1409
Rapid 3D lung imaging with bSSFP stack of spiral out-in (SoSoi) sampling at 0.55T1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, United States
Synopsis
Keywords: Lung, Lung
MRI provides radiation-free screening of many lung diseases. Its use has been limited at field strengths >1.5T, largely due to the ultra-shot T2* and low proton density in the lung. New 0.55T systems provide improved lung MRI capability since T2* is prolonged to the order of 10ms. In this work, we propose a rapid 3D bSSFP stack-of-spiral out-in (SoSoi) pulse sequence for lung imaging. The sequence can acquire 2 mm isotropic resolution image with 23 sec breathhold or 2.4 mm isotropic resolution image with 13 sec breathhold, both show great pulmonary vessels depiction.Introduction
MRI can provide screening, diagnostic assessment, and longitudinal monitoring for many lung diseases, such as cancer, emphysema, and chronic obstructive pulmonary disease, without any radiation. The use of MRI in lung has been limited at 1.5T and 3T due in large part to the ultra-short T2* which limits SNR and scan efficiency. Contemporary whole-body 0.55T MRI has demonstrated greatly improved image quality in the lung compared with 1.5T1, providing lung parenchyma T2* on the order of 10ms2. At 1.5T, a bSSFP half-radial dual-echo (bSTAR)3,4 sequence has been proposed to achieve volumetric lung imaging. bSTAR has a high SNR efficiency and uses short TR (<1.5ms), which is favorable for lung imaging where SNR is low due to low proton density and ultra-short T2*. At 0.55T, lung imaging has more flexibility due to the prolonged T2*2 and reduced B0 inhomogeneity, which allow bSSFP imaging with a longer readout and TR, providing improved SNR efficiency without compromise in image quality due to banding artifacts.In this work, we demonstrate fast volumetric bSSFP imaging using a stack-of-spiral out-in (SoSoi) trajectory and achieve isotropic 2 mm lung imaging within a single breathhold. SoSoi was compared with bSTAR implemented in Pulseq5 and a prototype product ultra-short echo 3D stack-of-spiral (UTE Spiral VIBE) sequence.
Methods
Pulse Sequence: The pulse sequence consists of a 0.08 ms non-selective “hard” pulse excitation with max flip angle 25º, a 0.43-ms kz phase encoding gradient, a 2-ms kx,ky spiral out-in readout (Figure 1(a)), and a 0.43-ms kz phase encoding rewinder. The readout duty cycle is exceptionally high at 64%. Prior to data acquisition, 21-tip ramp-up pulses followed by 59 dummy pulses were applied to drive the magnetization into steady-state. The undersampling pattern is shown in Figure 1(b), where the central 20 kz partitions is fully sampled and used to calibrate a 3D ESPIRiT kernel, and 2x undersampling in the remaining kz partitions is used in conjunction with a partial Fourier factor of 80%, making an effective undersampling factor 2.6x.Experiments: Imaging was performed on a whole-body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate)(1) and real-time interactive scanning platform (RTHawk, HeartVista)6. Five healthy adult volunteers (26-39 years, 2 female) were scanned under a protocol approved by our Institutional Review Board after providing written informed consent. Breathheld SoSoi scan parameters: flip angle=25o, FOV=48x48x24cm3, resolution=2mm isotropic, scan time=23 sec. In one subject, bSTAR (4) and a prototype UTE spiral VIBE were also acquired with the same 23 sec breathhold duration. In 3 subjects, a second slightly coarser resolution (2.4 mm isotropic) SoSoi was acquired with 10-13s scan time, where the volunteer was asked to perform extreme expiratory and inspiratory breathholds.
Reconstruction: SoSoi image was reconstructed with measured trajectories7 and an in-house implementation of 3D SPIRiT8. bSTAR was reconstructed using iterative conjugate SENSE with wavelet regularization available in the BART toolbox9 and UTE Spiral VIBE used the reconstruction available on the scanner. For SoSoi and bSTAR, the two echo images were reconstructed separately and magnitude summed.
