1291
Time-encoded Arterial Spin Labeling for Renal Perfusion Quantification Covering the Whole Kidneys
Zihan Ning1, Zhensen Chen2, Shuo Chen1, Hualu Han1, Long Zhao3, Rui Wang4, Dongyue Si1, Huiyu Qiao1, Rui Shen1, and Xihai Zhao1
1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 3Department of Radiology, Beijing Anzhen Hospital, Beijing, China, 4Department of Radiology, Peking University First Hospital, Beijing, China
1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 3Department of Radiology, Beijing Anzhen Hospital, Beijing, China, 4Department of Radiology, Peking University First Hospital, Beijing, China
Synopsis
Keywords: Kidney, Perfusion, renal perfusion
We performed a series of optimization on the encoding scheme, pseudo-continuous ASL (pCASL) parameters, and post-processing of time-encoded pCASL (te-pCASL), then proposed Time-encoded Arterial Spin labeling to cover the whole Kidneys (TASK) to achieve multiple time-points renal perfusion measurement efficiently. With Gave of 0.4-0.6 mT/m and Gmax/Gave around 10, Walsh-Hadamard encoding scheme, and retrospective registration, TASK was able to provide accurate and reproducible RBF and ATT measurement covering the whole kidneys with single 5-min scan.Introduction
Arterial spin labeling (ASL) has become a novel MRI technique for renal perfusion measurement without contrast agent injection, whereas suboptimal post-labeling dalay (PLD) choice influences the accuracy of renal blood flow (RBF) measurement. Traditional multi-delay ASL requires an intolerant long scan time for repeated scans, though it provides more accurate and repeatable renal perfusion quantification. In this study, we performed a series of optimization on the encoding scheme, pCASL parameters, and post-processing of time-encoded pseudo-continuous ASL (te-pCASL), then proposed Time-encoded Arterial Spin labeling to cover the whole Kidneys (TASK) to achieve multiple time-points renal perfusion measurement in a single scan. The accuracy and reproducibility of TASK were evaluated in the young and elder healthy subjects.Methods
Sequence Design: The sequence diagram of TASK is shown in Figure 1A. Pre-saturation is applied to eliminate the impact on the signal dependence of TR and the residual labeled blood. The te-pcasl in 7×8 blocks is encoded in the Walsh-Hadamard scheme1 and followed by multi-slice EPI acquisitions.Sequence Optimization: 1) Considering the large variety of labeling efficiency for pcasl applied in the abdomen, the net average gradient (Gave) and rate of the amplitude of the slice-selective gradient (Gmax) and Gave (Gmax/Gave) of te-pcasl were determined by Bloch simulation according to the labeling blood velocity at the abdominal aorta measured by 2D phase contrast (PC) imaging; 2) Retrospective groupwise registration2 was performed to eliminate the motion artifacts; 3) The Walsh-Hadamard encoding scheme1 was implemented to achieve decoding with incomplete data in case of severe movements and halfway abortion during the scans.
MR Experiment: Ten young (age: 25.9 ± 3.7 years old, 5 female) and ten elder healthy subjects (age: 53.2 ± 5.8 years old, 5 female) and four patients with different kidney diseases were recruited for MRI experiments with informed consent. The experiments were conducted on the same MR scanner with a 16-channel torso coil and a 12-channel posterior coil. For all subjects, a 2D PC was firstly conducted as a scout scan to obtain the mean labeling blood velocity at the labeling plane in the abdominal aorta. The best Gave and Gmax/Gave values were immediately calculated based on the average labeling blood velocity by Bloch simulation and applied to the all following ASL sequences. Subsequently, a traditional sequential multi-delay pcasl sequences (SMD) and three versions of TASK (TASKfix, TASKadj and TASKfree) were performed in secession (Figure 1C). The PLD and labeling duration of SMD and all TASK techniques were optimized with the method used by Woods JG et al1. Five subjects of the young (mean age: 26.0 ± 3.2 years old, 2 female) and five subjects of the elder groups (mean age: 51.6 ± 6.2 years old, 2 female) were randomly selected to undergo the reproducibility experiments.
