1493
MRI assessment of abscopal effect enhanced by immune checkpoint blockade1National Cancer Institute, Bethesda, MD, United States
Synopsis
Keywords: Cancer, DSC & DCE Perfusion
Radiation therapy (RT) on primary tumor rarely induces regression of non-irradiated metastatic lesions (abscopal effect), which is reported to be enhanced by immune-checkpoint blockade. In this study, we examined the physiological changes induced by abscopal effect using MRI-based imaging modalities such as EPR oximetry, DCE MRI, and 13C DNP MRI. Hypoxic fraction < 10 mmHg (HF10), permeability, perfusion, and CD8+ T cell infiltration in metastatic tumor increased after the combination of RT and PD-1 blockade. Interestingly, higher permeability/perfusion and lower HF10 in primary tumor before the treatment were associated with slower growth of the metastatic tumor after the treatment.
Introduction
It has been reported that radiation therapy (RT) on primary tumor rarely causes regression of non-irradiated metastatic lesions, which is called abscopal effect (AE). AE arises from systemic anti-tumor immune responses induced by localized RT on primary tumor. The radiation-mediated systemic anti-tumor effects are induced by an activation of tumor-specific CD8+ T cells which are primed by antigen-presenting cells that capture tumor-specific antigens from the collapsed tumor. 1 The primed CD8+ T cells can induce apoptosis of tumor cells at distant non-irradiated sites through Fas/Fas ligand and/or Perforin/Granzyme B pathways. 2 However, the overall occurrence rate of the AE by RT alone is extremely low because such anti-tumor effects are inhibited by an adaptive immune resistance mechanism including PD-1/PD-L1 pathway.3 Although it has been reported that immunotherapy, especially immune checkpoint blockade (ICB), can enhance AE, the imaging biomarkers accosiated with the AE have not been investigated to date.4The tumor microenvironment (TME) is tightly related to the local immune function. Hence, in the current study, we investigated pO2 distribution, permeability, perfusion and glycolytic metabolism in the primary/metastatic tumors treated with the combination therapy to explore the physiological and metabolic changes in the tumors showing AE.
Methods
MC38 colon adenocarcinoma treated with RT and PD-1 inhibitor were used to evaluate the AE . For in vivo treatment model, 1x106 tumor cells and 2x105 were inoculated subcutaneously into right (primary) and left (metastatic) hindlegs of C57BL/6 mice, respectively. Four treatment groups were prepared as described in Fig.1.Electron paramagnetic resonance imaging (EPRI) were performed for quantitative intra-tumor pO2 mapping with high resolution (~0.2mm) by observing the linewidth of the exogenously administered trityl radical probe Ox063.
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) and Apparent Diffusion Coefficiency (ADC) mapping were performed on a 3 T scanner. T1-weighted fast low-angle shot (FLASH) images were obtained with TR = 117.2 ms; TE = 6 ms; flip angle = 30˚; two slices; 28 x 28 mm resolution; 15-second acquisition time per image; and 45 repetitions. Gd-DTPA solution (4 mL/g of body weight of 50 mmol/L Gd-DTPA) was injected through a tail vein cannula 1 minutes after the start of the dynamic FLASH sequence. To determine the local concentrations of Gd-DTPA, T1 maps were calculated from three sets of Rapid Imaging with Refocused Echoes (RARE) with the acquisitions being made before running the FLASH sequence.
Multisection Diffusion Weighted imaging (DWI) were processed to generate the trace ADC maps based on the signal intensity of b0 = 0 and b1 = 200, 500, or 1000 s/mm2.
13C hyperpolarized MRI: Hyperpolarized 13C MRI studies were performed on BioSpec 3T (Bruker). Hyperpolarized [1–13C] pyruvate was rapidly injected intravenously (20 μL/g). Chemical-shift imaging images were acquired 30 s after the Hyperpolarized [1–13C] pyruvate injection with following parameters; FOV 28 × 28 mm, slice thickness 8 mm, matrix size 14 × 14, spectral width of 5000 Hz, repetition time 60 ms, and excitation pulse with a flip angle of 5.
