1321
MR Multitasking-based Multi-dimensional Assessment of Cardiovascular System (MT-MACS): Initial Clinical Experience
Jiayu Xiao1, Yang Chen1, Xin Liu2, Zhehao Hu1, Debiao Li3, Anthony Christodoulou3, Parveen Garg4, Michael Fong4, Alison Wilcox4, Qi Yang2, and Zhaoyang Fan1,5,6
1Radiology, Keck School of Medicine of USC, Los Angeles, CA, United States, 2Beijing Chaoyang Hospital, Beijing, China, 3Cedars-Sinai Medical Center, Los Angeles, CA, United States, 4Cardiology, Keck School of Medicine of USC, Los Angeles, CA, United States, 5Radiation Oncology, Keck School of Medicine of USC, Los Angeles, CA, United States, 6Viterbi School of Engineering, University of Southern California, Los Angeles, CA, United States
1Radiology, Keck School of Medicine of USC, Los Angeles, CA, United States, 2Beijing Chaoyang Hospital, Beijing, China, 3Cedars-Sinai Medical Center, Los Angeles, CA, United States, 4Cardiology, Keck School of Medicine of USC, Los Angeles, CA, United States, 5Radiation Oncology, Keck School of Medicine of USC, Los Angeles, CA, United States, 6Viterbi School of Engineering, University of Southern California, Los Angeles, CA, United States
Synopsis
Keywords: Myocardium, Cardiomyopathy
Cardiovascular diseases are common causes of mortality and morbidity globally. An MR MultiTasking based 3D Multi-dimensional Assessment of Cardiovascular System (MT-MACS) technique has recently been developed to provide multi-contrast, cardiac phase-resolved imaging of the whole heart and thoracic aorta in a single scan without the need for ECG triggering or respiratory navigation. We aimed to assess the performance of MT-MACS in patients with suspicious cardiovascular diseases. We demonstrated the feasibility of using MT-MACS in a routine clinical setting. More importantly, it achieved good image quality in most patients with almost perfect inter-reader agreement and diagnostic accuracy.Introduction
Cardiovascular diseases, such as cardiomyopathy, masses, and aortic vasculopathy, are common causes of mortality and morbidity globally1. Imaging assessment of the cardiac and aortic structure and function is a key component for diagnosis, risk stratification, and procedural planning in patients with cardiovascular diseases. MR has the potential to meet this need. An MR MultiTasking based 3D Multi-dimensional Assessment of Cardiovascular System (MT-MACS) technique has recently been developed to provide multi-contrast, cardiac phase-resolved imaging of the whole heart and thoracic aorta in a single scan without the need for ECG triggering or respiratory navigation2. In this work, we conducted a clinical study to assess the performance of MT-MACS in patients with suspicious cardiovascular diseases.Methods
Patient populationPatients were prospectively enrolled into an IRB-approved MR study if they 1) were adults (≥18 years) with suspected cardiovascular diseases, 2) underwent transthoracic echocardiography, and 3) were able to undergo MR scan.
Image acquisition
All imaging studies were performed on a 3T MR scanner (MAGNETOM Vida; Siemens Healthcare, Erlangen, Germany) with a standard 18-channel body coil. MT-MACS was acquired either after initial three-plane localizer or 15 mins after intravenous administration of gadolinium-based contrast agent (0.1 mmol/kg of body weight) depending on the clinical indication. Major imaging parameters included: coronal orientation, FOV=224×224×162.4 mm3, spatial resolution=1.4×1.4×2.8 mm3 (interpolated to 1.4 mm isotropic), T2-prep duration=60 ms, TR=3.94 ms, TE1/TE2=1.23/2.46 ms, 500 FLASH readouts after each T2-IR. Total scan time takes 10 min 30 seconds. Image reconstruction was performed offline to generate water-only images with multiple contrast weightings (i.e. bright blood, dark blood, gray blood).
