1451
An initial evaluation of image quality for double knee imaging with air coil as compared with traditional knee coils1General Hospital of Pingmei Shenma Group, Pingdingshan, China, 2GE Healthcare, MR Research, Beijing, China
Synopsis
Keywords: Joints, Joints
This study investigated the feasibility and potential advantages of adaptive imaging receiver (AIR) coil for knee imaging. The results show that the SNR and CNR of air coil images were inferior to that of traditional knee coil, but the visual image qualities were comparable between two coils. The air coil can be feasible for knee imaging, especially for patients with large size and double knee imaging.Background
Traditional phased-array knee coils are designed with fixed geometry to generate uniform RF field inside the volume, increase SNR and allow higher acceleration [1]. Though high-quality image can be obtained for usual situations, the rigid design also limits the utility for patients with large size or double knee imaging in as little time as possible. Adaptive image receive (AIR) coil is the new light and ultra-flexible coil constructed with inca fiber guide ring structure, which allow the coil fitting various shape and size, and closely wrapping anatomy. Due to significantly reduced mutual inductance and capacitive coupling between coil elements, air coil accommodates ultra-high density coil elements to obtain high quality images [2]. Air coil has been applied in brain[3], lung[4] and abdomen[5,6], and demonstrated improved performance and patient comfort as compared to traditional coil. This study is to initially evaluate the feasibility and performance of air coil for knee imaging and explore the potential benefit in compare with traditional rigid coil.Methods
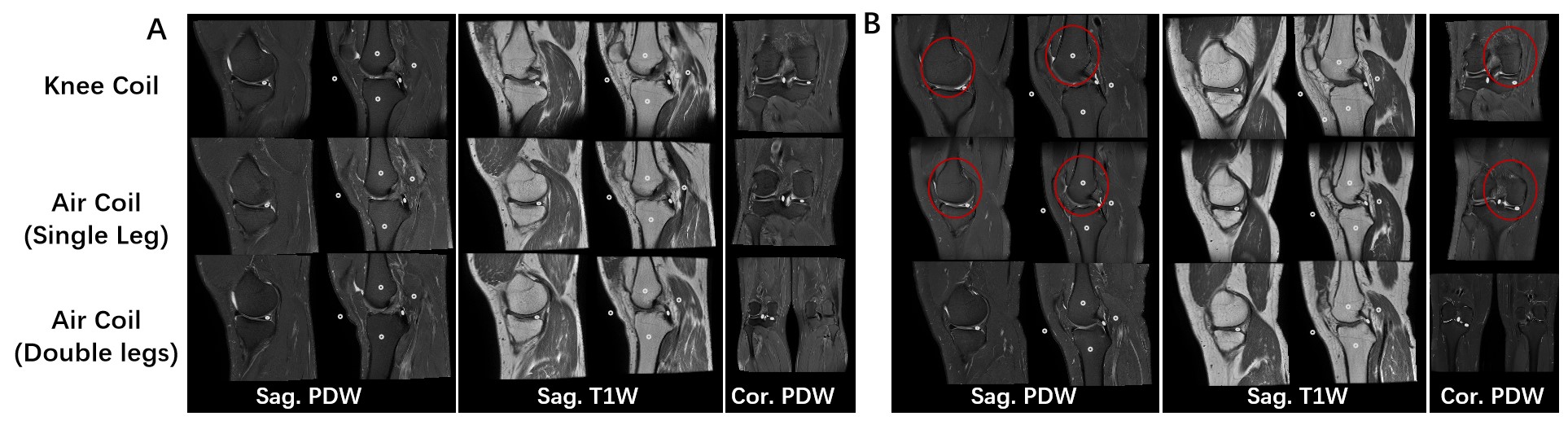
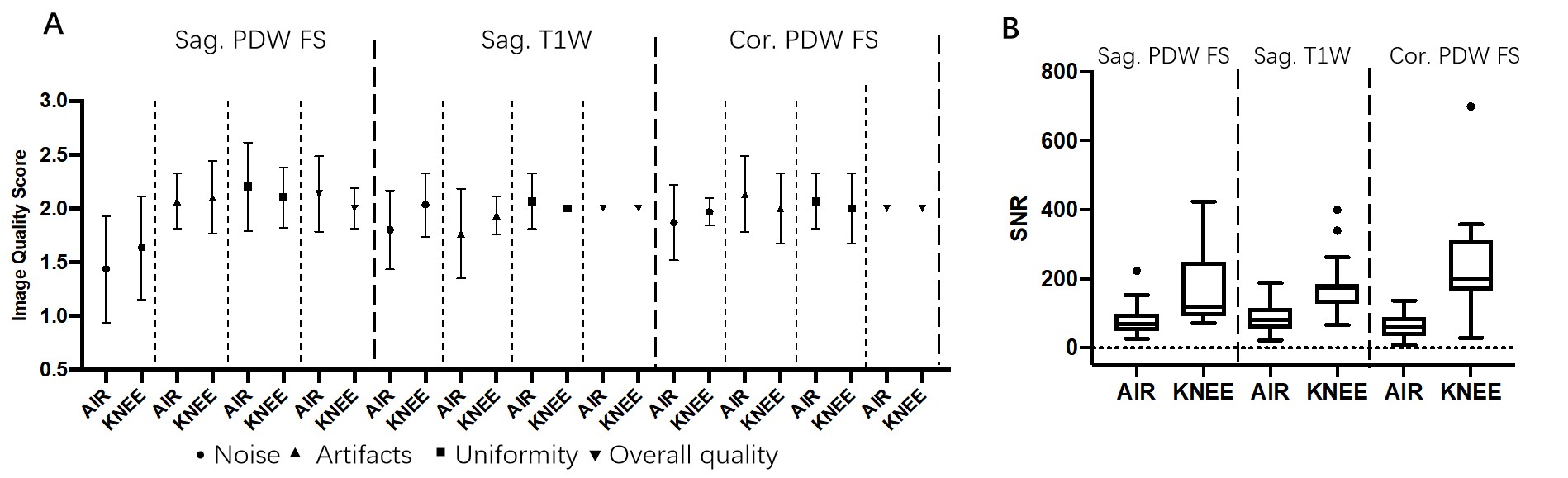
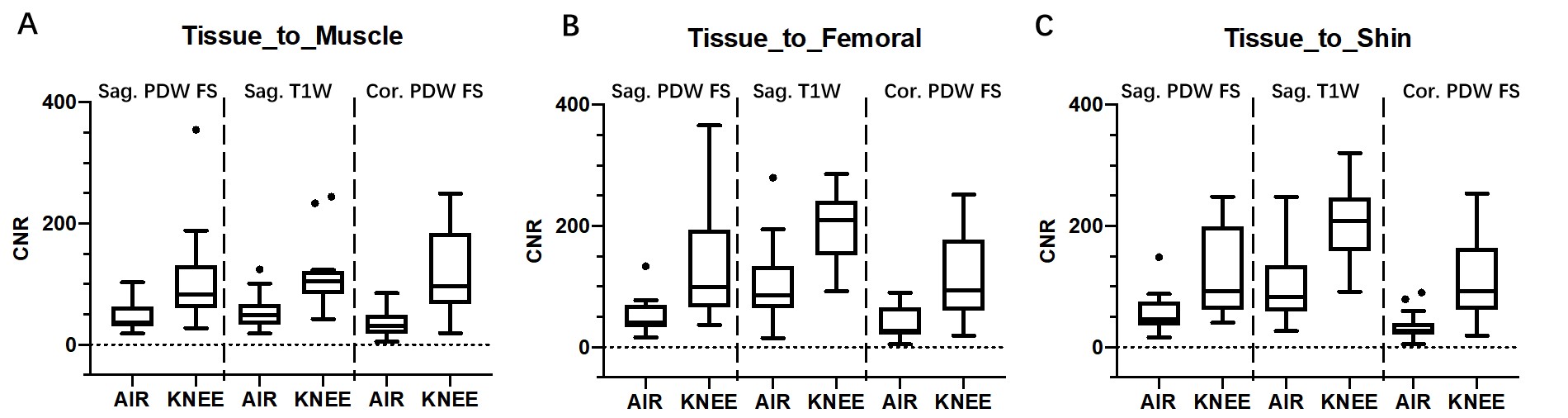
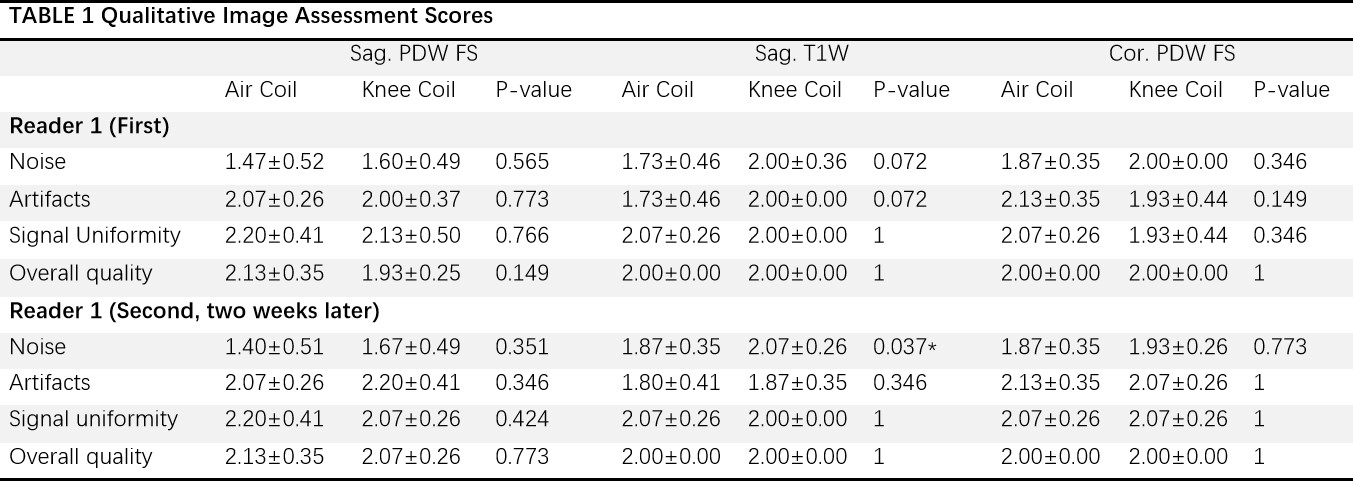
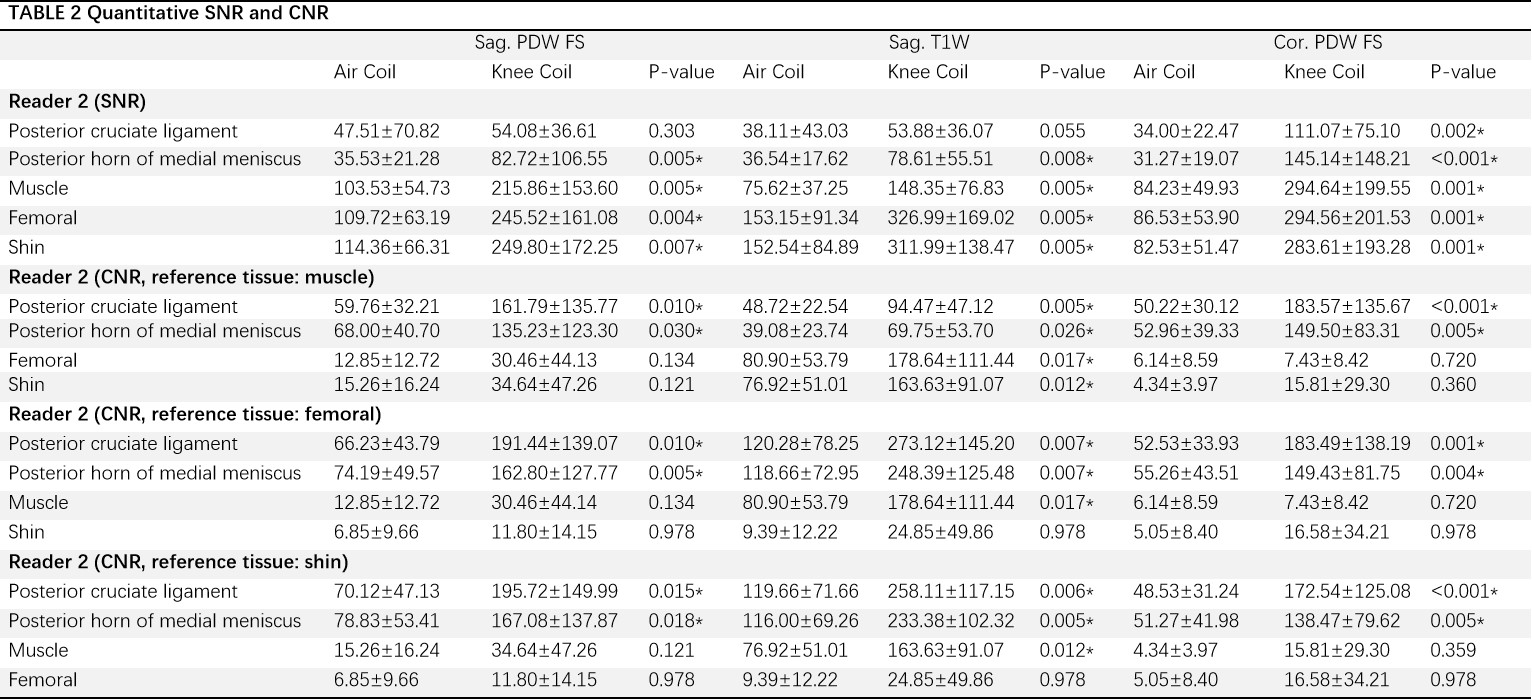
A total of 15 patients (42.5±13.4 years old, male/female: 13/2 f, 73.6±14.7 kg) were prospectively included in the study. All patients underwent knee imaging on a 3.0T MRI scanner (Signa Architect 3.0T, GE Healthcare, Milwaukee, WI) respectively with a 30-channel air body coil and a 16-channel knee coil (MAGTRON INC.) . All imaging was acquired with FOV = 160 ×160 mm, slice thickness/gap = 4/1 mm and NEX = 2. The other detailed parameters were as follows: (1) Sagittal proton density weighted with fat saturated imaging (PDW FS): TR/TE = 2093/42ms, matrix = 352 × 260, echo train length = 10, bandwidth = 41.67kHz, acquisition time = 2 min 2s ; (2) Sagittal T1 weighted imaging (T1W): TR/TE = 706/8.1 ms, matrix = 416 ×288, echo train length = 3, bandwidth = 62.5kHz, acquisition time = 1min 15s; (3) Coronal PDW FS: TR/TE = 2028/32 ms, matrix = 352 × 260, , echo train length = 10, bandwidth = 41.67kHz, acquisition time = 1min 58s. Double knees were scanned when using air coil