1402
Improved 129Xe MRI of cardiopulmonary oscillations in patients with chronic thromboembolic pulmonary hypertension1Medical Physics, Duke University, Durham, NC, United States, 2Biomedical Engineering, Duke University, Durham, NC, United States, 3Radiology, Duke University, Durham, NC, United States, 4Cardiology, Duke University, Durham, NC, United States, 5Clinical Imaging Physics Group, Duke University, Durham, NC, United States, 6Pulmonary, Critical Care, and Sleep Medicine, University of Kansas Medical Center, Kansas City, KS, United States
Synopsis
Keywords: Lung, Hyperpolarized MR (Gas), CTEPH, keyhole reconstruction
Dynamic spectroscopy of hyperpolarized 129Xe in red blood cells exhibits cardiopulmonary oscillations that can be used to detect both pre- and post-capillary pulmonary hypertension (PH). However, this whole-lung measurement cannot resolve spatially heterogeneous variations in oscillations. This limitation can be addressed by using keyhole reconstruction approaches to spatially resolve the oscillations. Here we demonstrate several extensions of this technique that make both the reconstruction and analysis more robust. We have used this to establish updated healthy reference distributions and demonstrate the utility of spatially resolved mapping in a cohort of patients with chronic thromboembolic pulmonary hypertension pre- and post-thromboendarterectomy.
Introduction
The interaction of 129Xe atoms with red blood cells (RBCs) provides a unique means to characterize various cardiopulmonary diseases1,2. Specifically, this signal exhibits cardiogenic oscillations capable of determining whether pulmonary hypertension (PH) is pre- or post-capillary in nature3. Such non-invasive detection of PH is particularly valuable given that the standard right heart catheterization (RHC) test is invasive and associated with some degree of morbidity and mortality4. However, current measurements using whole-lung spectroscopy are unable to discern spatial heterogeneity, which limits its diagnostic potential in certain conditions such as combined pre- and post-capillary pulmonary hypertension (CPcPH)5.An alternative approach is to exploit the cardiogenic oscillations detectable at the center of k-space in 129Xe gas exchange MRI by using keyhole reconstruction to map their spatial variation6,7. Here we demonstrate several technical improvements to this reconstruction approach and use them to establish more refined healthy reference distributions for image binning and visualization. We then demonstrate the benefits of such spatial resolution to detect regions of both low and high RBC amplitude oscillations in patients with chronic thromboembolic pulmonary hypertension (CTEPH)8 and show surgical response after pulmonary thromboendarterectomy (PTE) surgery.
Methods
All subjects underwent 129Xe gas exchange MRI according to established protocols9. Healthy subjects (11 male, 6 female ages 18-30) with no smoking history or known respiratory or cardiac conditions were used to establish reference distributions. Subsequently 10 subjects with CTEPH (6 male, 4 female with mean age 52±17) were enrolled for baseline MRI and 6 returned for imaging 1-6 months after PTE surgery to remove the chronic clots in the lung vasculature. For the CTEPH cohort, RHC was performed within 5 months of 129Xe MRI and was used to determine PH status (8 pre-capillary PH, 2 CPcPH) according to Simonneau et al.10.
RBC oscillation images were processed using the approach of Niedbalski et al.6 with several notable updates: 1) binning of radial views to the high and low keys was achieved using peak finding on the filtered RBC signal 2) reconstruction key radius was constrained to a value of 9 out of 128 in the radial spoke to eliminate artifacts and 3) oscillation amplitude $$$O_v$$$ was calculated on a voxel-by-voxel basis according to:
$$O_v = \frac{HighKey_v-LowKey_v}{Nonkeyhole_v} x 100%$$
These methods were used to build an updated cumulative reference distribution of oscillations from the healthy subject cohort. This distribution underwent Box Cox transformation to calculate the mean and standard deviation (SD) and establish image binning thresholds in one SD intervals. The thresholds were then inverse transformed and used for binning of regional cardiogenic oscillations amplitudes11,12.
The RBC oscillation amplitude maps were quantified using the mean oscillation percent and combined percentage of lung voxels classified as defect or low. These metrics were compared between the CTEPH and healthy cohorts (Mann-Whitney U-test) as well as for the CTEPH patients pre-and post-surgery (paired Wilcoxon tests).