Image analysis
Two readers (5 years and 15 years of experience, respectively) analyzed the MT-MACS images blinded to clinical and other imaging data. Overall image quality was independently rated on a 4-point scale (0=nondiagnostic, 1=poor, 2=good, and 3=excellent). Cases with an average image quality<2 were excluded for further analysis. The readers then classified MT-MACS images by consensus according to the presence or absence of a) myocardial thickening, b) atrial/ventricular enlargement, c) intracardiac masses, d) aortic enlargement, and e) aortic wall pathologies, to evaluate diagnostic accuracy. Regarding the prespecified categories, preliminary results from MT-MACS were compared with the final clinical diagnoses based on clinical information and imaging examinations other than MT-MACS.
Statistical analysis
Inter-reader agreement in image scores and diagnostic accuracy were evaluated using Cohen’s kappa value (κ). κ was interpreted as follows: values ≤ 0 as indicating no agreement and 0.01-0.20 as none to slight, 0.21-0.40 as fair, 0.41-0.60 as moderate, 0.61-0.80 as substantial, and 0.81–1.00 as almost perfect agreement.
Results
MT-MACS was successfully performed in all enrolled 17 patients (12 males, 5 females, aged 30-74 years). Their clinical information and image quality scores are shown in Table 1. Of all the patients, two had additional transesophageal echocardiography, six had conventional cardiovascular MR. No patients received an image quality score of 0, two received 1, eight received 2, and seven received 3, resulting in a mean score of 2.3±0.7. Inter-reader agreement was almost perfect (κ = 0.88). Diagnostic accuracy was assessed in 15 patients with image quality scores ≥2 (Table 1). Aortic wall pathologies were only assessed in patients who underwent conventional MR due to limited assessment of the aortic wall by echocardiography. Using MT-MACS, myocardial thickening was correctly detected in 9 of 10 cases with no false-positive cases, atrial/ventricular enlargement was correctly detected in 6 of 7 cases with 1 false-positive, intracardiac masses were correctly detected in 1 case with no false-positive cases, aortic enlargement was correctly detected in 6 of 8 cases with no false-positive cases, and aortic wall pathologies was correctly detected in 1 case with no false-positive cases. The agreements between MT-MACS and clinical final diagnosis for myocardial thickening, atrial/ventricular enlargement, intracardiac masses, aortic enlargement, and aortic wall pathologies were substantial to almost perfect (κ = 0.88, 0.76, 1, 0.76, 1, respectively). The reason for the disagreement in diagnosis was ascribed to different criteria by MR and echo. Representative cases with negative findings, left ventricular hypertrophy, left atrial appendage, and aortic vasculitis are shown in Figures 2-5.Discussion
In this study, we demonstrated the feasibility of MT-MACS in a routine clinical setting. MT-MACS allowed for a comprehensive assessment of the whole heart and thoracic aorta with an ECG- and navigator-free scan. Echocardiography is currently the first choice for assessing cardiac structural and functional abnormalities owing to its wide availability and excellent cost-effectiveness balance. Meanwhile, MR can not only quantify the volume, function, and mass of the heart, but also characterize myocardial tissue and aortic vessel wall, potentially achieving a one-stop-shop assessment. Our technique is able to overcome the limitations of the conventional MR, including (a) long scan time, (b) cumbersome imaging paradigm with multiple scans, and (c) inefficiency in compensating for cardiac and respiratory motion during data acquisition. We achieved good image quality in most patients with almost perfect inter-reader agreement and diagnostic accuracy. The effectiveness of MT-MACS as a gatekeeper for cardiovascular diseases warrants further large-scale investigations.Conclusion
Our initial experience demonstrated the clinical feasibility of using MT-MACS for cardiac and aortic vessel assessment. Evaluation of its performance in more diverse cardiovascular diseases in comparison with corresponding clinical standards is underway.Acknowledgements
None.References
1. Mc Namara K, Alzubaidi H, Jackson JK. Cardiovascular dis-ease as a leading cause of death: how are pharmacists getting involved?Integr Pharm Res Pract. 2019;8:1-11.