and only one for dedicated knee coil. One radiologist (reader 1, > 5years of experience as radiologist) visually assessed the image noise, artifacts, uniformity and overall image quality on the Advantage Workstation (AW, version 4.7; GE medical system) with a 3-point scale scoring (1=worse, 2=same, 3=better) twice in a two weeks separation. Images from knee and air coils were displayed side-by-side, but the coil information was blinded. Another radiologist (reader 2, > 5years of experience as radiologist) delineated the region of interests (ROIs) in posterior cruciate ligament, posterior horn of medial meniscus, muscle, femoral, shin and background (Figure 1, A) and the ROI size is in the range of 10-20mm2 for quantitative signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) analysis. SNR was calculated with the formula Signaltissue/SDbackground. And CNR was defined as CNRtissueA-tissueB = |SignaltissueA – SignaltissueB|/SDbackground. Image visualized scores, SNR and CNR were compared with Student-t test or Mann-Whitney U test based on the data normality and homogeneity. All statistics were done in R language (ver. 4.0.0) and P < 0.05 indicated statistically significant.Results
Representative knee images of a patient were displayed in Figure 1 (A: normal size, B: large size), including the double knee image of Cor. PWD FS with air coil. In general, there were significantly lower SNR (p < 0.05) of images obtained with air coil than that of