1474
Predictive Model for Breast Lesion Assessment Using Restriction Spectrum Imaging1Radiology, University of California, San Diego, San Diego, CA, United States, 2Radiation medicine, University of California, San Diego, San Diego, CA, United States, 3Bioengineering, University of California, San Diego, San Diego, CA, United States, 4Radiology, Beth Israel Hospital, Boston, MA, United States, 5Harvard Medical School, Boston, MA, United States, 6Commonwealth Radiology Associates, Boston, MA, United States, 7Neurosciences, University of California, San Diego, San Diego, CA, United States, 8American College of Radiology, Reston, VA, United States, 9Biostatistics, Herbert Wertheim School of Public Health and Human Longevity Science, University of California, San Diego, San Diego, CA, United States
Synopsis
Keywords: Breast, Diffusion/other diffusion imaging techniques
Diffusion weighted imaging (DWI) holds great potential in improving specificity of findings detected on contrast enhanced breast MRI. Restriction spectrum imaging (RSI), an advanced diffusion imaging model, has potential in discriminating between malignant and fibroglandular breast tissue. In this abstract, we evaluate RSI’s performance, combined with a random forest model, in differentiating lesions requiring biopsies from lesions that do not. The model showed significant preliminary results.Introduction
Breast cancer MRI screening protocols include dynamic contrast-enhanced (DCE) imaging for lesion detection and assessment. DCE has variable specificity (61-97%)1, requiring biopsies for final diagnosis. Diffusion-weighted imaging (DWI) is now often part of cancer screening protocols, aiming at improving specificity. Minimizing unnecessary biopsies is a challenge with both clinical and economic implications. DWI is widely used, but more advanced models such as restriction spectrum imaging (RSI) aim to separate signal components in different degrees of diffusion (free, hindered and restricted). An RSI breast-specific model was developed on cancers greater than 2cm in size2, and has shown potential in distinguishing cancers from healthy tissue3, but also in discriminating cancers from benign lesions4. In this study, we explore and evaluate the performance of the RSI outputs with a random forest model as a potential breast lesion predictor on a prospective study, performed on a breast cancer screening cohort.Methods
Women were recruited in two cohorts from a screening population– after screening mammography interpreted as BIRADS-0 with subsequent diagnostic work-up leading to the recommendation for biopsy or undergoing routine screening MRI due to high-risk status. A total of 187 women were prospectively scanned, of which 72 had at least either one malignant or one benign lesion and corresponding RSI data. A total of 89 lesions were identified. Lesions were then separated as 41 average-risk lesions (ARL), 13 high-risk lesions (HRL) and 35 cancers (CL). All lesions were assessed via core needle biopsy.Data were collected using a 3.0T wide-bore (Discovery MR750w, GE Healthcare, USA) and an 8-ch Sentinel breast coil. Reduced field-of-view (FOV) DW-MRI and DCE were collected. DW-MRI data were processed using Matlab (R2017a, Mathworks, USA) and were distortion corrected using the reverse polarity gradient (RPG) method5, followed by noise and eddy current corrections. Finally, datasets were normalized by the 98th percentile of the b= 0 s/mm2 images. Pre-processed data of all patients were fit to the breast RSI model2 to generate signal contribution maps of components C1, C2, C3:
$$ S(b) = C_1 + C_2e^{-b×1.4×10^{-3}} + C_3e^{-b×10.3×10^{-3}} $$
The outputs are hypothesized to correspond to cancer and fatty tissue (C1), fibroglandular tissue (C2), and vascular flow (C3), respectively. The square root of C1C2 was calculated, as well as the ratio $$$ \frac{C_1C_2}{C_3}$$$ (and divided 10-fold to better account for scaling) from Ci values in each ROI. All lesions were 3D-delineated using ITK-SNAP6 under the supervision of a radiologist, based on suspicious findings detected on DCE-imaging corresponding to biopsied tissue. Control ROIs were drawn in healthy fibroglandular tissue, while avoiding any breast lesion, once for each patient that had at least one biopsied lesion.
A random forest model was fit to the data, with the outcome as the type of lesion: control (healthy), ARL, HRL, and CL, and the predictors of interest include C1, C2, C3, square root of C1C2, and $$$ \frac{C_1C_2}{10C_3}$$$ . The control and ARL types were combined into one type as no biopsy is required for both types, while HRL and CL were combined as they both require biopsy and close follow-ups and treatment/surgery.
The data of lesions were randomly split into a training set (90% of lesions) and a set-apart test set (10% of lesions). Then a random forest model was fit to the training set only without using data from the test set. Parameters in the random forest model were determined using a 5-fold cross validation. The model trained with only the training set was then applied to the test set.