2. Hu Z, Xiao J, Mao X, Xie Y, Kwan AC, Song SS, Fong MW, Wilcox AG, Li D, Christodoulou AG, Fan Z. MR Multitasking-based multi-dimensional assessment of cardiovascular system (MT-MACS) with extended spatial coverage and water-fat separation. Magn Reson Med. 2022 Nov 6. doi: 10.1002/mrm.29522. Epub ahead of print. PMID: 36336794.
Figures
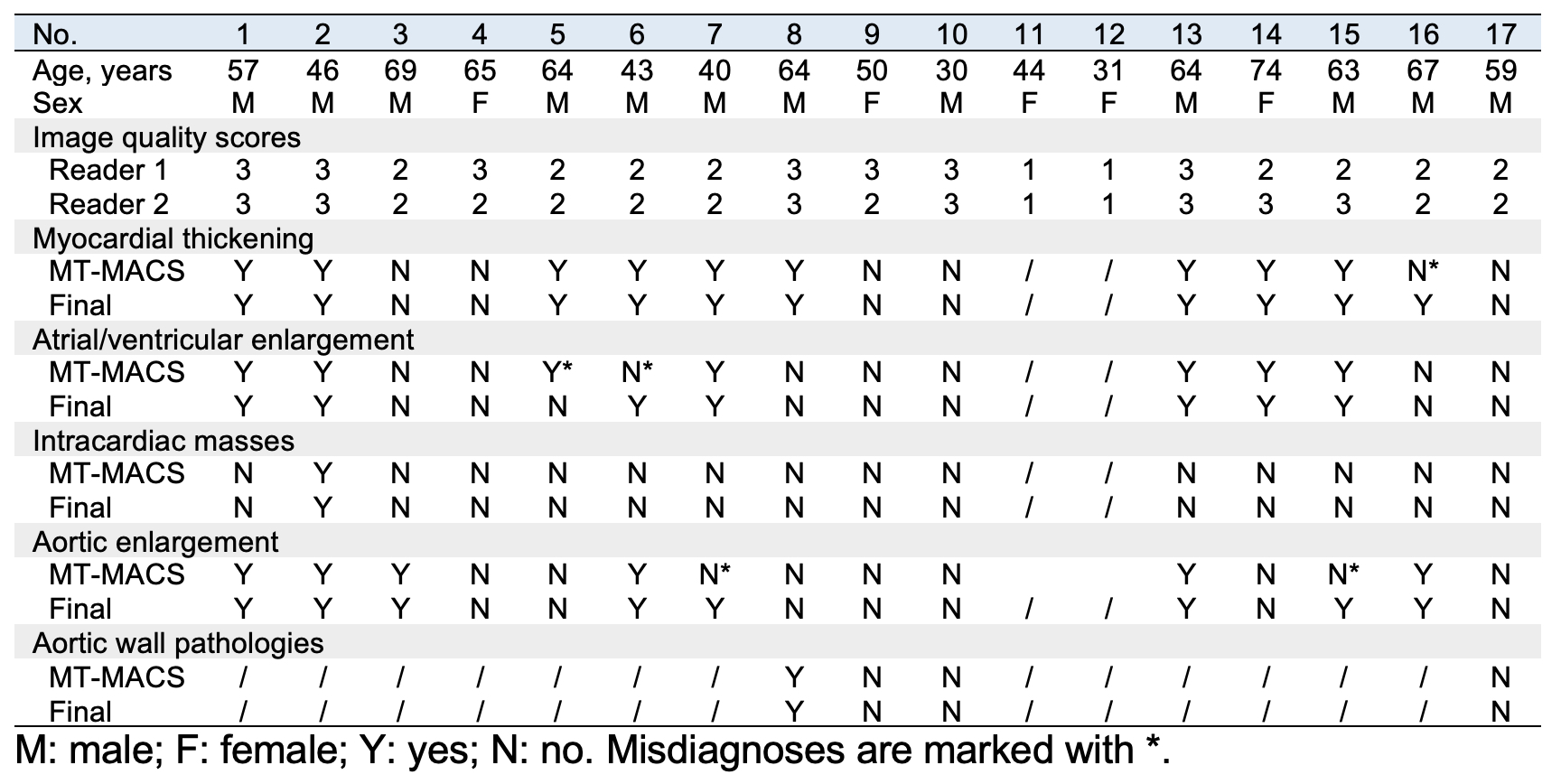
Figure 1. Clinical information, MT-MACS image quality scores and diagnostic accuracy
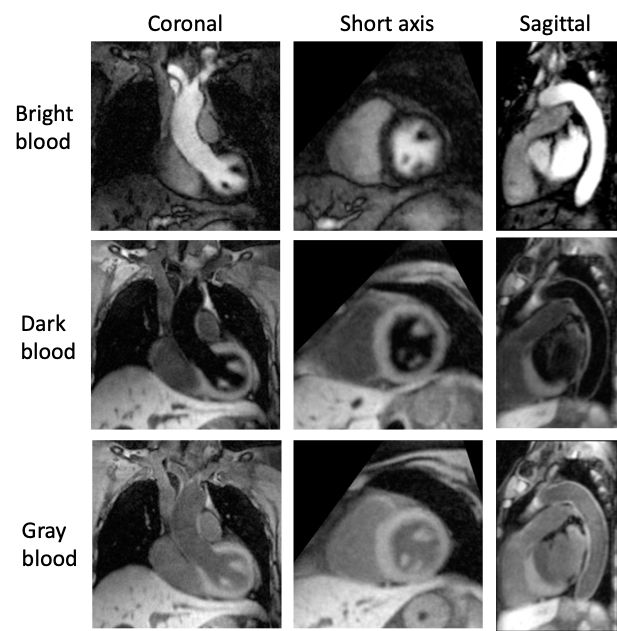
Figure 2. MT-MACS images from patient No. 10 with suspected right ventricular hypertrophy. Transthoracic echocardiogram both reported normal cardiac dimensions.
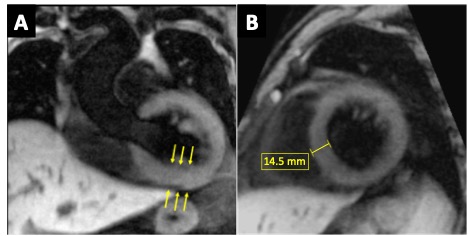
Figure 3. MT-MACS images of the end of diastolic phase from patient No. 7 with suspected left ventricular hypertrophy secondary to hypertension. Coronal