Image Analysis: All analyses were performed on MATLAB (Mathworks, Natick). To minimize the impact of respiratory motion on image quality, all acquisitions of SMD, TASKfix, TASKadj and TASKfree were internally registered by the PCA-based groupwise registration2 using Elastix3 mentioned above. For the TASK sequences, the acquisitions were firstly decoded according to the Walsh-Hadamard encoding scheme4 to obtain the PWI at 7 PLDs. The classic Buxton kinetic model5 was used for quantitating RBF and ATT for the four sequences. The PWI decoded from the incomplete data (TASK-2 for 1×2 encoding blocks and TASK-4 for 3×4 encoding blocks) for the three versions of TASKs were also calculated, and corresponding RBF and ATT results were fitted by the same kinetic model. The root-mean-squared error (RMSE) of fitting was also calculated. The ground truth RBF and ATT estimates were generated by fitting the combined data from all of the ASL sequences (~20 min scan time of data), similar to the method proposed by Woods JG et al6.
Results
Figure 2 shows the representative of the RBF and ATT ground truth and the RBF, ATT, RBF error, ATT error and RMSE maps obtained by SMD, TASKfix, TASKadj, and TASKfree. Figure 3 shows the representative quantitative image of the four patients. There was no significant difference in RBF between the young and elder groups (211.25±42.06 vs. 196.39±35.71 mL/100g/min, P>0.05), while ATT of the elder group was longer than that of the young group (663.05±199.91 vs. 789.68±149.89 ms). Gave of 0.4-0.6 mT/m and Gmax/Gave around 10 was executable for TASK techniques. Compared with SMD, RBF and ATT measured by TASK techniques were in better and excellent agreement (ICC: 0.932-0.986, R2 = 0.92-0.95 vs. ICC: 0.769-0.902, R2 = 0.40-0.74) and had significantly smaller errors (P<0.001) with the ground truth (Figure 4). Among TASK techniques, the RMSE of TASKfree was relatively higher than the others (P<0.05) (Figure 4). All TASK techniques showed excellent reproducibility (ICC, 0.897-0.987, R2 = 0.70-0.99, CV = 3.45-9.28%), which were better than SMD (ICC: 0.655-0.940, R2 = 0.57-0.81, CV = 7.71-15.20%) (Figure 5).Discussion and Conclusion
With Gave of 0.4-0.6 mT/m and Gmax/Gave around 10, Walsh-Hadamard encoding scheme, and retrospective registration, TASKfix and TASKadj were able to provide accurate and reproducible RBF and ATT measurement covering the whole kidneys with single 5-min scan.Acknowledgements
None.References
- Woods JG, Chappell MA and Okell TW. Designing and comparing optimized pseudo-continuous Arterial Spin Labeling protocols for measurement of cerebral blood flow. Neuroimage 2020; 223: 117246.
- Huizinga W, Poot DH, Guyader JM, et al. PCA-based groupwise image registration for quantitative MRI. Med Image Anal 2016; 29: 65-78.
- Klein S, Staring M, Murphy K, et al. elastix: a toolbox for intensity-based medical image registration. IEEE Trans Med Imaging 2010; 29: 196-205.
- von Samson-Himmelstjerna F, Madai VI, Sobesky J, et al. Walsh-ordered hadamard time-encoded pseudocontinuous ASL (WH pCASL). Magn Reson Med 2016; 76: 1814-24.
- Buxton RB, Frank LR, Wong EC, et al. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med 1998; 40: 383-96.
- Woods JG, Chappell MA and Okell TW. A general framework for optimizing arterial spin labeling MRI experiments. Magn Reson Med 2019; 81: 2474-88.
