypia and nuclear pleomorphism, etc.) [2]. Group 1 had significantly higher MD value than group 2, which might because high TB grade group has more necrosis area and the structure of tissue is relatively loose, thus the degree of diffusion limitation of water molecules is low [3-4]. MK and MD values both performed great diagnostic efficiency in prediction of TB grade, while MD values showed the greatest diagnostic efficiency.Conclusions
DKI could noninvasively predict TB grade of rectal cancer, which is an important prognostic information, and has important guiding significance for clinical treatment.Acknowledgements
None.References
1. Liu S, Zhang Y, Ju Y, Li Y, Kang X, Yang X, Niu T, Xing X, Lu Y. Establishment and Clinical Application of an Artificial Intelligence Diagnostic Platform for Identifying Rectal Cancer Tumor Budding. Front Oncol. 2021 Mar 8;11:626626. doi: 10.3389/fonc.2021.626626. PMID: 33763362; PMCID: PMC7982570.
2.Yim K, Jang WM, Cho U, Sun S, Chong Y, Seo KJ. Intratumoral Budding in Pretreatment Biopsies, among Tumor Microenvironmental Components, Can Predict Prognosis and Neoadjuvant Therapy Response in Colorectal Adenocarcinoma. Medicina (Kaunas). 2022 Jul 12;58(7):926. doi: 10.3390/medicina58070926. PMID: 35888645; PMCID: PMC9324564.
3. Trotsyuk I, Sparschuh H, Müller AJ, Neumann K, Kruschewski M, Horst D, Elezkurtaj S. Tumor budding outperforms ypT and ypN classification in predicting outcome of rectal cancer after neoadjuvant chemoradiotherapy. BMC Cancer. 2019 Nov 1;19(1):1033. doi: 10.1186/s12885-019-6261-5. PMID: 31675950; PMCID: PMC6824112.
4. Fujiyoshi K, Väyrynen JP, Borowsky J, Papke DJ Jr, Arima K, Haruki K, Kishikawa J, Akimoto N, Ugai T, Lau MC, Gu S, Shi S, Zhao M, Da Silva AFL, Twombly TS, Nan H, Meyerhardt JA, Song M, Zhang X, Wu K, Chan AT, Fuchs CS, Lennerz JK, Giannakis M, Nowak JA, Ogino S. Tumour budding, poorly differentiated clusters, and T-cell response in colorectal cancer. EBioMedicine. 2020 Jul;57:102860. doi: 10.1016/j.ebiom.2020.102860. Epub 2020 Jul 8. PMID: 32652320; PMCID: PMC7347996.
Figures