Results
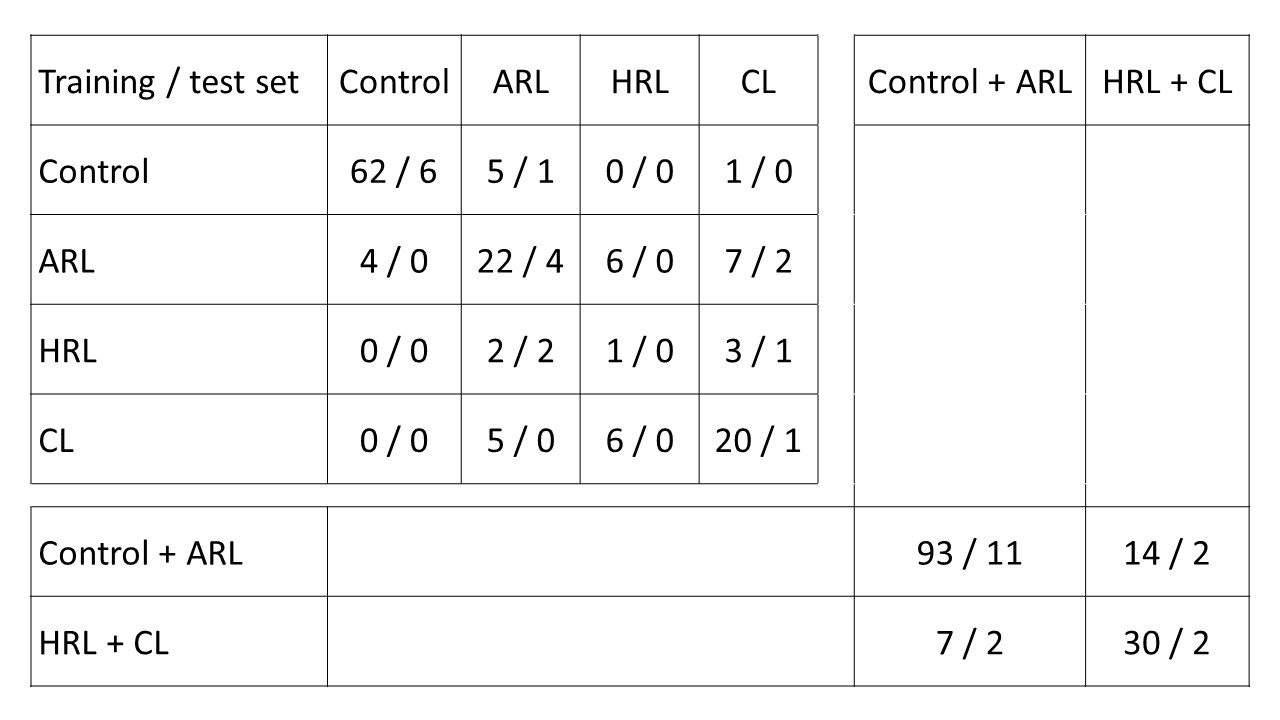
The prediction with regrouped population (control + ARL vs HRL + CL) accuracy is 85% with 95% CI: (79%, 91%) in the training set and 0.76 with 95% CI: (50%, 93%) in the test set. Classification results are shown in confusion matrices in Table 1.Discussion
In this study, we propose a random forest model for breast lesion classification. Preliminary results have demonstrated potential in improving diagnostic specificity, especially when regrouping lesion in two groups “no biopsy required” (control + ARL) versus “biopsy required” (HRL + CL). Minimizing unnecessary biopsies is crucial for patient care, and a high-performing model would help reduce unnecessary procedures for patient and health care expenses.Next steps to improve the model will start with including more lesions in the dataset, especially high-risk lesions as there are fewer (only 13 compared to 41 ARL and 35 CL). With optimal sample size, a more comprehensive analysis will be performed, including optimizing data partitioning for model training.
Finally, the model would benefit from better, high-resolution DWI acquisitions. Parallel-imaging techniques, such as multi-slice excitation, could help improve through-plane resolution and provide better datasets for model training.
Acknowledgements
No acknowledgement found.References
1. Kriege M, Brekelmans CTM, Boetes C, et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351(5):427-437. doi:10.1056/NEJMoa031759
2. Rodríguez-Soto AE, Fang LK, Holland D, et al. Correction of Artifacts Induced by B0 Inhomogeneities in Breast MRI Using Reduced-Field-of-View Echo-Planar Imaging and Enhanced Reversed Polarity Gradient Method. J Magn Reson Imaging. 2021;53(5):1581-1591. doi:10.1002/jmri.27566
3. Andreassen MMS, Rodríguez-Soto AE, Conlin CC, et al. Discrimination of Breast Cancer from Healthy Breast Tissue Using a Three-component Diffusion-weighted MRI Model. Clin Cancer Res. 2021;27(4):1094-1104. doi:10.1158/1078-0432.CCR-20-2017
4. Besser AH, Fang LK, Tong MW, et al. Tri-Compartmental Restriction Spectrum Imaging Breast Model Distinguishes Malignant Lesions from Benign Lesions and Healthy Tissue on Diffusion-Weighted Imaging. Cancers. 2022;14(13):3200. doi:10.3390/cancers14133200
5. Holland D, Kuperman JM, Dale AM. Efficient correction of inhomogeneous static magnetic field-induced distortion in Echo Planar Imaging. NeuroImage. 2010;50(1):175-183. doi:10.1016/j.neuroimage.2009.11.044
6. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. NeuroImage. 2006;31(3):1116-1128. doi:10.1016/j.neuroimage.2006.01.015
Figures