Figures
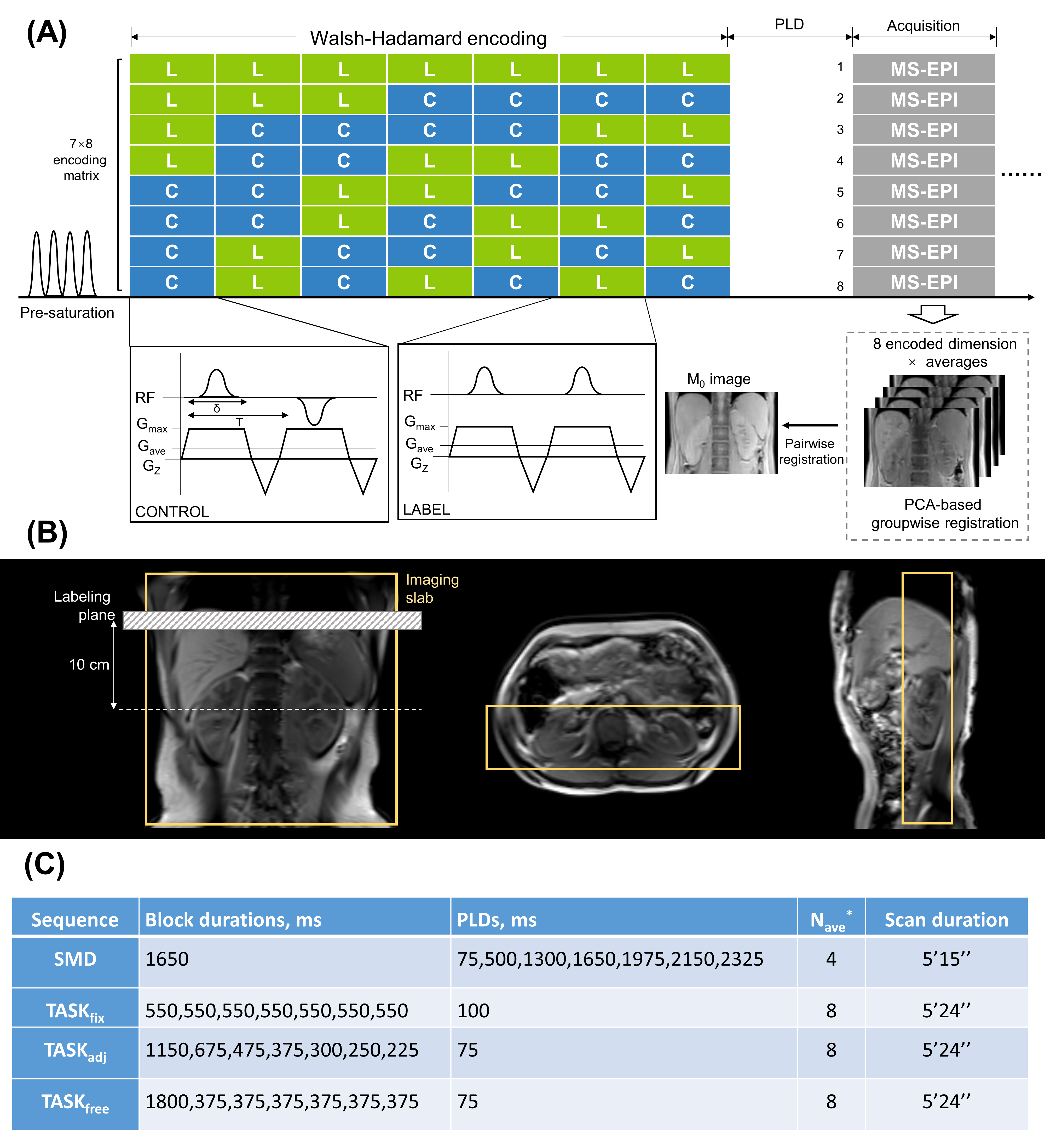
Figure 1. The sequence diagram (A), positioning diagram
(B) and the timings (C) of TASK.