Flowcytometry: To analyze tumor infiltrating lymphocytes (TILs), on day 9 after treatment, single-cell suspensions were prepared from left hind leg tumor. The cell surface phenotypes were determined by direct immunofluorescence staining with aCD3, aCD8, and aCD4 antibody and analyzed using FACS Calibur. TILs were identified and gated on a forward scatter versus side scatter plot.
Results and Discussion
A mouse tumor model exhibiting AE induced by the combination of RT and PD-1 blockade was established using MC38 tumors. Combination of RT and PD-1 blockade showed a synergistic effect on metastatic tumors (Fig.1). Flow cytometry showed that CD8+ T cell infiltration in metastatic tumors increased after the combination of RT and PD-1 blockade (Fig.2), suggesting that in vivo synergistical effect was caused by enhanced CD8+ T cell infiltration. Hypoxic fraction < 10 mmHg (HF10), permeability, perfusion and inflammation in metastatic tumors improved after the combination of RT and PD-1 blockade (Fig.3 and 4), suggesting that enhanced CD8+ T cell infiltration by the AE was associated with the changes in these imaging biomarkers. Hyperpolarized 1-13C Pyruvate MRI showed that the combination of RT and PD-1 blockade did not alter glycolytic profiles in metastatic tumors (Fig.5). Interestingly, the biomarkers in TME (high Permeability, Perfusion, and low HF10) before treatment were found to correlate to the extent of AE induction (Fig.6), which may imply that the condition in TME while the primary tumors were irradiated has a significant impact on the induction of AE.Conclusion
Hypoxic fraction < 10 mmHg, permeability, perfusion and CD8+ T cell infiltration in metastatic tumors improved after the combination of RT and PD-1 blockade. Higher permeability/perfusion and lower HF10 in primary tumor before the treatment were associated with slower metastatic tumor growth after the treatment. These data suggested that the imaging biomarkers potentially predict the successful AE after the combination of RT and PD-1 blockade.Acknowledgements
No acknowledgement found.References
1. Wang, D.; Zhang, X.; Gao, Y.; Cui, X.; Yang, Y.; Mao, W.; Li, M.; Zhang, B.; Yu, J., Research Progress and Existing Problems for Abscopal Effect. Cancer Manag Res 2020, 12, 6695-6706.2. Henkart, P. A., Lymphocyte-mediated cytotoxicity: two pathways and multiple effector molecules. Immunity 1994, 1 (5), 343-6.
3. Taube, J. M.; Anders, R. A.; Young, G. D.; Xu, H.; Sharma, R.; McMiller, T. L.; Chen, S.; Klein, A. P.; Pardoll, D. M.; Topalian, S. L.; Chen, L., Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci Transl Med 2012, 4 (127), 127ra37.
4. Liu, Y.; Dong, Y.; Kong, L.; Shi, F.; Zhu, H.; Yu, J., Abscopal effect of radiotherapy combined with immune checkpoint inhibitors. J Hematol Oncol 2018, 11 (1), 104.
