1322
Relaxation-Enhanced Angiography without Contrast and Triggering (REACT) for evaluation of iliac vein compression syndrome at 3T1The First Affiliated Hospital of Chongqing Medical University, Chongqing, China, 2Clinical Science, Philips Healthcare, Chengdu, China
Synopsis
Keywords: Vessels, Blood vessels
Relaxation-Enhanced Angiography without Contrast and Triggering (REACT) is a novel flow-independent MR angiography technique without cardiac triggering, breath holding and contrast agent injection and has promising results to show robust blood-to-tissue contrast over multiple anatomies. This study aims to investigate the feasibility of REACT for evaluation iliac vein compression syndrome in comparison with catheter angiography. Results showed that with comparable image quality to catheter angiography and high sensitivity and specificity for the detection of stenosis, REACT was proven to be a clinically applicable method for assessing iliac vein compression syndrome.Introduction
The central venous stenosis (CVS) of end-stage renal disease is a common complication of hemodialysis[1] and the gold standard for CVS imaging is catheter angiography, which is invasive. Contrast enhanced MR evaluation of the central veins has been reported to be extremely sensitive and specific in the detection of stenoses and occlusions[2]. But the gadolinium-based contrast agents as a causative factor may introduce nephrogenic systemic fibrosis, especially for ESRD patients. In recent years, MR venography with the blood pool specific agent acquired better image quality and can eliminate the risk of NSF, but the price is high. Relaxation-Enhanced Angiography without Contrast and Triggering (REACT) is a MRA technique without contrast and has been evaluated in pelvic venous vessels and pulmonary vasculature[3,4]. However, the evaluation of REACT in central venous stenosis has not been reported yet. Therefore, this study aims to assess the feasibility and diagnostic accuracy of REACT in the evaluation of central thoracic venous occlusive disease and compare it with CE-MRA and catheter angiography.Materials and Methods
This study was approved by our Institutional Review Board and obtained informed consent. The MR examinations were conducted on a clinical 3.0T MR system using ng a 32-channel coil array (Ingenia 3.0T, Philips Healthcare, the Netherlands). 126 consecutive patients (61 women and 65 men; age range, 14-85 years; mean age, 57 years ± 12 [SD]) with iliac vein compression symptoms, such as lower limb varicose veins, skin pigmentation, ulceration and others, has prospectively enrolled and had undergone REACT MR examinations in this study. The scan parameters of REACT were listed as follows: FOV=500 mm× 420 mm, acquired voxel size=1.4 mm× 1.4 mm× 3.0 mm, reconstructed voxel size=0.65 mm× 0.65 mm× 1.50 mm, T2-prep time = 50 ms, Inversion delay time=100 ms, TR/TE1/ TE2= 3.70/1.31/2.40ms, Flip angle 12°, TFE shot duration is 395 ms, TFE shot interval is 3000 ms, NSA = 3 time, scanning time is 4 minutes and 33 seconds. Catheter