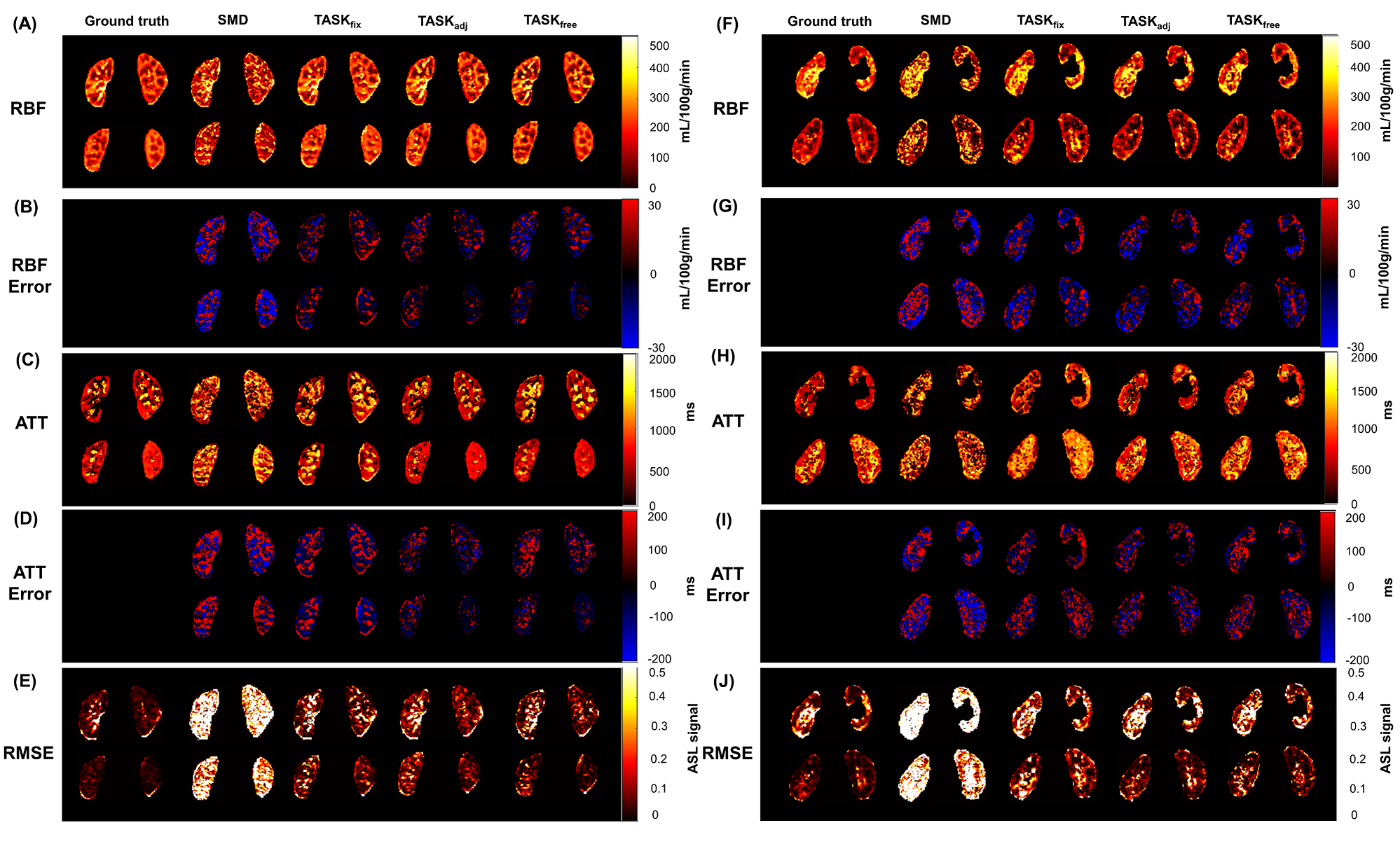
Figure 2. The RBF (A, F), RBF
error (B, G), ATT (C, H), ATT error (D, I) and RMSE (E, J) maps of the ground
truth estimation, SMD, TASKfix, TASKadj, TASKfree
of one 24-year-old female healthy subject (A-E) and one 61-year-old female
healthy subject (F-J).
