1246
Fetal 3D cine cardiovascular MRI: Improved image quality with region-optimized virtual coils
Marjolein Piek1, Johannes Töger1, Erik Hedström1,2, and Anthony H. Aletras1,3
1Clinical Physiology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden, 2Diagnostic Radiology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden, 3Laboratory of Computing, Medical Informatics and Biomedical-Imaging Technologies, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece
1Clinical Physiology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden, 2Diagnostic Radiology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden, 3Laboratory of Computing, Medical Informatics and Biomedical-Imaging Technologies, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece
Synopsis
Keywords: Fetal, Image Reconstruction
Recently, the first 3D cine radial acquisition of the fetal heart with isotropic resolution was introduced. However, image quality suffers from radial streaking artifacts due to under-sampling. A new coil combination method, Region-Optimised Virtual coils (ROVir), was suggested to improve image quality by highlighting signal from the ROI while suppressing signal from unwanted regions. This study aimed to compare 3D fetal cardiac imaging ROVir to conventional SVD-based coil combination, in a parallel imaging based reconstruction. Streaking artifacts were reduced, and the cine could be reconstructed to more cardiac phases. This allowed for improved appreciation of fetal cardiac function.Introduction
Fetal cardiovascular MRI has shown value as an important tool for diagnosing congenital heart defects (CHD) already before birth1. Recently, the first 3D cine acquisition of the fetal heart with isotropic resolution was introduced with the potential to reduce examination time and to simplify image planning2. However, image quality suffers from radial streaking artifacts due to under-sampling. Also, high computational power is required for image reconstruction, thus limiting the reconstructed number of time frames per cardiac cycle. Region-Optimized Virtual (ROVir) coil combination was recently introduced to improve image quality by highlighting signal from the region of interest (ROI), while at the same time suppressing signal from unwanted regions within the field of view (FOV)3. This is in contrast to conventional coil combination using singular value decomposition (SVD), which instead selects coil combinations with the highest possible total signal, regardless of the ROI.We hypothesized that by using ROVir to select only the coil combinations most sensitive to the region of interest, i.e., the fetal heart, radial streaking could be minimized, and computation times for image reconstruction could be shortened. Therefore, this study aimed to compare ROVir coil combination to a conventional SVD-based coil combination algorithm.
Methods
Sequence designA 3D slab-selective radial balanced steady-state free precession (bSSFP) research pulse sequence with a double golden-angle radial k-space trajectory was used for data acquisition, as previously described4. Scan parameters were: TE = 1.58 ms, TR = 3.54 ms, flip angle 46°, isotropic voxel size 1.9 mm3, isotropic FOV 360 mm3, BW = 1085 Hz/pixel and acquisition time = 3.9 minutes. The examination was performed at normal operating mode, with specific absorption rate constrained to 2 W/kg, thereby limiting the flip angle.
In vivo study
Two coil combination algorithms, SVD and ROVir, were tested in one fetus (32 gestational weeks) with ventricular asymmetry. The Ethics Review Board approved the study and written informed consent was obtained from the pregnant woman before participation. The fetal cardiac MRI exam was performed on a 1.5 T MAGNETOM Aera scanner using the anterior 18-channel array coil and the 32-channel spine array coil (Siemens Healthcare, Erlangen, Germany). The 3D imaging volume covered the entire fetus and was acquired during maternal free breathing. For fetal cardiac gating, an MRI-compatible Doppler Ultrasound (DUS) gating device was used (smart-sync, Northh medical GmbH, Hamburg, Germany)5.
Image reconstruction
The 3D cine reconstruction pipeline is shown in Figure 1. The Berkeley Advanced Reconstruction Toolbox (BART)6 interfaced with Matlab (R2019a, MathWorks, Natick, MA, USA) was used for image reconstruction. The raw k-space data was pre-whitened and then coil combination, to speed up image reconstruction and reduce the computational load, was applied. Coil combination was performed using either SVD or ROVir resulting in 3 or 8 virtual coils, respectively. Figure 2 shows the volume of interest (VOI) (green area) and the volume of interference (red area) in the three orthogonal views for the ROVir reconstruction. Sensitivity maps were estimated using ESPiRIT7, and the radial spokes were binned to their corresponding cardiac phase using the DUS triggers. The image reconstruction minimization problem (Figure 1d) was solved by performing a parallel imaging and compressed sense reconstruction8. The optimization problem was solved for SVD and ROVir in an iterative fashion with 30 iterations, creating 8 and 16 cardiac phases for SVD and ROVir respectively. All reconstructions were performed using 16 threads on an 18-core Xeon Gold 5520R CPU (Intel, Mountain View, CA, USA) running at 2.2 GHz with 1.5 TB random-access memory (RAM).
