1290
Initial Experience of Hyperpolarized [1-13C]pyruvate MRI in Kidney Transplant Patients1Department of Radiology & Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital at Linkou, Tainwan, Taiwan, 3Department of Medicine, University of California, San Francisco, San Francisco, CA, United States, 4Department of Pathology, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Kidney, Hyperpolarized MR (Non-Gas)
We present our initial experience of applying hyperpolarized (HP) [1-13C]pyruvate MRI in three patients with renal allograft. The pyruvate metabolism to lactate and bicarbonate in two patients with well functioning allografts and normal biopsy was in the range of healthy native kidneys. The allograft pyruvate metabolism in the third patient with reduced eGFR was higher than that of healthy native kidneys. Study is ongoing to establish the range of pyruvate metabolism in normal allografts and to correlate pyruvate metabolism to allograft biopsy. This study paves the way for investigation of HP MRI in the noninvasive assessment of kidney allograft injury.Introduction
Kidney transplant is the treatment of choice for patients with end-stage renal disease. Early detection of allograft injury and timely intervention are critical to delay or prevent irreversible damage. Current noninvasive methods for monitoring kidney allograft such as measuring serum creatinine have significant limitations. Biopsy remains the standard for assessing allograft injury, however it is invasive and is associated with complications. Increasing evidence indicates that perturbed energy metabolism, such as a shift from oxidative phosphorylation to glycolysis, plays a key role in various kidney diseases, including allograft injury. Hyperpolarized (HP) 13C MRI allows for dynamic measurements of energy metabolism in various diseases. In this work, we present our initial experience of applying HP [1-13C]pyruvate MRI to assess energy metabolism in patients with kidney allograft.Methods
Patients with kidney allograft who were already scheduled for allograft biopsy (either surveillance or for-cause biopsies) were recruited under an institutional review board approved protocol. MRI scans were performed prior to the biopsy on a GE 3T scanner (MR750, GE Healthcare, Waukesha, WI) with a semi-flexible quadrature transmit and 8-channel array receive (QTAR) coil (Clinical MR Solutions, Brookfield, WI, USA). [1-13C]pyruvate was polarized by GE SPINlab polarizer (GE Healthcare, Waukesha, WI) operating at 5T and 0.8K. The dissolution-to-injection time was 68.5±7.2s. 13C acquisitions were triggered by bolus tracking on the kidney allografts using RTHawk platform (HeartVista, Los Altos, CA) along with real-time frequency and B1 calibration1. Pyruvate was acquired by spectral-spatial 2D gradient-echo sequence1, and lactate and bicarbonate