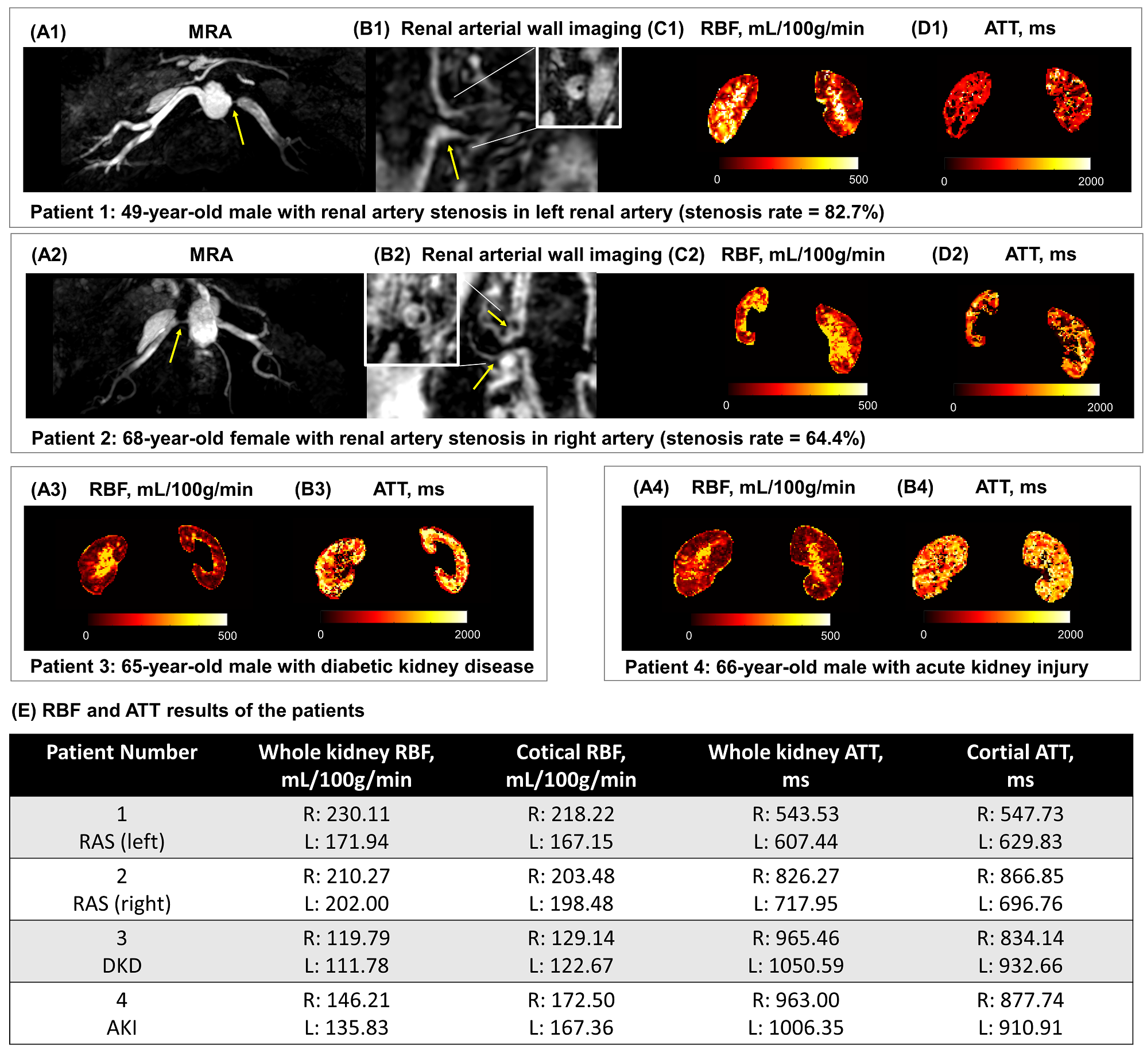
Figure 3. The
MRA (A1, A2), renal arterial wall imaging (B1, B2), RBF (C1, C2, A3, A4) and
ATT maps (D1, D2, B3, B4) of four patients with different renal diseases with
the RBF and ATT quantitative results (E). RAS, renal artery stenosis; DKD,
diabetic kidney disease; AKI, acute kidney injury.