Figures
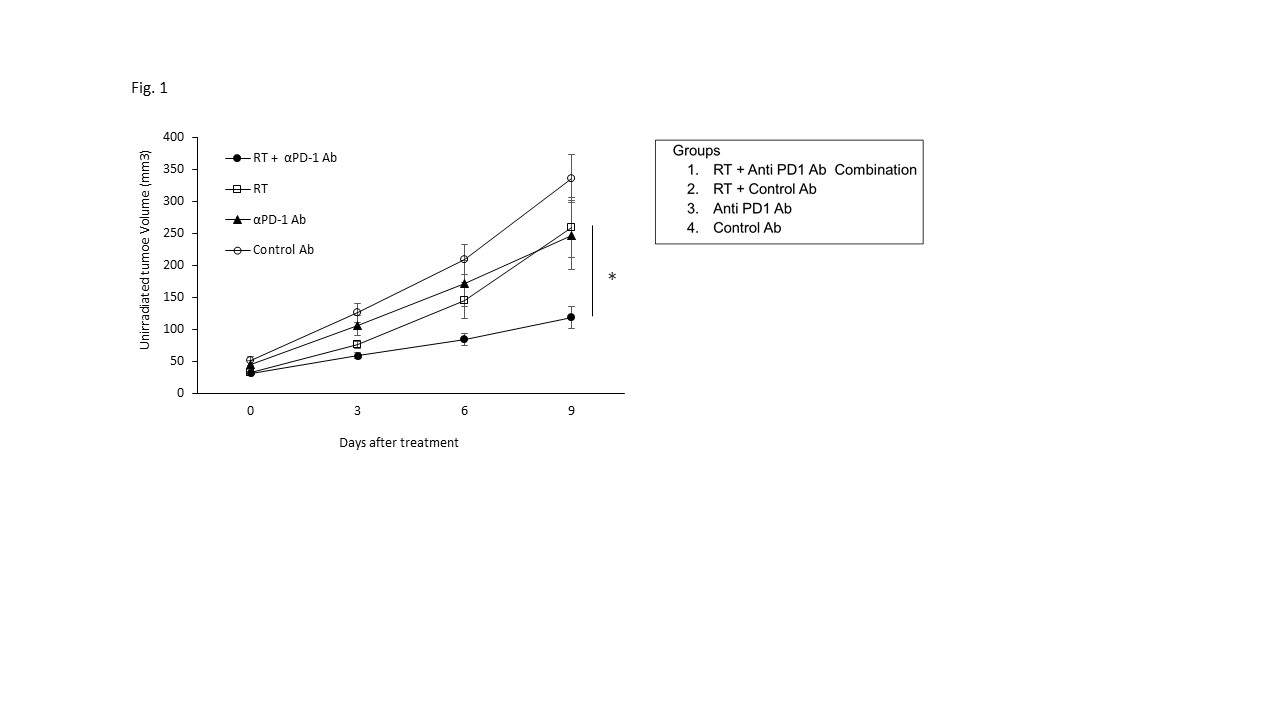
Figure 1. Tumor growth of the combination treatment of RT and PD-1 inhibitor in MC38 murine tumor model. Growth kinetics of MC38 mouse metastatic tumor on left leg. MC38 inoculated mice were treated with either combination of RT and PD-1 inhibitor or RT alone or PD-1 inhibitor alone or IgG isotype antibody (n = 10 per group). Only right leg tumor was irradiated, Data are shown as mean ± SE at each time point. Statistical significance between groups was determined by Student t test. *p < 0.05.
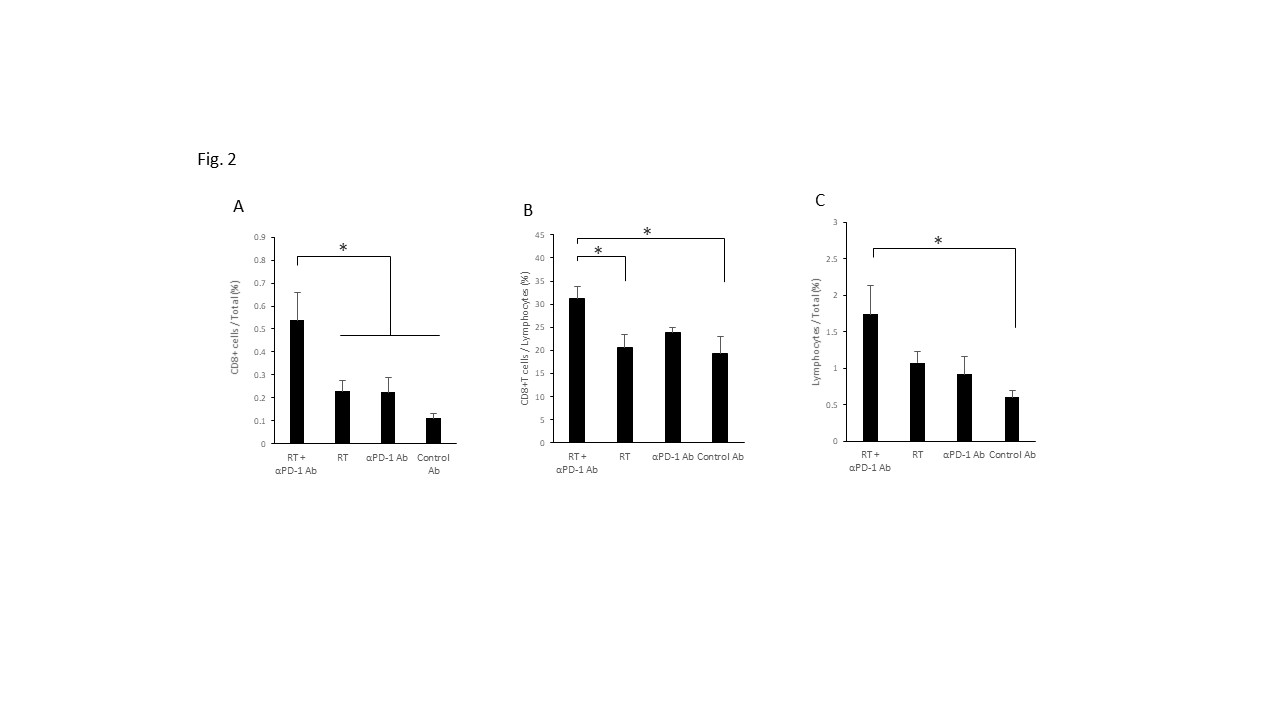