view (A): a thickened left ventricular wall is recognized (arrows). Short axis view (B): left ventricular hypertrophy is evident, measuring 14.5 mm in the septal region. The diagnosis is confirmed by transthoracic echocardiogram.
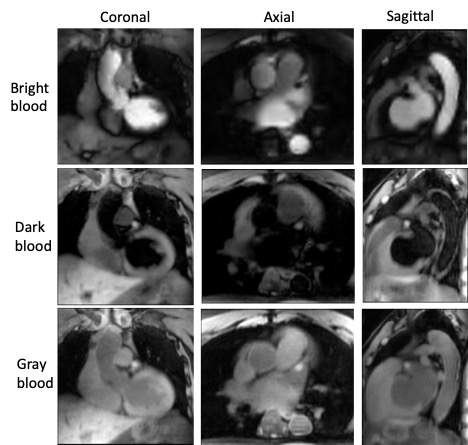
Figure 4. MT-MACS images from patient No. 2 with suspected left atrial appendage thrombus. A thrombus is identified as hypointense mass in the bright blood images and hyperintense mass in both dark blood and gray blood images. The diagnosis is confirmed by transesophageal echocardiogram.
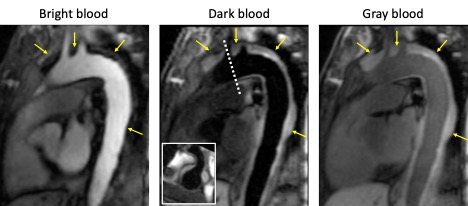
Figure 5. MT-MACS images from patient No. 8 with suspected aortic vasculitis. A thickened aortic wall withheterogeneous signal intensity is identified in all contrasts. The diagnosis is confirmed by conventional cardiac MRI.
DOI: https://doi.org/10.58530/2023/1321