the 16-channel dedicated knee coil except the posterior cruciate ligament and posterior horn of medial meniscus for images, and in femoral and shin relative to muscle, in muscle relative to femoral and shin for T1W were found (Table2, Figure 3). Visually, no significant difference was showed for image noise, artifacts, uniformity and overall image quality between images from air coil and dedicated knee coil except the noise in Sag. T1W (Table 1).Conclusions
The SNR and CNR of images from coil were inferior to traditional knee coil for double knee imaging. The number of air coil channels is 30 and less than half was used for each knee due to the large size (66cm×79cm), therefore, much less signal could be received than the 16-channel traditional knee coil. The CNR in PDW FS images for tissue with large uniform region, such as muscle, shin and femoral and the visualized scores for noise, artifacts, uniformity and overall quality were comparable between two coils. It means that knee images from air coil were feasible for clinical observation. Air coil could be used as an alternative strategy when there is no or impaired musculoskeletal coil. Traditional coil, limited by fixed design, showed noisier and less uniform imagethan air coil for patients with larger size (Figure 1B), thus air coil is suitable at this situation, though further evaluation is necessary. For double knee imaging when required, more than half time can be saved with air coil. In future, dedicated knee air coil is till essential for better quality and flexible clinical use.Acknowledgements
No acknowledgement found.References
1. Universally Sized, High-Resolution and ASSET Optimized AIR Cervical Coils Combined with a48-Channel Head Coil for 3T MRI. ISMRM2022, ID 1606.
2. McGee KP, Stormont RS, Lindsay SA, et al. Characterization and evaluation of a flexible MRI receive coil array for radiation therapy MR treatment planning using highly decoupled RF circuits. Phys Med Biol. 2018;63(8):08NT02. Published 2018 Apr 13. doi:10.1088/1361-6560/aab691.
3. Cogswell PM, Trzasko JD, Gray EM, et al. Application of Adaptive Image Receive Coil Technology for Whole-Brain Imaging. AJR Am J Roentgenol. 2021;216(2):552-559. doi:10.2214/AJR.20.22812.
4. Bae K, Jeon KN, Hwang MJ, Jung Y, Lee J. Application of Highly Flexible Adaptive Image Receive Coil for Lung MR Imaging Using Zero TE Sequence: Comparison with Conventional Anterior Array Coil. Diagnostics (Basel). 2022;12(1):148. Published 2022 Jan 8. doi:10.3390/diagnostics12010148.
5. Comparison of Air Coil and the traditional abdomen coil for multiplexed sensitivity encoding diffusion weighted imaging (MUSE-DWI) of the liver. ISMRM 2022, ID 2134.
6. Fukui H, Onishi H, Nakamoto A, et al. Impact of adaptive image receive coil technology for liver MR imaging at 3.0 Tesla: Intraindividual comparison with use of conventional coil. Eur J Radiol. 2022;150:110271. doi:10.1016/j.ejrad.2022.110271.
Figures