by a spectral-spatial 3D bSSFP sequence2. Scan parameters were 1cm in-plane resolution for pyruvate and lactate, 2cm in-plane resolution for bicarbonate, 21mm slice thickness, 20° flip angle for pyruvate, 60° flip angle for lactate and bicarbonate, 3.5s temporal resolution. Images were acquired during free breathing. When feasible, two repeated injections separated by 20 minutes were performed to assess repeatability. In the second HP 13C injection, 13C images were acquired in a lower resolution: 1.5cm in-plane resolution for pyruvate and lactate, 2.5cm in-plane resolution for bicarbonate, while the other acquisition parameters were the same. Data from the kidney allografts were also compared to those from native kidneys from five healthy volunteers who were scanned previously with the same acquisition setting.Results and Discussion
To date, 3 patients with renal allograft were successfully imaged with HP [1-13C]pyruvate MRI. Figure 1 shows the area-under-curve (AUC) images of the three kidney allografts and one of the native healthy kidneys. The representative dynamic metabolite images in two renal allografts are presented in Figure 2. Tables 1 and 2 show the lactate-to-pyruvate and bicarbonate-to-pyruvate ratios of the kidney allograft which were very similar across two different slices. Patients #1 and #2 had well functioning allografts and underwent surveillance biopsy following the MRI with