Results
Figure 1 shows the combined distribution of RBC oscillation amplitudes and thresholds for the healthy cohort after Box Cox transformation. Compared to the published distribution6, the mean value increased from 9.8% to 10.6% while the standard deviation decreased from 9.0% to 8.2%. Application of these bins to generate oscillation amplitude maps are shown for a healthy subject.Figure 2 shows RBC oscillation amplitude maps from a CTEPH patient before and after PTE surgery. This patient exhibited a large percentage of voxels with oscillations in the defect and low bins (19% vs 7.4±7.5% reference) as well as in the high bins (7.5% vs 3.9±4.2% reference). After PTE, their combined defect and low percentage decreased to 2%, while high percentage increased to 14%, suggesting persistent microvasculopathy despite near-complete reversal of the pre-capillary PH. Figure 3 shows a second example of a CTEPH patient at baseline and 1 month after surgery. For this patient the resected thrombi were noted to have come from the right lung, which is where oscillation defects were most prominent.
In aggregate, subjects with CTEPH at baseline (Figure 4 top) exhibited lower mean oscillation amplitudes, (4.8±2.9%) than healthy volunteers (11.2±3.4%, p < .001) and a higher percentage of voxels in defect+low (25.3±9.3% vs 11.2±3.4%, p < .001). In CTEPH subjects who underwent PTE mean oscillation amplitudes increased from 4.0±3.5% to 7.5±5.2% (p = 0.04). All but one subject post-PTE exhibited a decrease in defect+low oscillations amplitudes (from 26.5±11.3% to 16.8±8.2%, p = 0.09).
Discussion
RBC oscillation imaging using keyhole reconstruction is sensitive to the choice of radial projection binning, keyhole radius, and voxel intensity calculation. This work builds on the published approach by implementing several processing changes that improve robustness of keyhole reconstruction. Applying these updated methods to a well-curated healthy cohort yielded a narrower healthy reference distribution, which we expect to provide greater sensitivity to changes in oscillation amplitude.Applying this approach to CTEPH subjects permitted visualization of low and absent oscillations distal to chronic thrombi. The technique could visualize improvement in these oscillations after PTE, suggesting a positive surgical response. Spatial information introduced by keyhole oscillation imaging has the potential to address current limitations of whole-lung dynamic spectroscopy in its evaluation of complex and heterogeneous hemodynamics.
Acknowledgements
Funding sources: R01HL105643, R01HL12677, NSF GRFP DGE-1644868, AHA CDA 930177References
1. Weatherley, N.D., et al. Hyperpolarised xenon magnetic resonance spectroscopy for the longitudinal assessment of changes in gas diffusion in IPF. Thorax 74, 500-502 (2019).
2. Wang, Z., et al. Diverse cardiopulmonary diseases are associated with distinct xenon magnetic resonance imaging signatures. Eur Respir J 54(2019).
3. Bier, E. Noninvasive Diagnosis of Pulmonary Hypertension with Hyperpolarized 129Xe Magnetic Resonance Imaging and Spectroscopy. in ISMRM (2021).
4. Hoeper, M.M., et al. Complications of right heart catheterization procedures in patients with pulmonary hypertension in experienced centers. J Am Coll Cardiol 48, 2546-2552 (2006).
5. Ibe, T., et al. Combined pre- and post-capillary pulmonary hypertension: The clinical implications for patients with heart failure. PLoS One 16, e0247987 (2021).
6. Niedbalski, P.J., et al. Mapping cardiopulmonary dynamics within the microvasculature of the lungs using dissolved (129)Xe MRI. J Appl Physiol (1985) 129, 218-229 (2020).
7. Bier, E.A., et al. Extension of a Diagnostic Model for Pulmonary Hypertension with Hyperpolarized 129Xe Magnetic Resonance Imaging and Spectroscopy. in ISMRM 2021 (2021).
8. Madani, M.M. Surgical Treatment of Chronic Thromboembolic Pulmonary Hypertension: Pulmonary Thromboendarterectomy. Methodist Debakey Cardiovasc J 12, 213-218 (2016).
9. Niedbalski, P.J., et al. Protocols for multi-site trials using hyperpolarized (129) Xe MRI for imaging of ventilation, alveolar-airspace size, and gas exchange: A position paper from the (129) Xe MRI clinical trials consortium. Magn Reson Med 86, 2966-2986 (2021).