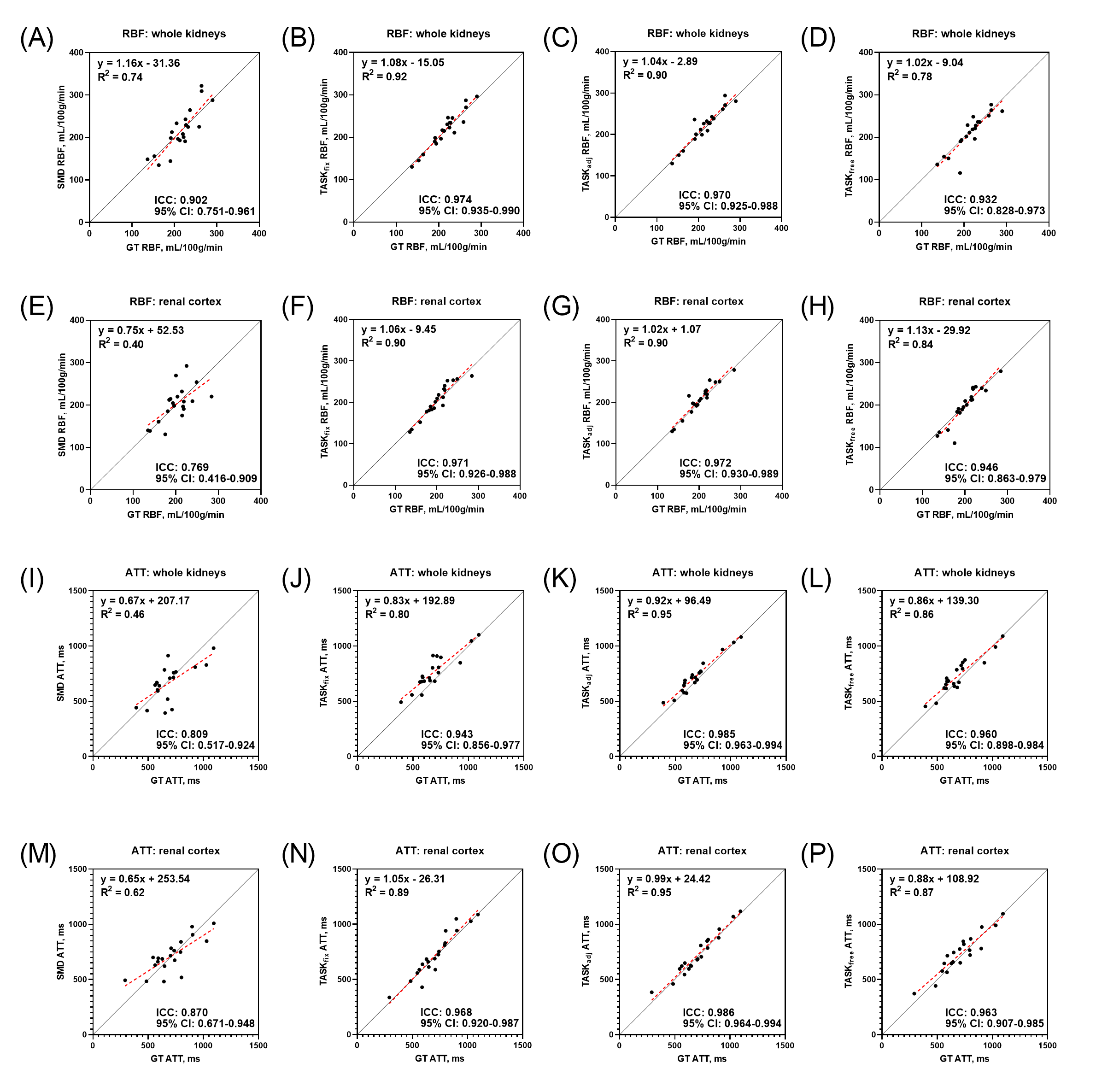
Figure 4. The linear regression and ICC results
of RBF and ATT between the ground truth and SMD, TASKfix, TASKadj
and TASKfree in the whole kidneys and renal cortex.
