1352
Real-time Multi-Contrast 4D MRI using Motion Transfer for Low-Latency Volumetric Motion Tracking on a 1.5T MR-Linac System1Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 3Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: Multi-Contrast, Cancer
Real-time multi-contrast 4D MRI is proposed by transferring motion from 4D T1-weighted images to 3D T2-weighted images and performing fast signature matching based on T1-weighted 3D radial stack-of-stars acquisitions. The proposed approach exploits the anatomical correlations between T1-weighted and T2-weighted images and fast acquisition of T1-weighted data to generate real-time multi-contrast volumetric motion information for adaptation and monitoring of radiation treatment of tumors affected by respiratory motion on an MR-Linac system. The feasibility of the proposed method was demonstrated on patients with pancreatic cancer.INTRODUCTION
Real-time 4D MRI would enable free-breathing treatment adaptation and dose accumulation calculation for tumors affected by respiratory motion on an MR-Linac system. MR signature matching (MRSIGMA) is a recently developed real-time 4D MRI technique with an imaging latency below 300 ms [1, 2], which has shown great potential to image motion of tumors and organs-at-risk (OARs) on an Elekta Unity MR-Linac system [3]. MRSIGMA uses a T1-weighted (T1W) golden-angle stack-of-stars radial acquisition to generate the 4D dictionary and perform fast signature matching. T2-weighted (T2W) contrast provides complementary information that is essential for accurate contouring of the tumor and OARs due to higher fluid sensitivity compared to T1W images. However, T2W imaging requires a significantly longer echo time, which makes it inefficient to perform MRSIGMA. This work presents a motion transfer technique to generate motion-resolved 4D T2W images using static 3D T2W images and motion information from T1W MRSIGMA data for real-time multi-contrast 4D MRI on a 1.5T MR-Linac system.METHODS
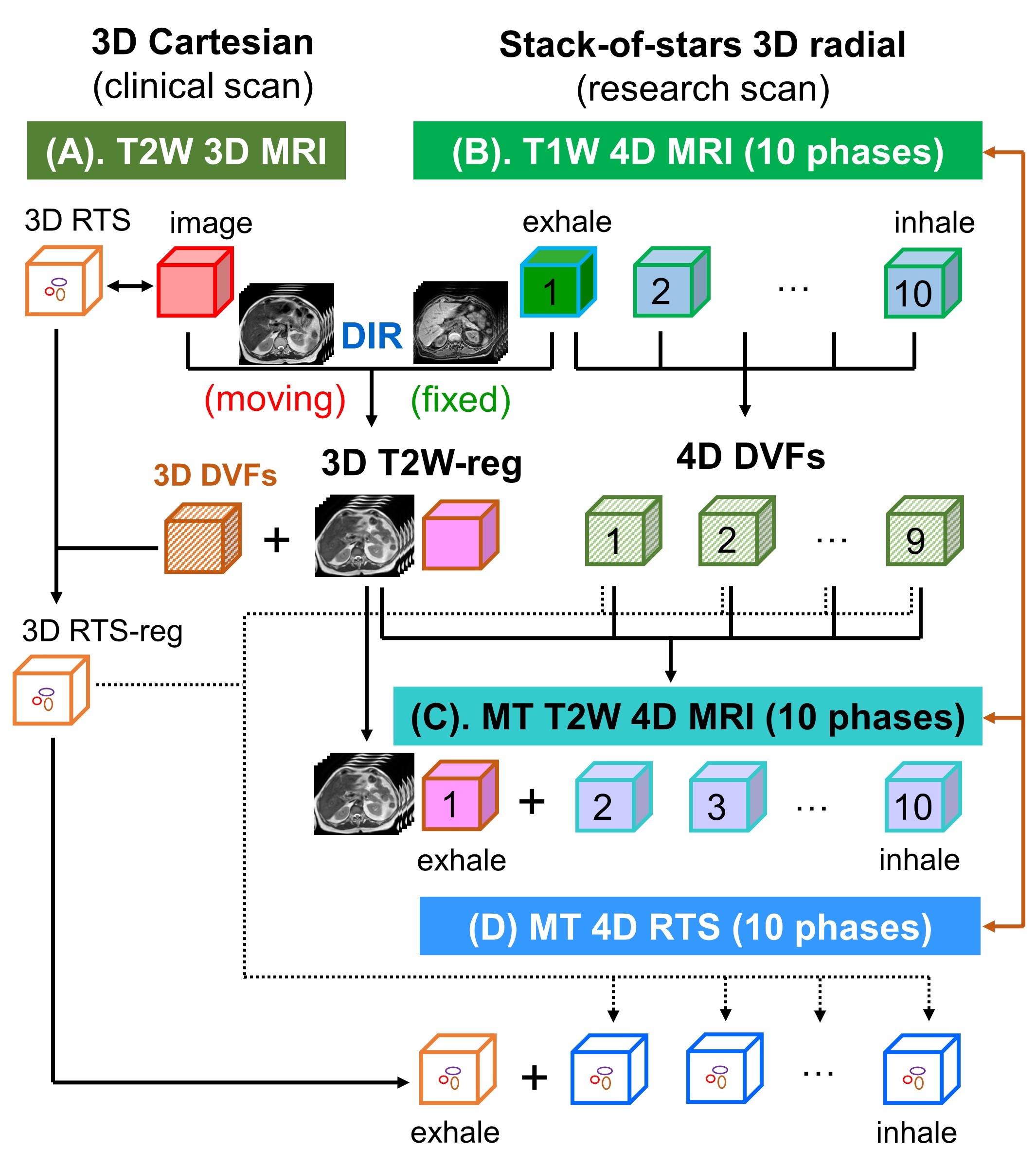