Figure 2. Flow cytometry analysis of tumor infiltrating lymphocytes (TILs) (A) The percentage of CD3+CD8+ T cells to total tumor cells in each group. (B) The percentage of CD3+CD8+ T cells to lymphocytes in each group. (C) The percentage of lymphocytes to total tumor cells in each group. (n = 5 per group) Data are shown as mean ± SE. Statistical significance between groups was determined by Student t test. *p < 0.05.
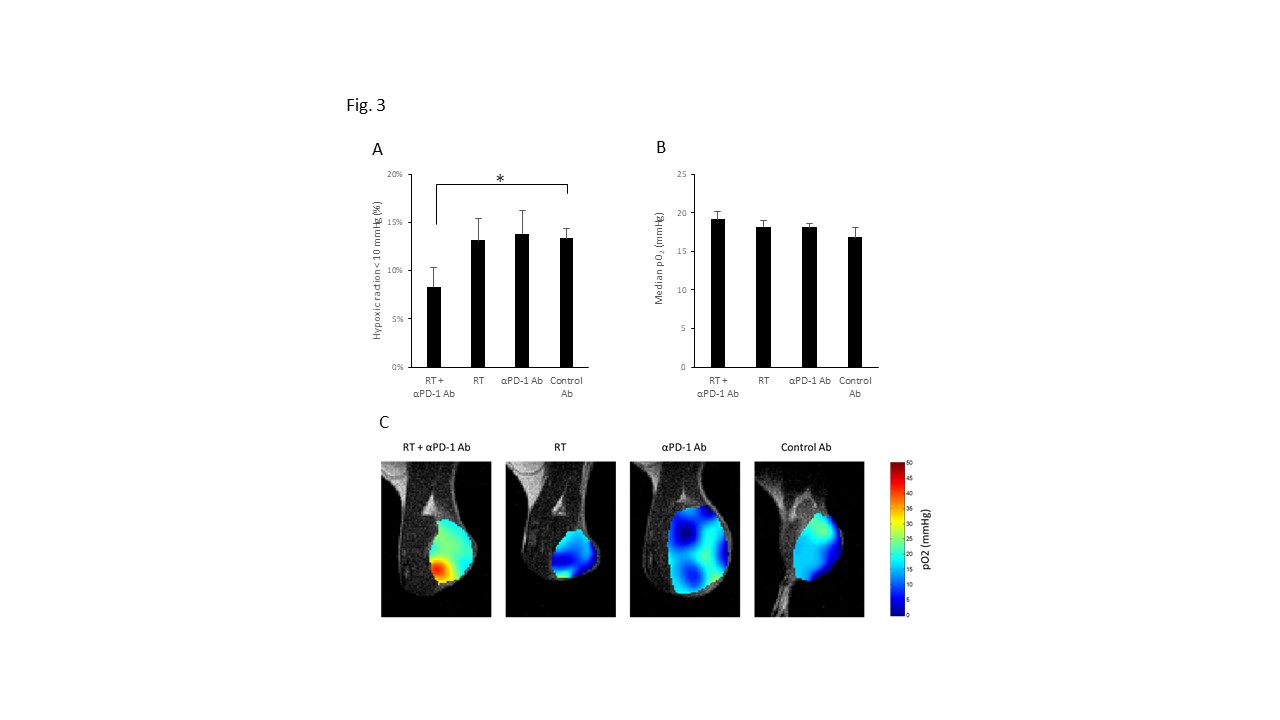
Figure 3. EPR imaging on MC38 tumor after combination treatment. Intra-tumor pO2 mapping were performed on day 9 after treatment on unirradiated left hindleg tumor (n = 10 per group). (A) Hypoxic fraction < 10 mmHg (HF10). (B) Median pO2. (C) pO2 maps in MC38 tumor. Data are