angiography was performed for all patients within 1 week after REACT MR examination. The images were evaluated in separate reading sessions by two independent radiologists for the rate and type of iliac vein stenosis using the following grading scale: 100-(100×D1/D2) where D1 is the minimum diameter at the point of maximum compression and D2 is the minimum diameter at the common iliac vein (CIV) caudal to the obstruction [1]. The accuracy of REACT was assessed with catheter angiography as the standard of reference. The data were performed by Mann-Whitney test between two groups.Results
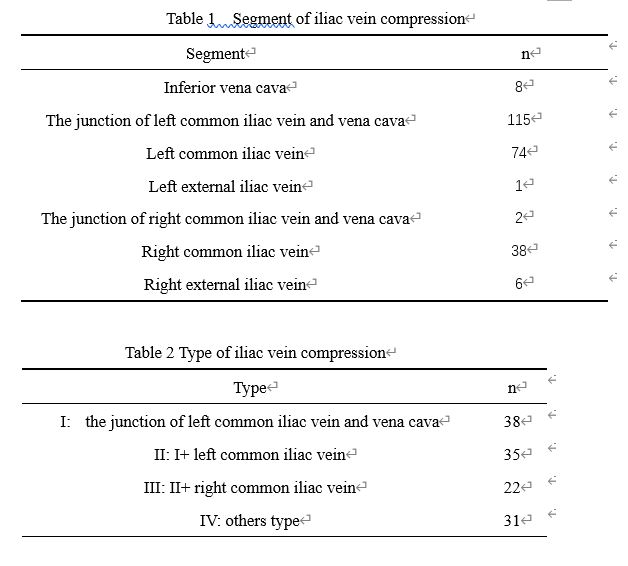
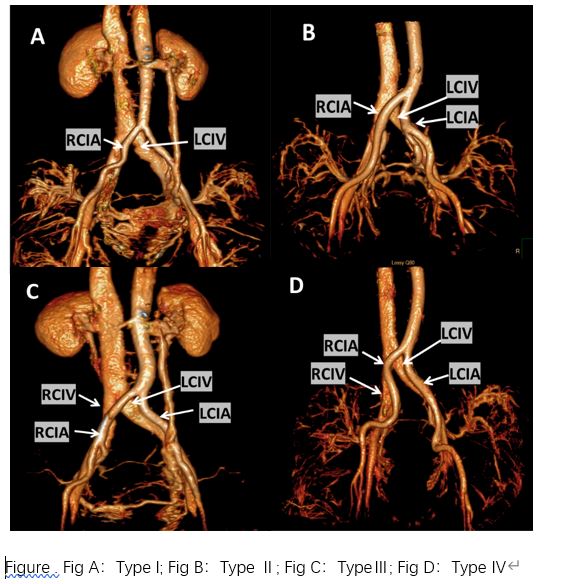
The number of visible stenosis was summarized in Table 1. Overall 244 stenosis in126 patients: inferior vena cava 8 stenosis, the junction of left common iliac vein and vena cava 115 stenosis, left common iliac vein 74 stenosis, left external iliac vein 1 stenosis , the junction of right common iliac vein and vena cava 2 stenosis, right common iliac vein 38 stenosis, right external iliac vein 6 stenosis [ZXY1] (Table 1). There were four types of compression divided by the location and frequency of iliac vein compression, and the evaluation results in stenosis and occlusion of vein by REACT had no statistical difference from those by catheter angiography (Table 2)Conclusion and Discussion
In our study, there is no statistical difference in the evaluation of iliac vein compression between REACT and catheter angiography. With comparable diagnostic accuracy to catheter angiography, REACT was proven to be a clinically applicable method for assessing iliac vein compression syndrome. which should help clinicians make better treatment plans for patients.Acknowledgements
noneReferences
1. Fabio H. Rossi, Antônio M. Kambara, Thiago O. Rodrigue, et al. Comparison of computed tomography venography and intravascular ultrasound in screening and classification of iliac vein obstruction in patients with chronic venous disease[J]. J Vasc Surg Venous Lymphat Disord. 2020 May;8(3):413-422.
2. Jiang J, Xu M, Chen Q, et al. Diagnosis and endovascular treatment of iliac venous compression syndrome [J]. Phlebology. 2019 Feb;34(1):40-51.
3.Yoneyama M, Zhang S, Hu HH, et al. Free-breathing noncontrast-enhanced flow-independent MR angiography using magnetization-prepared 3D non-balanced dual-echo Dixon method: a feasibility study at 3 Tesla[J]. Magn Reson Imaging, 2019, 63: 137-146.
4. Terwolbeck M N, Zhang S, Bode M, et al. Relaxation-enhanced angiography without contrast and triggering (REACT) for pelvic MR venography in comparison to balanced gradient-Echo and T2-weighted spin-Echo techniques[J]. Clinical Imaging, 2021.
5. Pennig L, Wagner A, Weiss K, et al. Imaging of the pulmonary vasculature in congenital heart disease without gadolinium contrast: Intraindividual comparison of a novel Compressed SENSE accelerated 3D modified REACT with 4D contrast-enhanced magnetic resonance angiography[J]. Journal of Cardiovascular Magnetic Resonance, 2020, 22.
Figures