10. Simonneau, G., et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 53(2019).
11. Sakia, R.M. The Box-Cox Transformation Technique: A Review. Journal of the Royal Statistical Society. Series D (The Statistician) 41, 169-178 (1992).
12. Wang, Z., et al. Quantitative analysis of hyperpolarized (129) Xe gas transfer MRI. Med Phys 44, 2415-2428 (2017).
13. Bier, E.A., et al. Noninvasive diagnosis of pulmonary hypertension with hyperpolarised (129)Xe magnetic resonance imaging and spectroscopy. ERJ Open Res 8(2022).
Figures
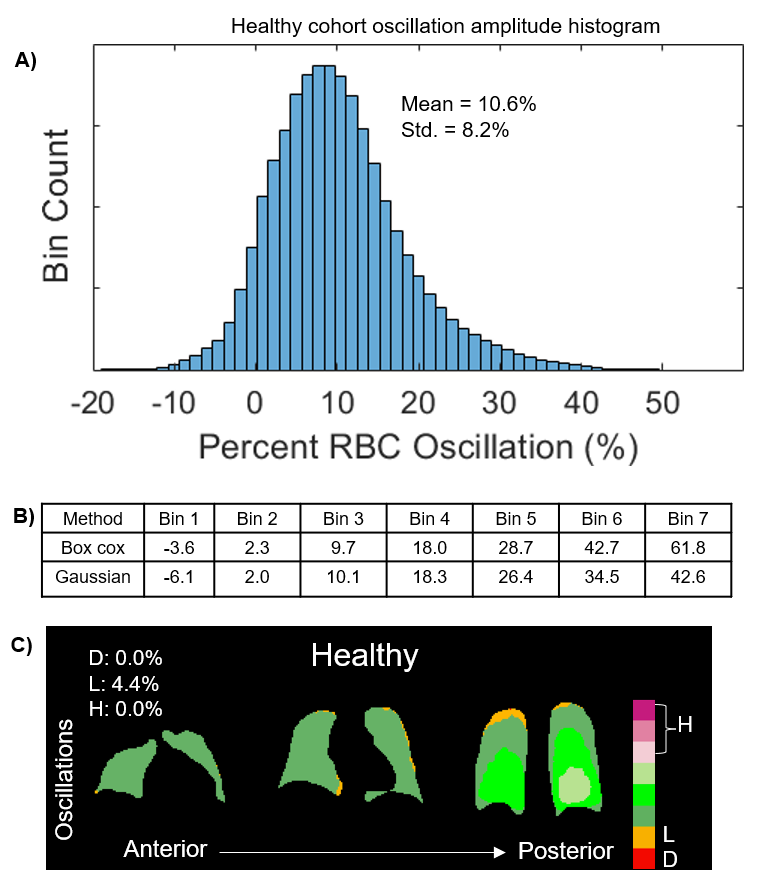
Figure 1. A) Cumulative reference distribution from 17 healthy, young subjects (ages 18-30). Notably, its standard deviation is narrower (8.2%) than the previously reported value (9.0%). B) An 8-bin set of thresholds were determined by calculating the mean and standard deviation after undergoing a Box Cox transformation. C) Representative binned oscillation maps of a healthy subject using the refined thresholds.