Results
A 3D cine with ROVir coil combination was successfully reconstructed. Figure 3 compares the results of the ROVir-based reconstruction with the SVD-based coil combination. Radial streaking artifacts were reduced within the VOI in the ROVir-based reconstructed images. Signal intensities inside the VOI were increased, whereas signal intensities outside the VOI were reduced.Figure 4 shows cardiac function in a short-axis image reconstructed with both SVD and ROVir from the acquired 3D cine volume. The reconstructed temporal resolutions are 66 ms and 33 ms respectively. Figure 5 shows image quality differences between the SVD-based and ROVir-based reconstruction.
Image reconstruction computational demands were independent of the coil combination method, but were based on the number of iterations, reconstructed cardiac phases and virtual coils. A reconstruction with 30 iterations, 16 cardiac phases and 3 virtual coils took 949 GB RAM and 99 minutes. A reconstruction with 8 cardiac phases and 8 virtual coils took 567 GB and 113 minutes. A reconstruction with 16 cardiac phases and 8 virtual coils resulted in a memory overflow and was not feasible.
Discussion
The ROVir coil combination resulted in reduced radial streaking artifacts, thereby allowing for a reconstruction with a small number of virtual coils. This decreased the computational load and allowed for more cardiac phases to be reconstructed.Conclusions
ROVir coil combination was successfully implemented for fetal cardiac MRI. In comparison with the standard SVD approach, ROVir coil combination showed reduced radial streaking artifacts, and as computing load was decreased, 16 instead of 8 cardiac phases were reconstructed, which in turn allowed for improved appreciation of fetal cardiac function.Acknowledgements
We thank Dr. Frederik Testud, Siemens Healthcare AB, Malmö, Sweden, for useful discussions.
References
1. Ryd D, Fricke K, Bhat M, Arheden H, Liuba P, Hedström E. Utility of Fetal Cardiovascular Magnetic Resonance for Prenatal Diagnosis of Complex Congenital Heart Defects. JAMA Netw Open. 2021;4(3):e213538. doi:10.1001/jamanetworkopen.2021.35382. Piek M, Ryd D, Töger J, Testud F, Hedström E, Aletras AH. Fetal 3D cardiovascular cine image acquisition using radial sampling and compressed sensing. Magn Reson Med. 2022. doi:10.1002/mrm.29467
3. Kim D, Cauley SF, Haldar JP. optimized virtual ( ROVir ) coils : Localization and / or suppression of spatial regions using sensor- domain beamforming. Magn Reson Med. 2021;(January):1-16. doi:10.1002/mrm.28706
4. Chan RW, Ramsay EA, Cunningham CH, Plewes DB. Temporal stability of adaptive 3D radial MRI using multidimensional golden means. Magn Reson Med. 2009;61(2):354-363. doi:10.1002/mrm.21837
5. Kording F, Schoennagel B, Lund G, et al. Doppler ultrasound compared with electrocardiogram and pulse oximetry cardiac triggering: A pilot study. Magn Reson Med. 2015;74(5):1257-1265. doi:10.1002/mrm.25502