T2W 3D MRI and T1W 4D MRI: T2W 3D MRI was acquired using the routine sequence for pancreatic cancer treatment on a 1.5T MR-Linac system (Elekta AB, Stockholm, Sweden) with the following parameters: TR/TE = 1300/87 ms, voxel size = 1.1×1.1×2.0 mm3, and scan time = 3:41 min. Clinical contours of the gross tumor volume (GTV) and OARs were adjusted on T2W and T1W 3D MRI images by radiation therapists and physicians to enable treatment adaptation to daily changes in anatomical positions and shapes. In addition, a research scan was performed after clinical treatment using 3D T1W golden-angle stack-of-stars radial sampling with the following parameters: TR/TE = 5.0/2.1 ms, voxel size =1.5 ×1.5×4.0 mm3, flip angle = 12°, and scan time = 5:35 min. XD-GRASP [4] reconstruction was performed to generate 4D T1W images with 10 respiratory phases. Three patients with pancreatic cancer were included in the study.Multi-contrast 4D MRI: Figure 1 illustrates the concept of multi-contrast 4D MRI using motion transfer. First, clinical T2W 3D MRI is registered to the first phase (end-expiration) of T1W 4D MRI using deformable image registration (DIR) in Plastimatch [5], which produces the registered T2W 3D MRI (3D T2W-reg) and corresponding 3D deformation vector fields (3D DVFs). Second, the 3D radiotherapy structures (RTS) associated with clinical T2W 3D MRI are deformed using the 3D DVFs to obtain the registered 3D RTS (3D RTS-reg). Third, 3D T2W-reg are deformed by the 4D DVFs from T1W 4D MRI to generate the motion-transferred (MT) T2W 4D MRI. Finally, 3D RTS-reg are deformed using the same 4D DVFs to generate the MT 4D RTS, which are co-registered with T1W and T2W 4D MRI.
Real-time motion tracking: The training dictionary includes T1W 4D MRI, MT T2W 4D MRI, and MT 4D RTS, which are spatially and temporally co-registered. The motion signatures are based on the T1W images. Real-time imaging is performed by signature matching of each real-time T1W point (radial angle) to one of the T1W motion signatures and its corresponding multi-contrast motion states and associated RTS in the training dictionary.
RESULTS
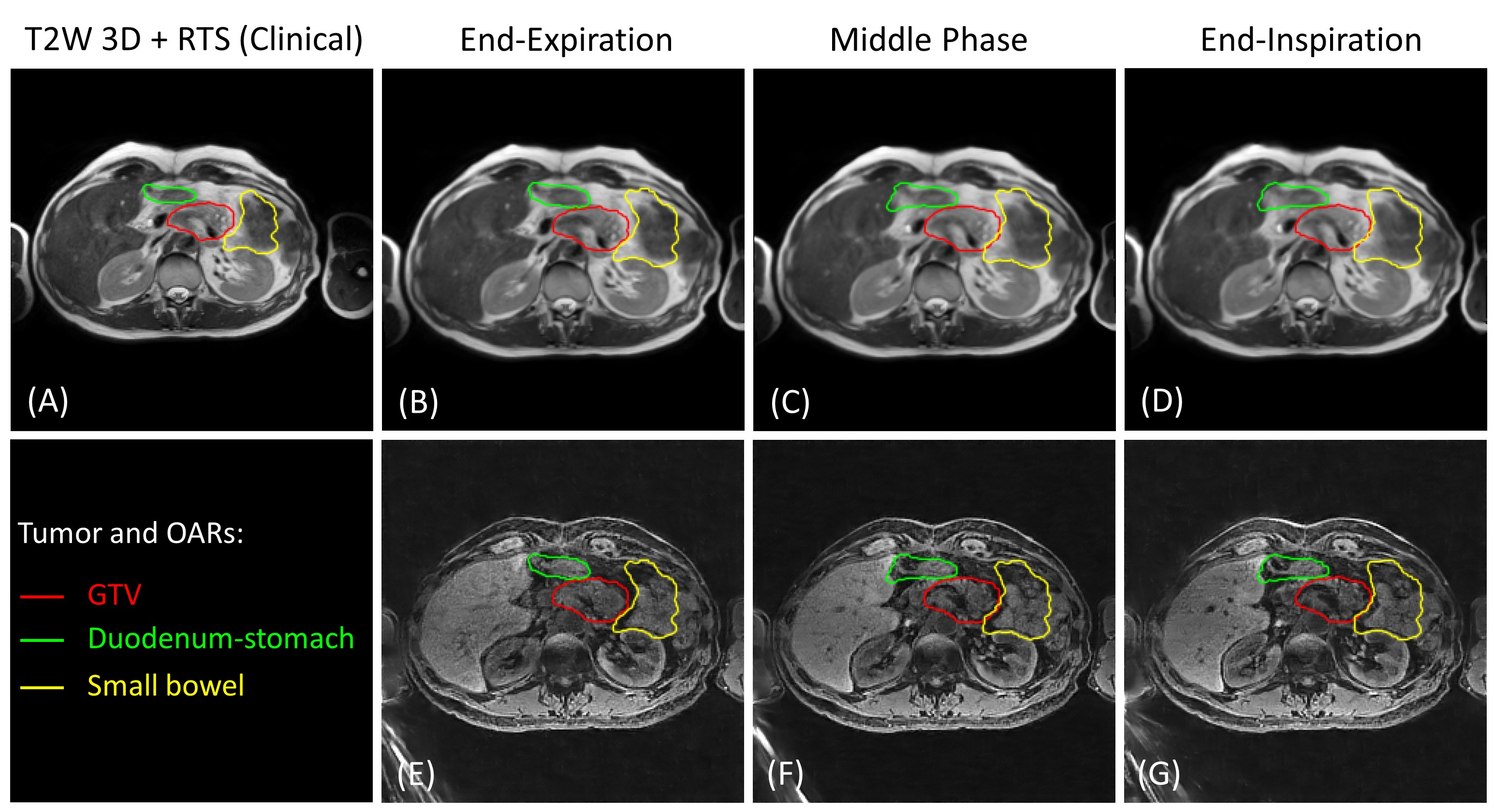
Figure 2 (GIF video) shows the clinical T2W 3D MRI, T1W 4D MRI, and MT T2W 4D MRI from a 62-year-old patient. The clinical T2W 3D images were successfully registered to the first respiratory phase of the T1W 4D MRI images and the motion from T1W 4D MRI was transferred to generate the MT T2W 4D MRI. Figure 3 (GIF video) shows another example from a 72-year-old patient. Figure 4 shows the overlay of the RTS (GTV, duodenum-stomach, and small bowel) on clinical T2W 3D MRI and three respiratory phases (end-expiration, middle phase, and