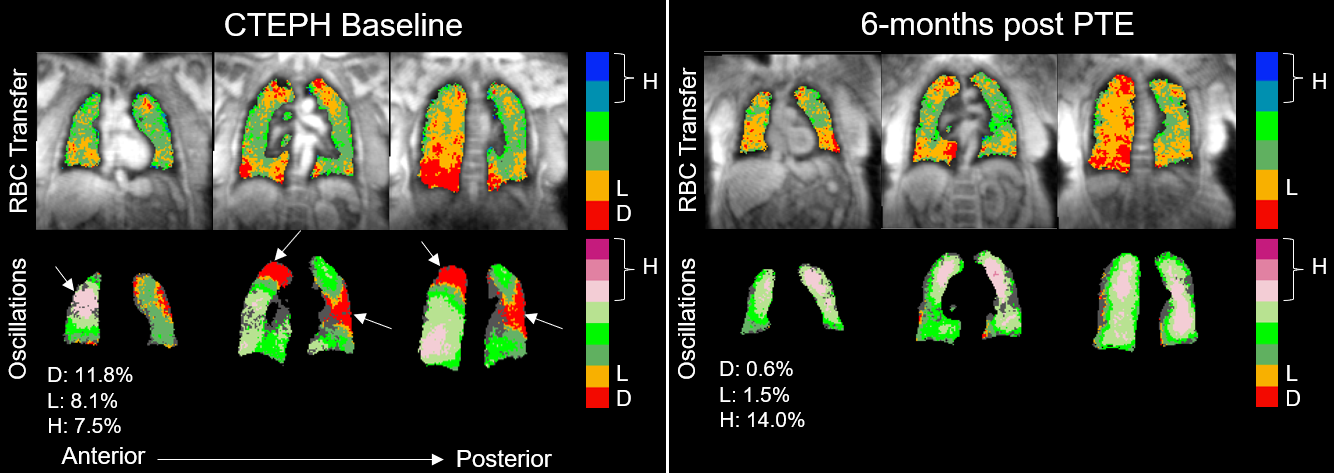
Figure 2. 129Xe MRI and RBC oscillation imaging for a representative subject with CTEPH and no extensive obstructive or interstitial disease. Conventional whole-lung dynamic spectroscopy showing a 10.9% oscillation amplitude would falsely classify this subject as having no PH13. However, spatially resolving the oscillations appears to correctly indicate the presence of both decreased perfusion (areas of decreased oscillations) and microvasculopathy (loss of RBC transfer) at baseline and an improvement in perfusion post-PTE.
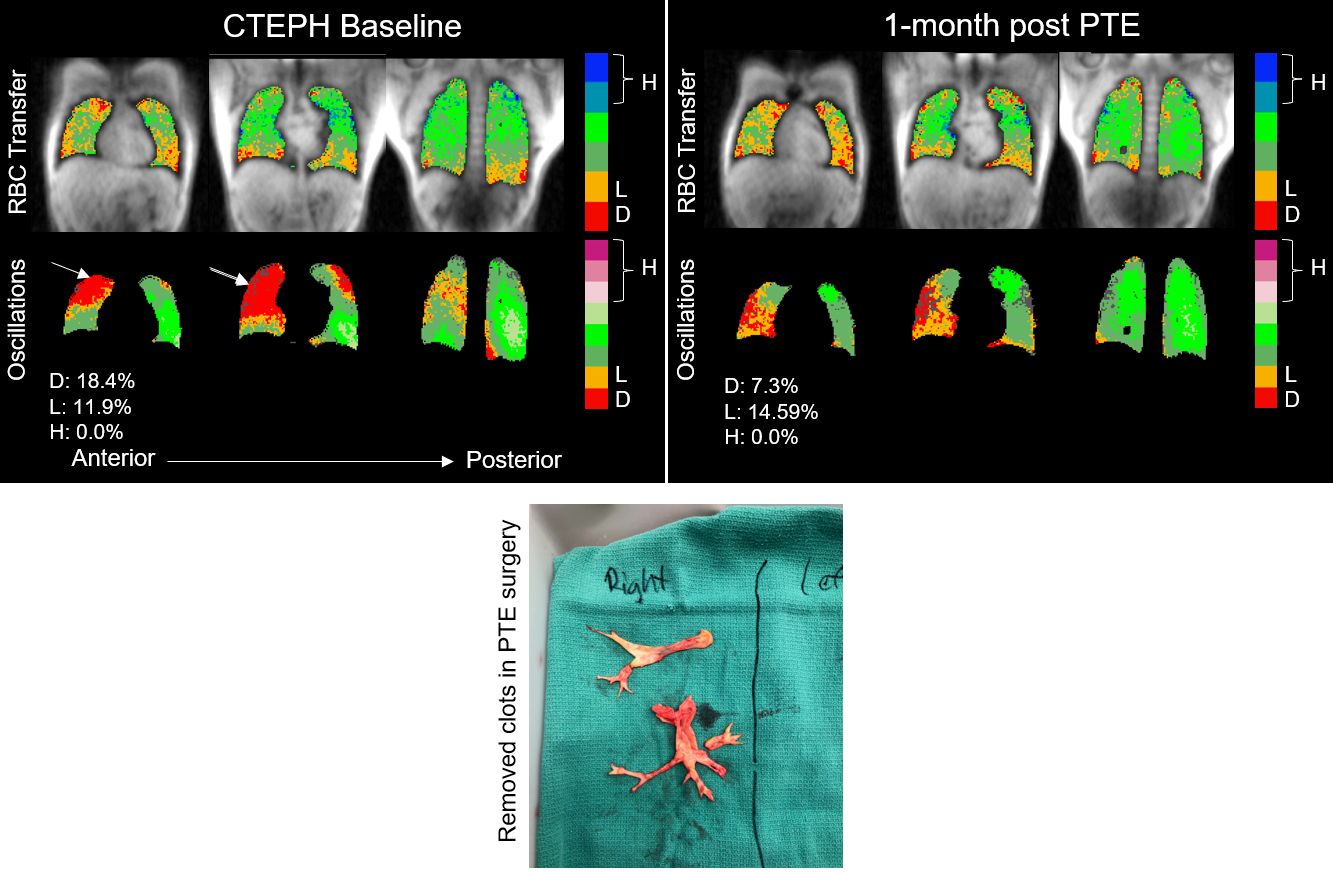
Figure 3. 