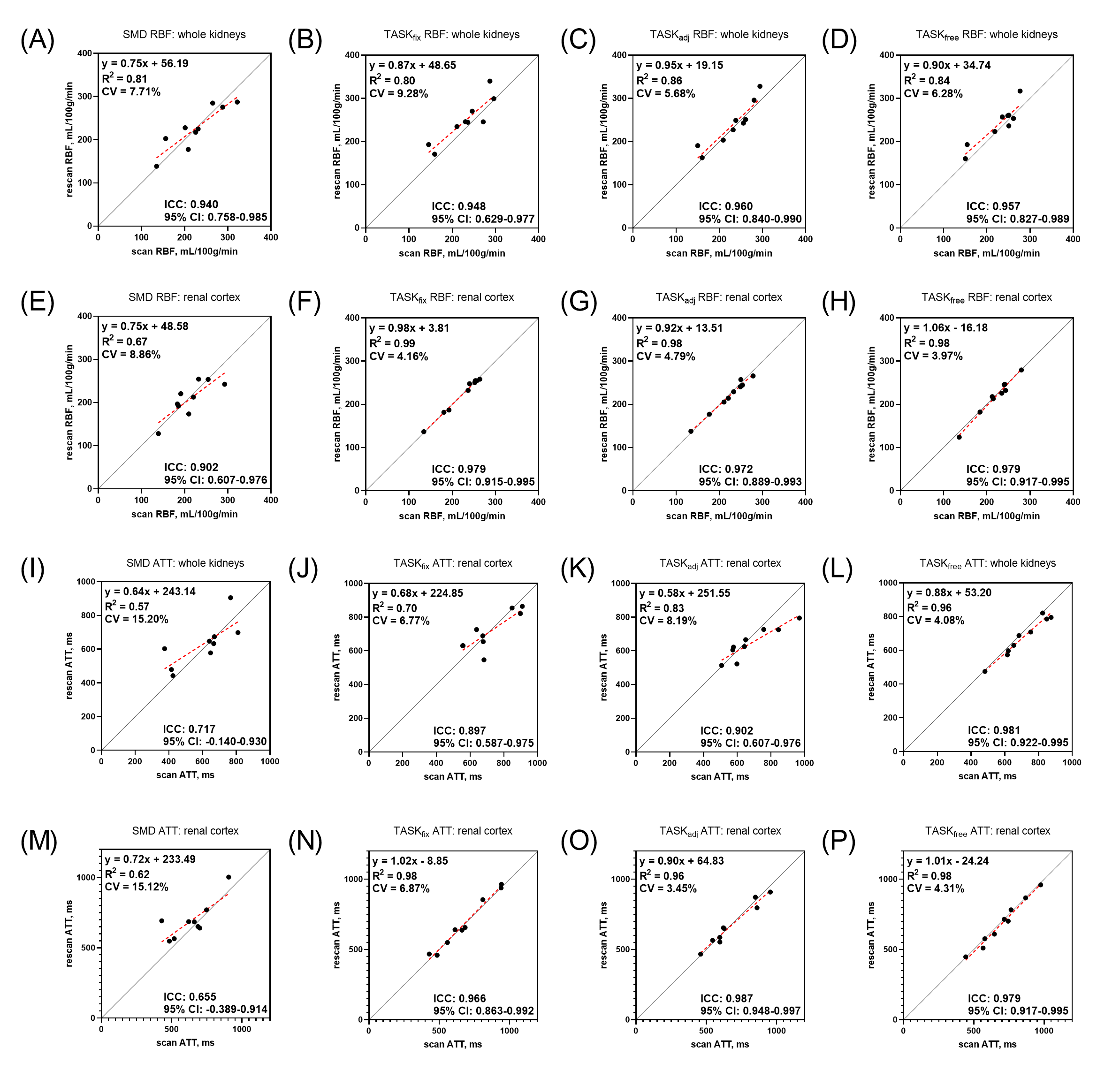
Figure 5. The linear regression, ICC and CV results of RBF and ATT
between the scan and rescan of SMD, TASKfix, TASKadj and
TASKfree in the whole kidneys and renal cortex.
DOI: https://doi.org/10.58530/2023/1291