6. Uecker M, Ong F, Bahri D, et al. Berkeley Advanced Reconstruction Toolbox. Proc Intl Soc Mag Reson Med. 2015;23:2486.
7. Uecker M, Lai P, Murphy MJ, et al. ESPIRiT - An eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magn Reson Med. 2014;71(3):990-1001. doi:10.1002/mrm.24751
8. Feng L, Grimm R, Block KT obia., et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2014;72(3):707-717. doi:10.1002/mrm.24980
Figures
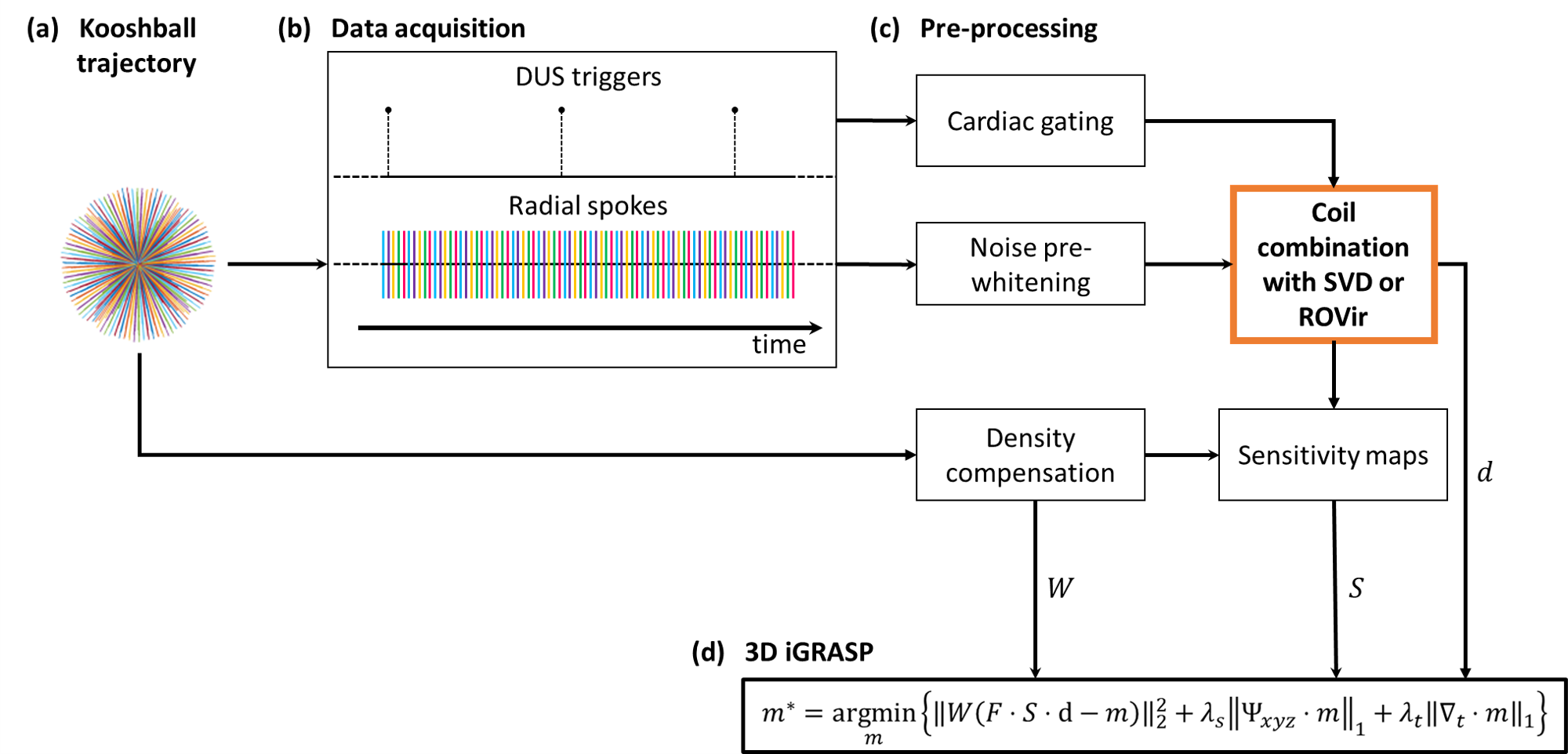
Figure 1. Flowchart of the fetal image acquisition and reconstruction pipeline. A 3D kooshball trajectory was prescribed to acquire the k-space data (a). The Doppler Ultrasound signal was obtained during the acquisition (b). Pre-processing included gating, pre-whitening, coil combination (SVD or ROVir), estimation of coil sensitivity maps, and density compensation (c). The 3D minimization problem was then solved with parallel imaging and compressed sensing (d).
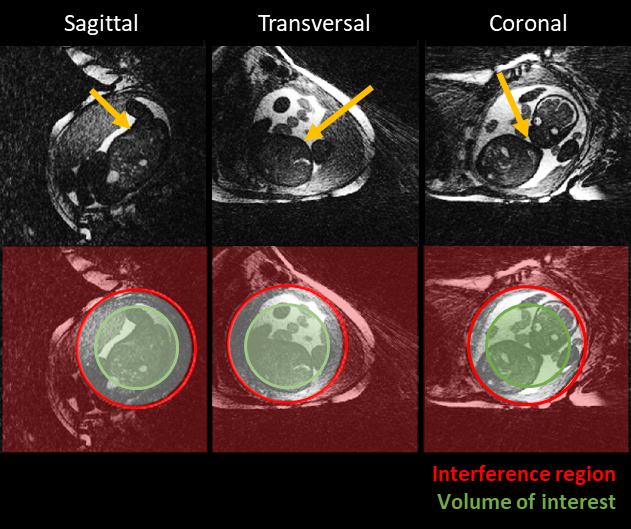
Figure 2. The volume of interest (area withing the green circle) and the volume of interference (area outside the red circle) are shown in the sagittal (left), transversal (middle) and coronal view (right). The yellow arrows point at the fetal heart.