129Xe MRI and RBC oscillation imaging for a representative subject with CTEPH and the location of the blood clots removed during PTE (arrows). Here, the blood clots were in the right lung, suggesting a region of high pulmonary vascular resistance. The RBC oscillation defects matched this spatial pattern and were later normalized in the region post-PTE.
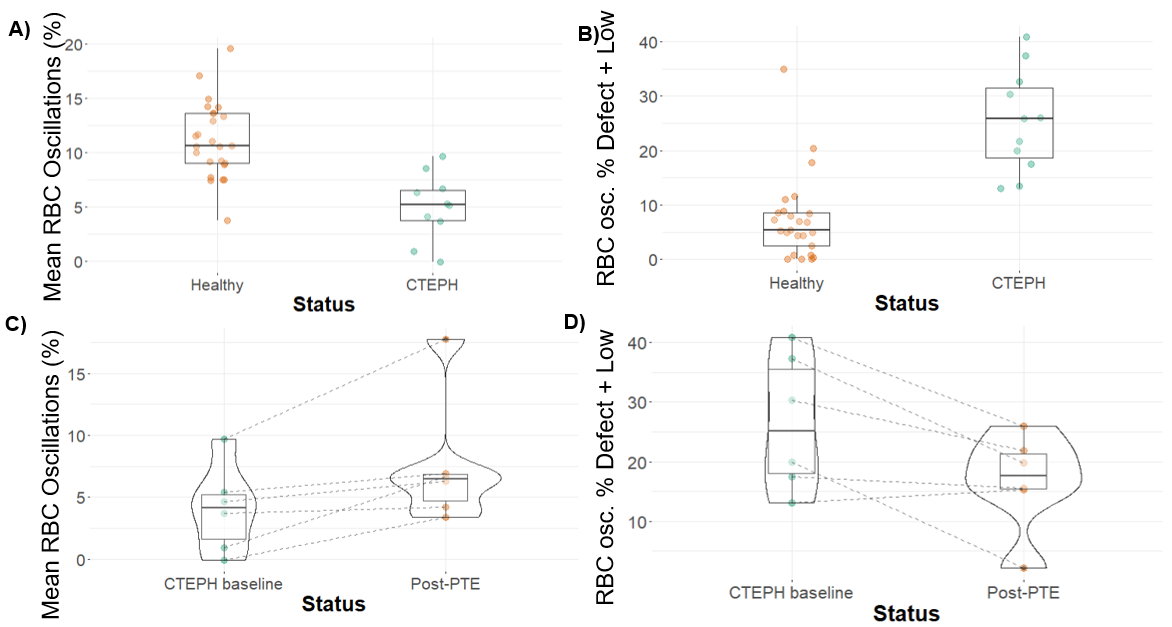
Figure 4. Comparisons of metrics obtained from oscillation maps. Comparing healthy subjects vs CTEPH (A) mean oscillation amplitudes and (B) percentage of voxels binned as defect and low both differentiate healthy and subjects with CTEPH (p<.001). For CTEPH subjects who underwent PTE (C) mean oscillation amplitude increased significantly (p=0.04), and (D) percentage of defect+low voxels decreased in all but one patient.