biopsy showing well-preserved allograft without evidence of rejection. Compared to the native healthy kidneys, the kidney allografts from patients #1 and #2 show comparable lactate-to-pyruvate and bicarbonate-to-pyruvate ratios. Compared to the native healthy kidneys, the allograft from patient #3 has a higher lactate-to-pyruvate ratio and higher bicarbonate-to-pyruvate ratio. This patient has not had allograft biopsy to date, and the etiology for the elevated metabolite ratio is unclear. Patient #3 had a urinary tract infection and lower than baseline eGFR at the time of the MRI, and was also taking immunosuppressants. It is possible that the elevated lactate-to-pryuvate and bicarbonate-to-pyruvate may be related to the urinary tract infection that patient experienced.Patient #2 had two repeated HP [1-13C]pyruvate injections followed by MRI. The metabolite AUC images of the two repeated injections for patient #2 are shown in Figure 3. With a higher spatial resolution, the images from the first injection show a sharper edge but a lower signal-to-noise ratio. Images from the repeated injections show similar lactate-to-pyruvate and bicarbonate-to-pyruvate, suggesting repeatability.3
Conclusion
We present the first data of HP [1-13C]pyruvate MRI in kidney transplant patients. Metabolites lactate and bicarbonate were observed with excellent signal-to-noise ratio. Two of the patients with well functioning