end-inspiration) of the T1W 4D MRI and MT T2W 4D MRI images from a 63-year-old patient. Figure 5 (GIF video) presents real-time multi-contrast 4D MRI and associated 4D RTS in 50 consecutive time points for volumetric motion tracking. Signature matching latency was lower than 300ms, including acquisition time for one radial angle (~250ms) and matching (~30ms).DISCUSSION
Clinical T2W 3D MRI is routinely acquired for treatment adaptation at each fraction. Therefore, no additional scan time is needed to generate the MT T2W 4D MRI with motion transfer from T1W 4D MRI. Similarly, the 3D RTS can be deformed to generate the MT 4D RTS, which can be used for real-time volumetric motion tracking without needing additional work from radiation therapists and physicians. Since signature acquisition and matching are based solely on T1W images, there is no overhead for the inclusion of T2W images in the real-time section and the same latency from the original MRSIGMA implementation is preserved. Moreover, motion information from T1W 4D MRI can be similarly transferred to other image contrasts, such as T2/T1 image contrast from bSSFP or diffusion-weighted image contrast. In addition, the process of deformable image registration (~5 min) can be significantly accelerated using a deep-learning based registration approach.CONCLUSION
This work demonstrates the feasibility of real-time multi-contrast 4D MRI using motion transfer for low-latency volumetric motion tracking on a 1.5T MR-Linac. Real-time multi-contrast 4D MRI can be useful to improve adaptation and to calculate dose accumulations in tumors affected by respiratory motion.Acknowledgements
The work was supported by NIH Grant R01CA255661.References
1. Feng L, Tyagi N, Otazo R. MRSIGMA: Magnetic Resonance SIGnature MAtching for real-time volumetric imaging. Magn Reson Med 2020; 84(3):1280-1292.
2. Kim N, Tringale KR, Crane C, Tyagi N, Otazo R. MR SIGnature MAtching (MRSIGMA) with retrospective self-evaluation for real-time volumetric motion imaging. Phys Med Biol 2021; 66(21):215009.
3. Wu C, Tyagi N, Reyngold M, Crane C, Otazo R. Real-time 3D MRI for low-latency volumetric motion tracking on a 1.5T MR-Linac system. Proc Intl Soc Mag Reson Med 2022; 30:0230.
4. Feng L, Axel L, Chandarana H, et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med 2016;75(2):775-788.
5. www.plastimatch.org
Figures