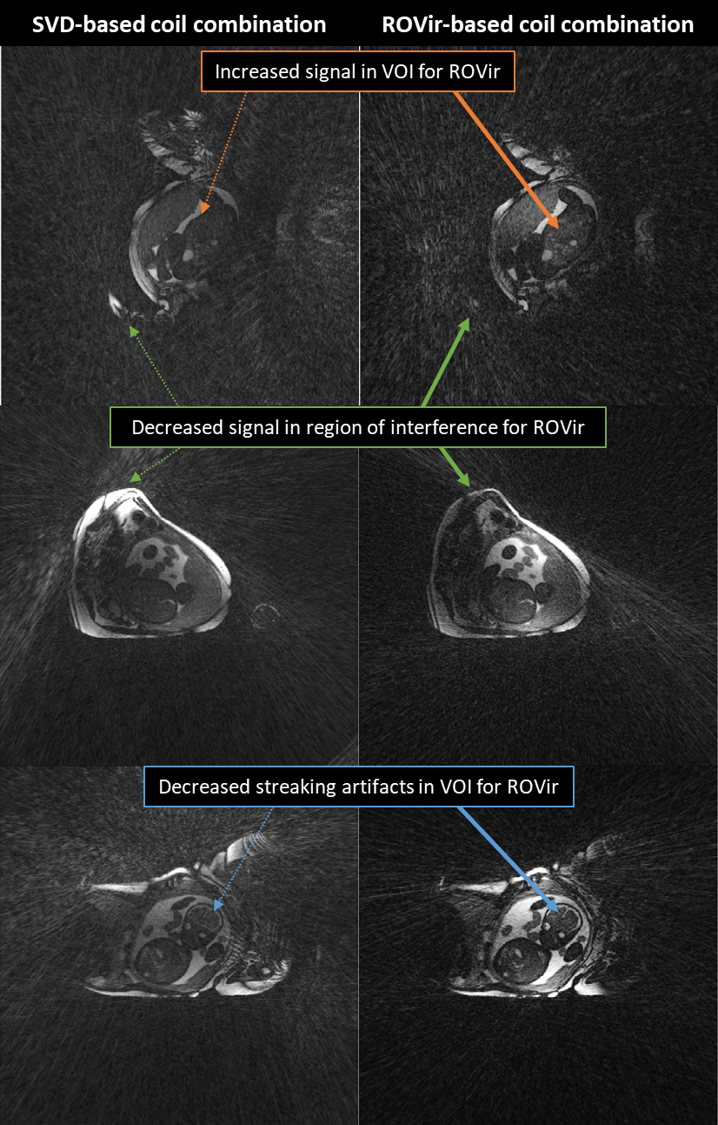
Figure 3. Multiplanar reformatted static images from a 3D SVD-based coil combination (left) and a 3D ROVir coil combination (right). It can be appreciated in the ROVir coil combination that the perceived image contrast is higher (orange circles). Additionally, the radial streaking artifacts in the volume of interest (VOI) (red circle) and the signal intensities in the region of interference (green circles) have been reduced.
Figure 4. Fetal cardiac function in a short-axis view. Multiplanar reformatted cine movies based on the SVD (left) and ROVir (right) coil combination-based reconstructions at 113 bpm (note that gif is limited in frames per second and fetal heart rate is not depicted properly). Whereas the SVD was reconstructed to 8 cardiac phases (temporal resolution 66 ms) due to computational load limitations the right-hand ROVir could be reconstructed to 16 cardiac phases (temporal resolution 33 ms) on the same system. The yellow arrow points at the right ventricle.
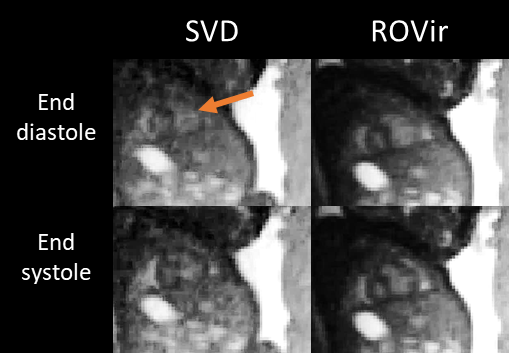
Figure 5. Short-axis reformatted images of the SVD (left) and ROVir (right) cine reconstruction, showing end-diastolic (top row) and end-systolic (bottom row) time frames. The orange arrow points at the right ventricle. In the ROVir reconstruction, note the increased visibility of intracardiac structures and thereby increased diagnostic quality.
DOI: https://doi.org/10.58530/2023/1246