shown as mean ± SE. Statistical significance between groups was determined by Student t test. *p < 0.05.
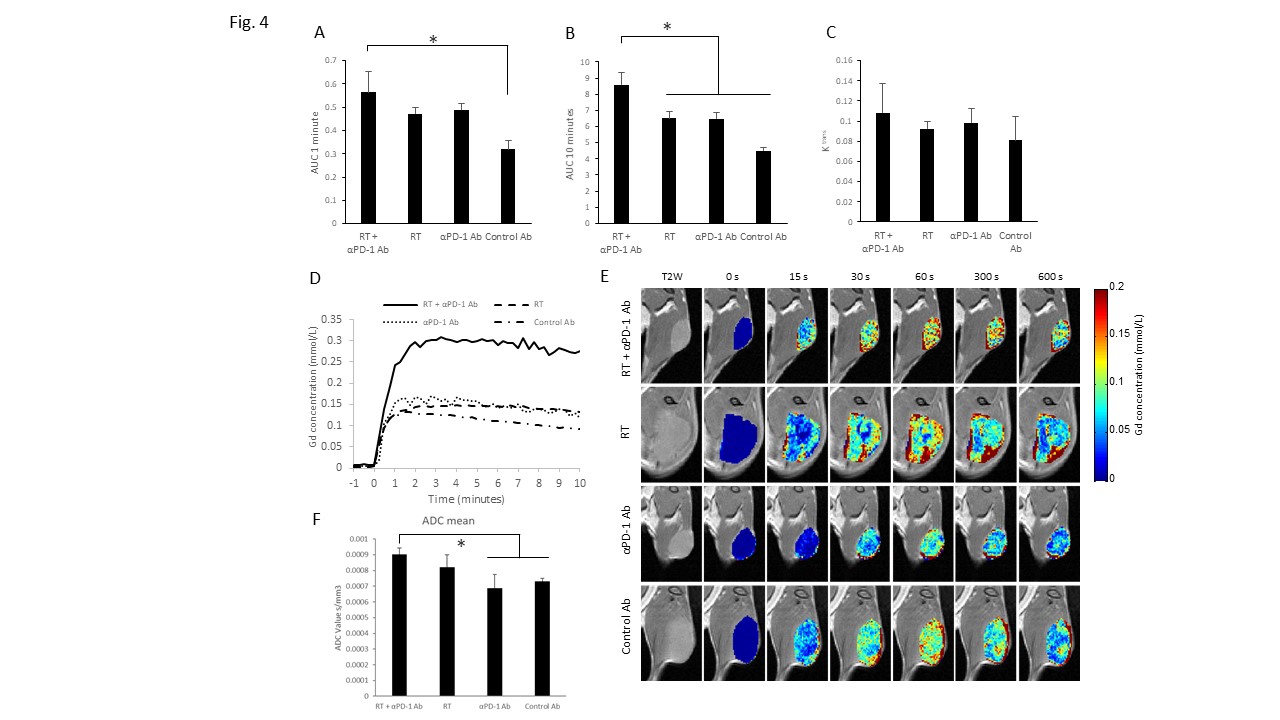
Figure 4. DCE-MRI and ADC mapping on MC38 tumor after the combination treatment. Permeability and perfusion analysis on MC38 tumor model. Imaging were performed on day 9 on unirradiated left hindleg tumor in each group (n = 6 per group). (A) Area under curve (AUC) 1 min; Perfusion, (B) AUC 10 min; Permeability, (C) Ktrans, (D) Representative time-intensity kinetic curve of Gd-DTPA in MC38 tumor, (E) Gd-DTPA intensity with T2-weighted anatomical image of MC38 tumor. (F) ADC mapping. Data are shown as mean ± SE.