Results
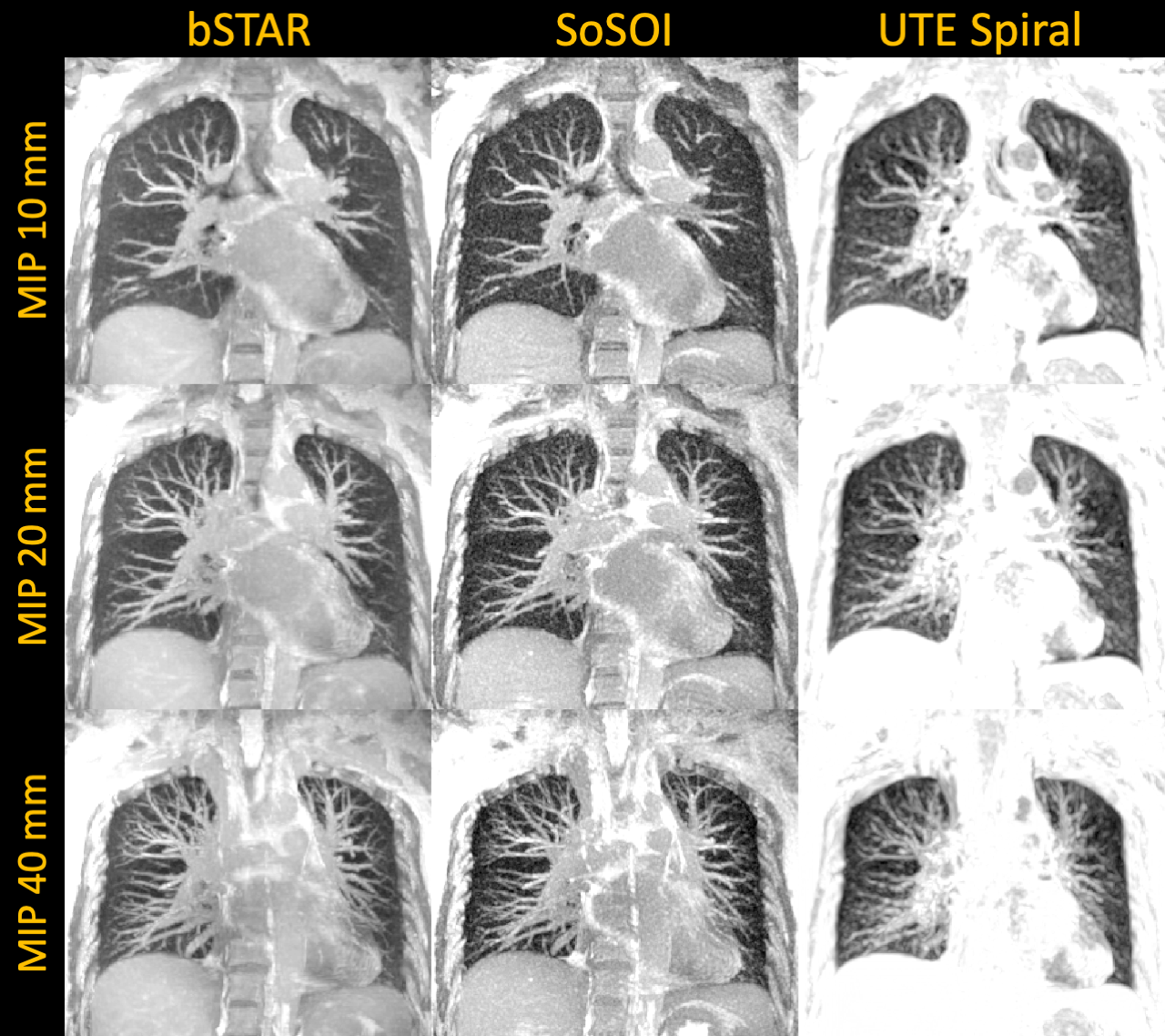
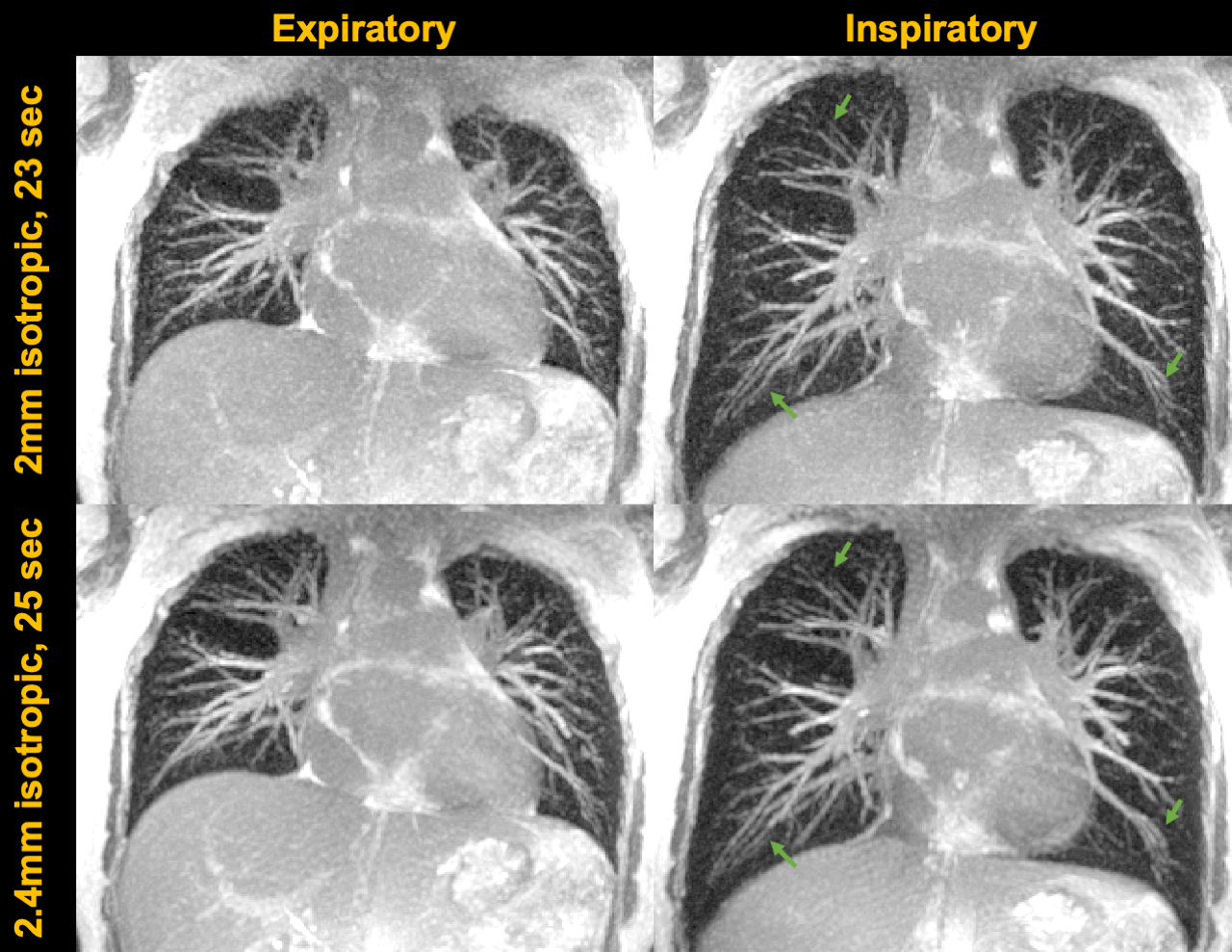
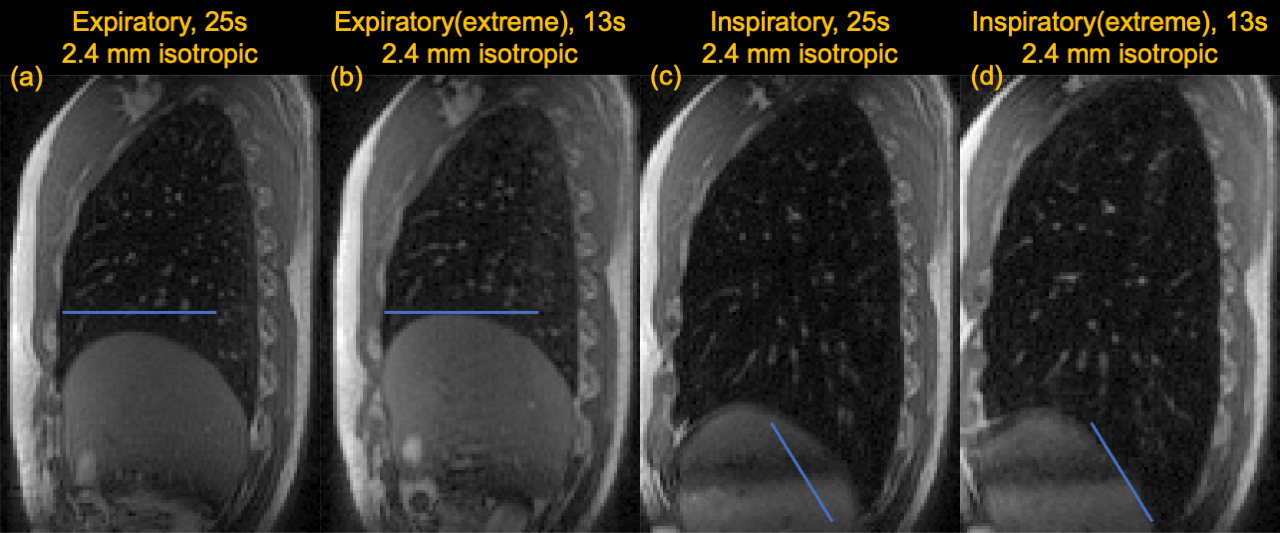
Figure 2 compares SoSoi (2mm isotropic), bSTAR (1.6mm isotropic), and Spiral UTE (2.5x2.5x2 mm3) images acquired with the same 23 sec breathhold duration. bSTAR and SoSoi resolves fine pulmonary structures such as peripheral vessels better than the UTE spiral images. Figure 3 shows maximum intensity projection (MIP) images at different thicknesses for SoSoi, bSTAR, and UTE spiral, where the pulmonary vessels are more easily appreciated. SoSoi and bSTAR again outperform UTE spiral.Figure 4 compares two versions of SoSoi images acquired with comparable breathhold duration (23-25s). Figure 5 compares the undersampled and fully sampled 2.4mm isotropic SoSoi. With undersampling the scan duration is greatly reduced (from 25s to 13s) which allows the volunteer to perform difficult breathing maneuvers such as extreme inspiration or expiration.