allografts and normal biopsy showed pyruvate metabolism similar to healthy native kidneys. The study is ongoing and enrolling additional patients to establish range of pyruvate metabolism in normal allografts and to correlate pyruvate metabolism to allograft biopsy findings. This initial study paves the way for the investigation of HP MRI in the noninvasive assessment of kidney allograft injury.Acknowledgements
This work was supported by the US National Institute of Health grants R21DK130002 andP41EB013598.References
1. Tang S, Milshteyn E, Reed G, et al. A regional bolus tracking and real-time B1 calibration method for hyperpolarized 13C MRI. Magn Reson Med. 2019;81(2):839-851. doi:10.1002/mrm.273912.
2. Tang S, Bok R, Qin H, et al. A metabolite-specific 3D stack-of-spiral bSSFP sequence for improved lactate imaging in hyperpolarized [1-13C]pyruvate studies on a 3T clinical scanner. Magn Reson Med. 2020;84(3):1113-1125. doi:10.1002/mrm.282043
3. Tang S, Meng M v., Slater JB, et al. Metabolic imaging with hyperpolarized 13C pyruvate magnetic resonance imaging in patients with renal tumors—Initial experience. Cancer. 2021;127(15):2693-2704. doi:10.1002/cncr.33554
Figures
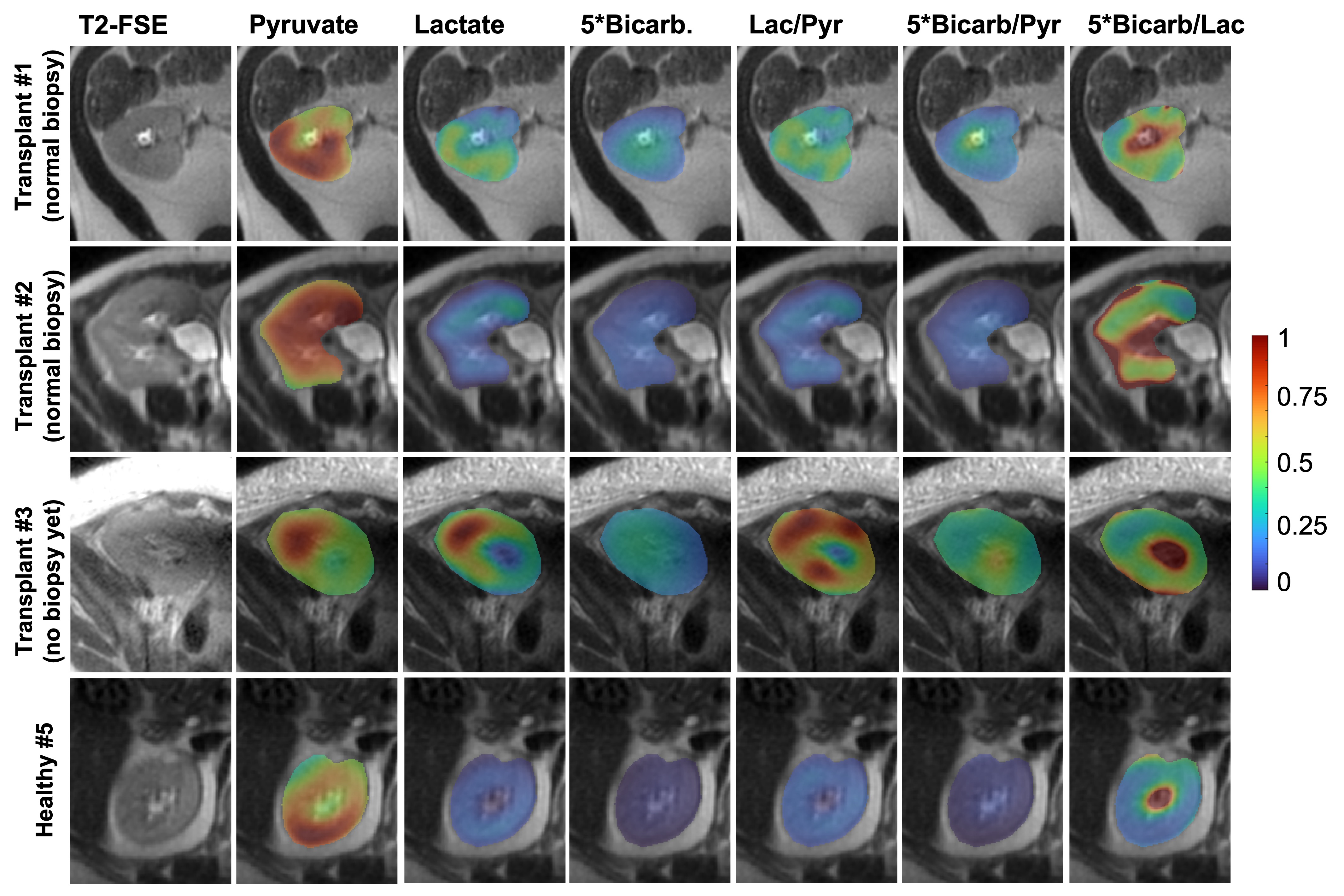
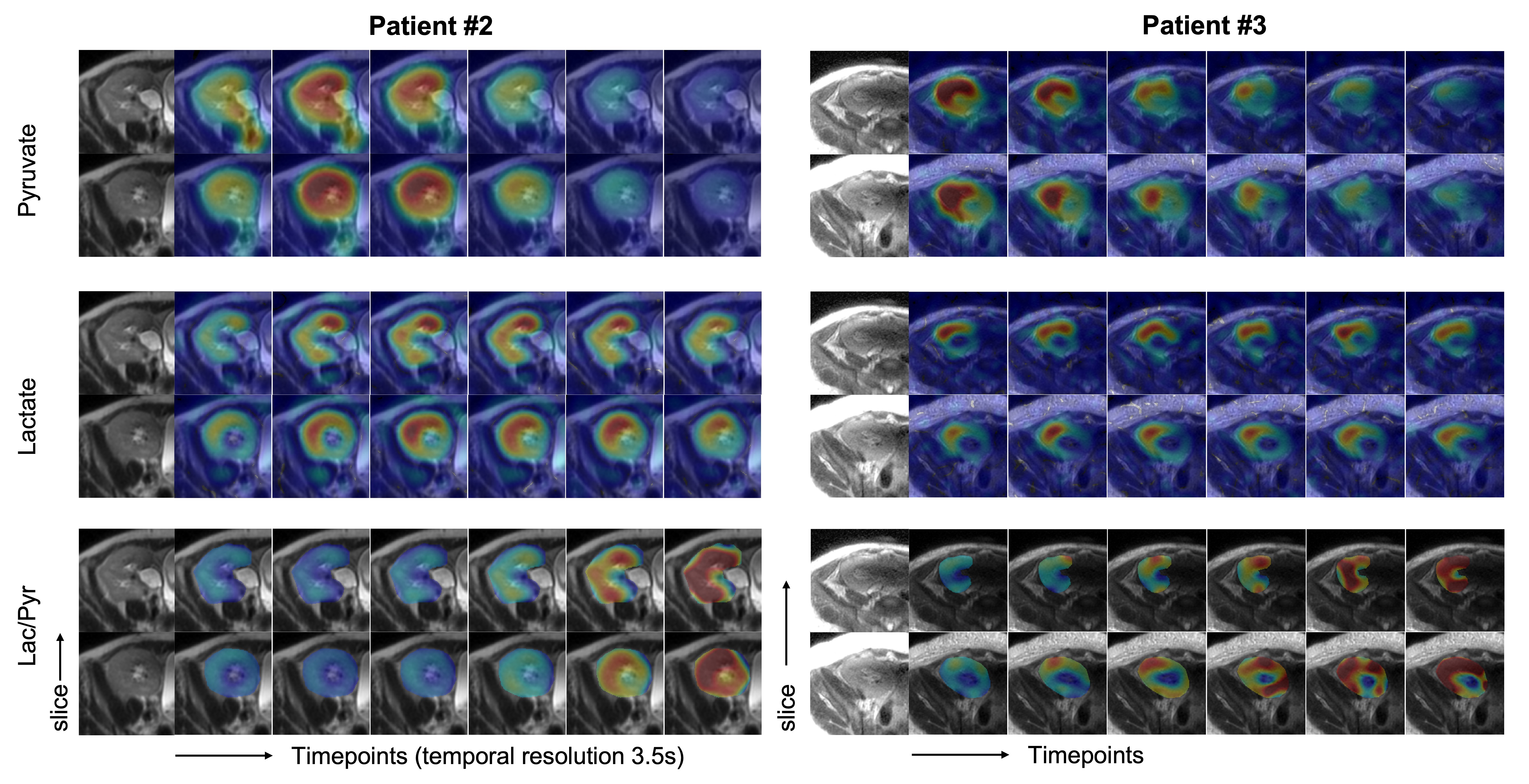
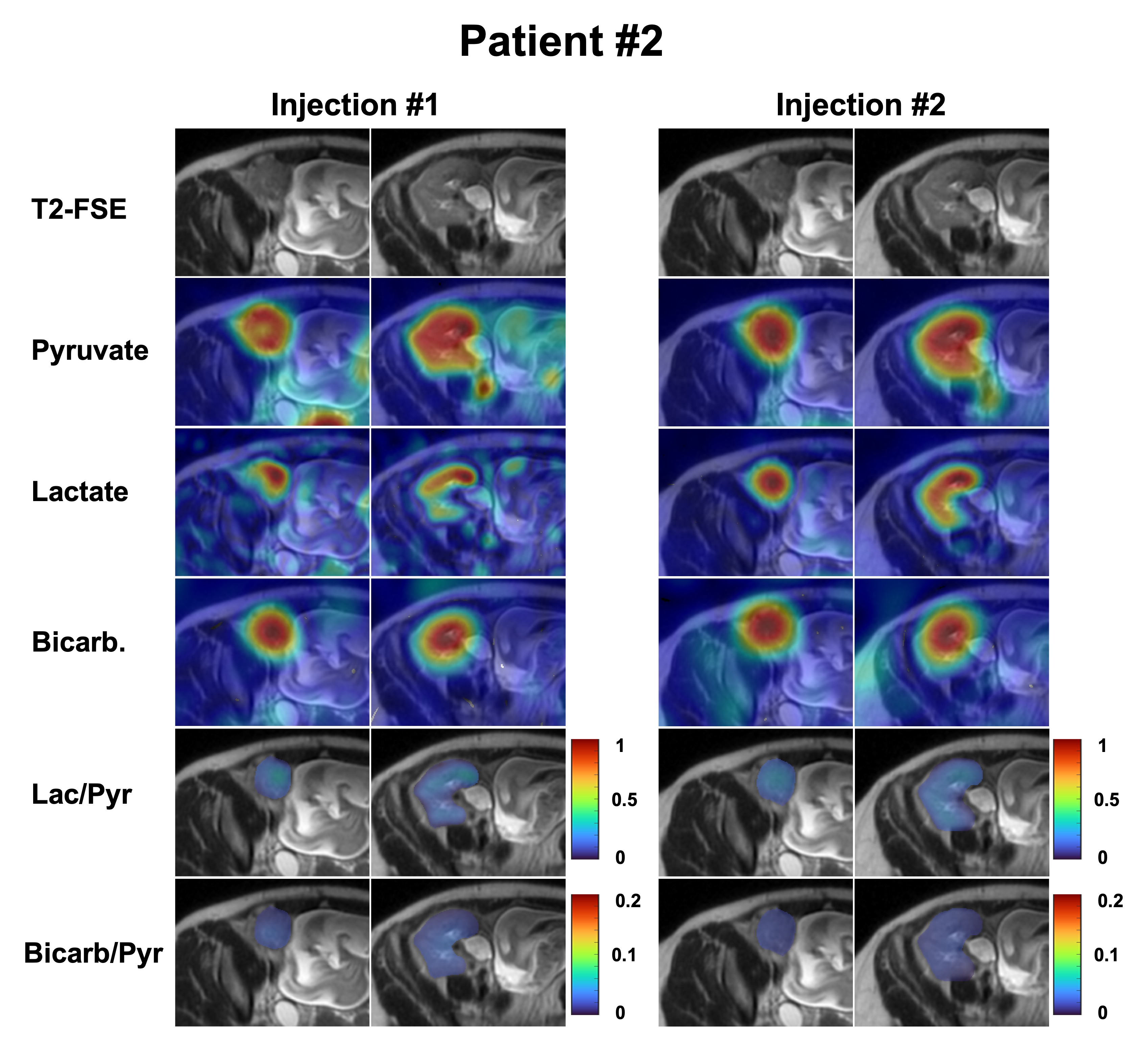
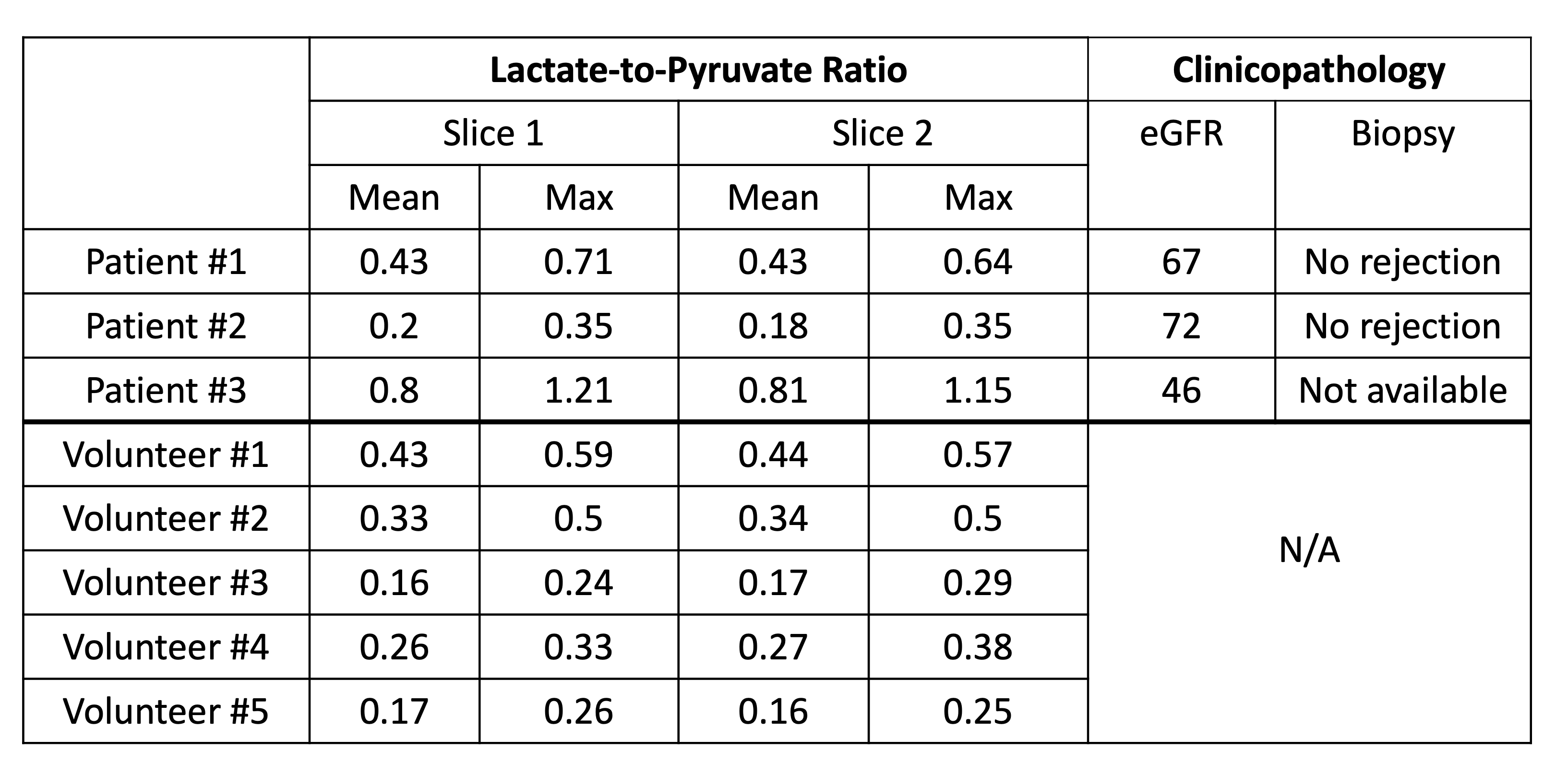
Table 1: Lactate-to-pyruvate ratio and clinicopathology of the patients.