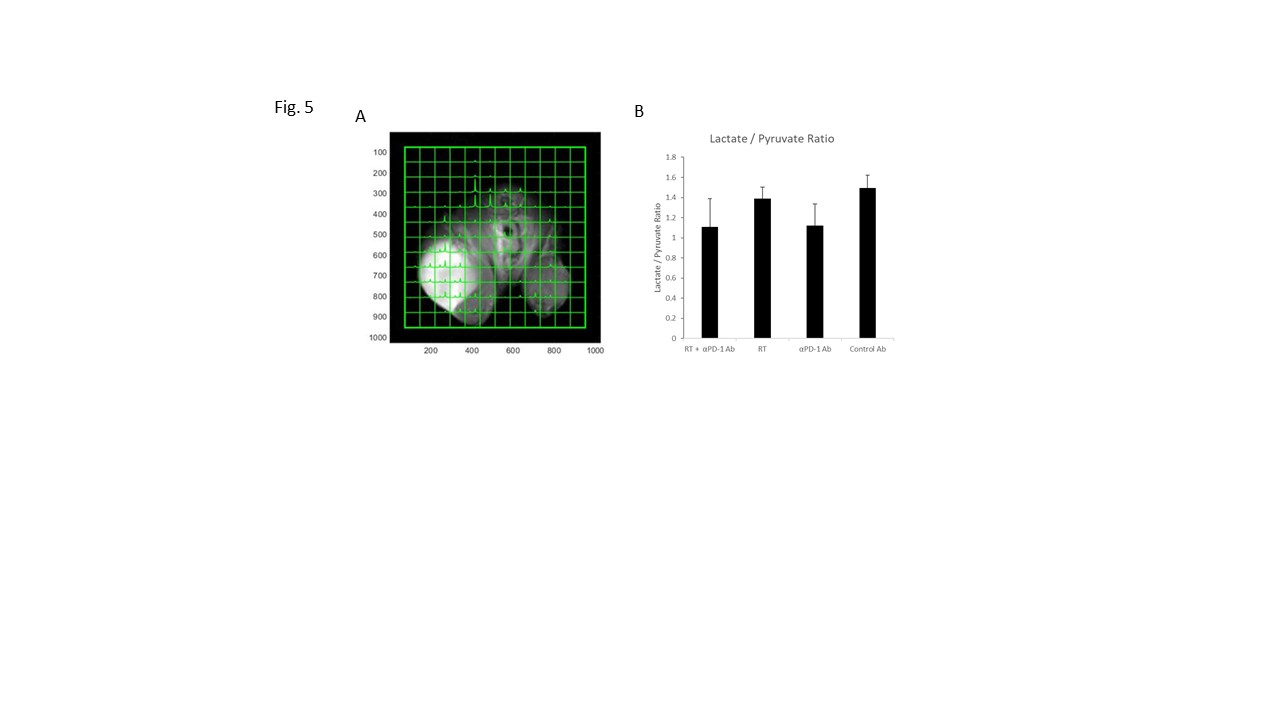
Figure 5. Evaluation of glycolysis on MC38 tumor. Hyperpolarized 1-13C Pyruvate MRI were performed on day 9 on unirradiated left hindleg tumor in each group (n = 8 per group). Chemical-shift imaging (A) The chemical shift images were superimposed on grayscale T1-weighted proton images, Representative data of tumor in combination of RT and PD-1 inhibitor group. (B) Lactate to pyruvate ratio. Data are shown as mean ± SE.