Discussion
We have demonstrated 3D SoSoi which can provide ultra-fast bSSFP lung imaging at 0.55T. Patients with lung conditions are usually compromised in the ability of breath holding, this fast 3D imaging may provide lung disease screening for such patient groups or allow imaging under extreme breathing maneuvers.With the spiral out-in readout, images at two echoes are acquired within a single TR, providing an opportunity for field map estimation and correction. We did not consider spatial blurring caused by off-resonance or concomitant fields and this remains future work10,11.
This work used a stack-of-spiral out-in trajectory and used a 3D SPIRiT reconstruction. It is possible to extend it into 3D spiral projection out-in to achieve an even higher duty cycle12. Since 3D spiral projection encodes the entire volume, the kz phase encoding gradients can be avoided and investigating the trade-offs are of interest for future works. We also observed that the SoSoi images are slightly noisier than bSTAR images, which could be attributed to the additional use of wavelet regularization in the bSTAR reconstruction pipeline. The combination of 3D SPIRiT with image-domain regularizations for SoSoi may further improve its apparent SNR.
Conclusion
We have demonstrated efficient 3D lung imaging at 0.55T based on dual-echo bSSFP with a SoSoi trajectory. This approach provides volumetric 2mm isotropic resolution and 2.4mm isotropic resolution under a 23s and 13s breathhold, respectively.Acknowledgements
We acknowledge grant support from NSF Grant #1828736 and research support from Siemens Healthineers.References
1. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-93.
2. Li B, Lee NG, Cui SX, Nayak KS. Lung parenchyma transverse relaxation rates at 0.55 Tesla. Magnetic Resonance in Medicine2022.
3. Bieri O, Pusterla O, Bauman G. Free-breathing half-radial dual-echo balanced steady-state free precession thoracic imaging with wobbling Archimedean spiral pole trajectories. Z Med Phys. 2022.
4. Bauman G, Bieri O. Balanced steady-state free precession thoracic imaging with half-radial dual-echo readout on smoothly interleaved archimedean spirals. Magn Reson Med. 2020;84(1):237-46.
5. Layton KJ, Kroboth S, Jia F, Littin S, Yu H, Leupold J, et al. Pulseq: A rapid and hardware-independent pulse sequence prototyping framework. Magn Reson Med. 2017;77(4):1544-52.
6. Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med Biol Soc. 2004;2004:1048-51.
7. Duyn JH, Yang Y, Frank JA, van der Veen JW. Simple correction method for k-space trajectory deviations in MRI. J Magn Reson. 1998;132(1):150-3.
8. Lustig M, Pauly JM. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn Reson Med. 2010;64(2):457-71.
9. BART Toolbox for Computational Magnetic Resonance Imaging.
10. Javed A, Ramasawmy R, O'Brien K, Mancini C, Su P, Majeed W, et al. Self-gated 3D stack-of-spirals UTE pulmonary imaging at 0.55T. Magn Reson Med. 2022;87(4):1784-98.
11. Lee NG, Ramasawmy R, Lim Y, Campbell-Washburn AE, Nayak KS. MaxGIRF: Image reconstruction incorporating concomitant field and gradient impulse response function effects. Magn Reson Med. 2022.
12. Cao X, Liao C, Iyer SS, Wang Z, Zhou Z, Dai E, et al. Optimized multi-axis spiral projection MR fingerprinting with subspace reconstruction for rapid whole-brain high-isotropic-resolution quantitative imaging. Magn Reson Med. 2022;88(1):133-50.
Figures