Note: The ratios were measured over the kidney on two different slices.
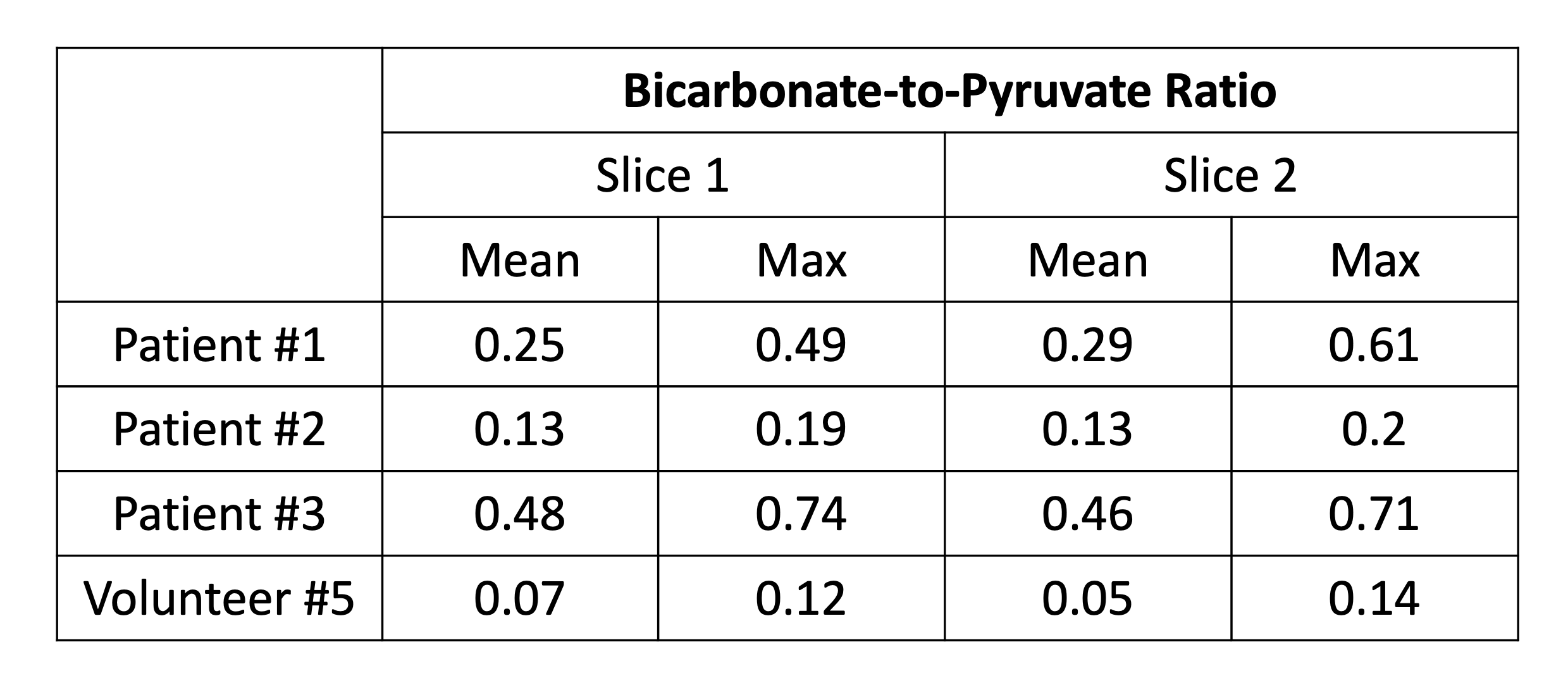
Table 2: Bicarbonate-to-pyruvate ratio of renal allografts and native kidneys from a healthy volunteer.
Note: The ratios were measured over the kidney on two different slices.