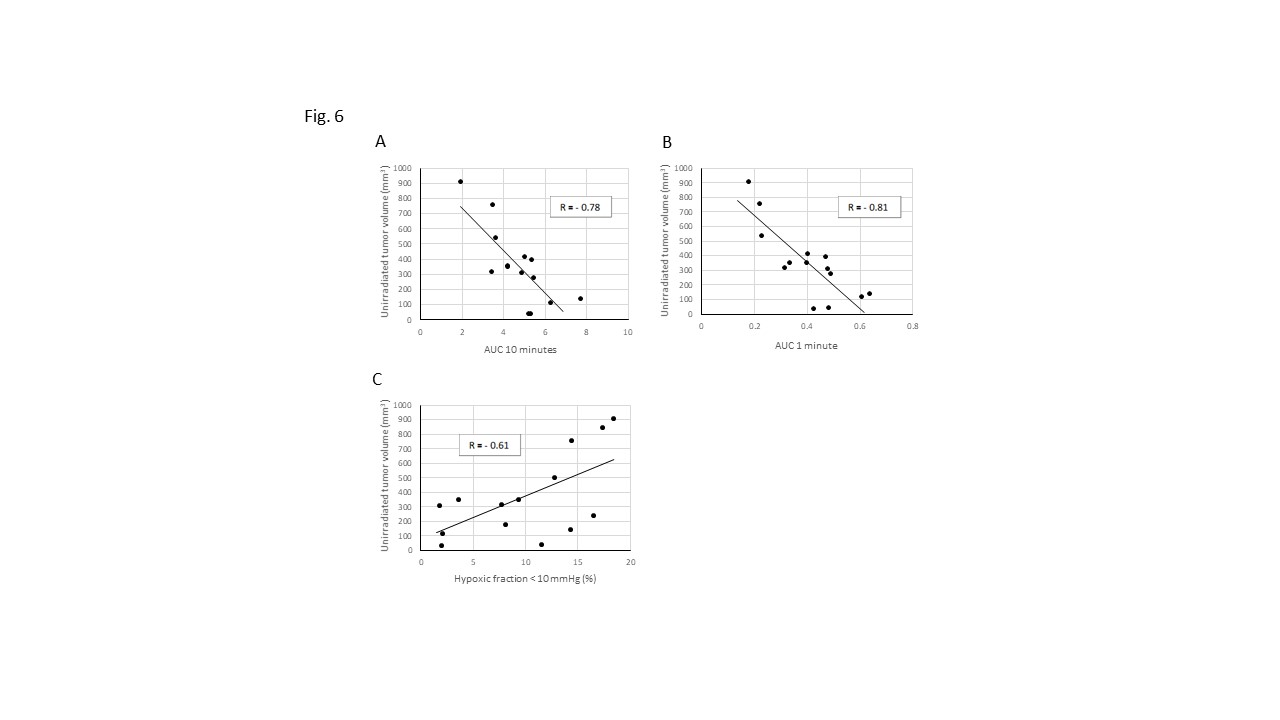
Figure 6. Correlation between pre-treatment imaging data and post-treatment tumor growth. Pre-treatment DCE-MRI and EPR imaging were performed on right hindleg tumor before the combination treatment of RT and PD-1. Post-treatment tumor growth on unirradiated left hindleg tumor were evaluated on day 9 after the combination treatment of RT and PD-1. (A-C) The correlation between unirradiated tumor volume on day 9 after treatment and pre-treatment permeability (A), perfusion (B), HF10 (C) on irradiated tumor. (n = 14)