1245
Real-time fetal cardiac MRI at 0.55T enables assessment of ventricular function and heart and great vessel anatomy1University of Southern California, Los Angeles, CA, United States, 2Children’s Hospital Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Fetal, Fetus
We demonstrate a real-time spiral balanced steady-state free precession (bSSFP) pulse sequence for fetal cardiac examinations on a 0.55T scanner. The real-time sequence provides easy adjustments of scan plan, automatic volumetric sweeping covering the whole heart, and flexible choice of reconstruction temporal resolution, without relying on any maternal breath-hold or cardiac gating. In 9 experiments involving 8 volunteers, we demonstrated high-temporal resolution (40ms/frame) real-time videos that capture fetal cardiac dynamics, and low-temporal resolution (320ms/frame) volumetric images that capture cardiac anatomy. This approach provides both functional and structural evaluations of the fetal heart.Introduction
Screening and assessment of fetal congenital heart disease is important for diagnosis, prognosis, parental counseling, and postnatal planning. Fetal cardiac MRI (CMR) is standard of care for static anatomic assessment, but to date, is in limited use for cardiac function evaluation. We believe fetal CMR can be useful when ultrasound imaging is suboptimal or limited.New whole-body 0.55T systems may provide superior fetal CMR image quality and patient experience, because of the larger bore sizes (70-80cm), lower acoustic noise, lower specific absorption rate, and reduced susceptibility. These advantages favor bSSFP pulse sequences with a high flip angle (FA), which can provide real-time images with high SNR and blood-myocardium contrast. These systems can also support underserved patient groups such as pregnant women with underlying obesity.
Fetal CMR has been demonstrated on 1.5T scanners1 but these studies require cardiac triggering from ultrasound or retrospective metric-optimized gating to reconstruct cine videos. In this study, we demonstrate the feasibility of real-time fetal CMR at 0.55T using a golden-angle spiral bSSFP pulse sequence, to evaluate fetal cardiac function and anatomy. Without relying on maternal breathhold or fetal cardiac gating, we collect real-time videos of the fetal heart and perform an automatic real-time sequential sweep sequence to cover the heart and great vessel anatomy.
Methods
Experiments: Imaging was performed on a whole-body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate)2. Imaging was performed using a real-time console (RTHawk, HeartVista Inc)3. Eight volunteers (maternal age 23-39 years, gestational age 25-38 weeks), including one with underlying obesity (BMI = 51) were enrolled after providing written informed consent, and under a protocol approved by our Institutional Review Board. One volunteer with healthy pregnancy was scanned twice at gestational age of 25 weeks and 34 weeks.Data Acquisition: Fetal CMR was performed using a real-time spiral bSSFP sequence with golden angle increment. Scan parameters were optimized in a couple of volunteers, by varying the FA (60o, 90o, 120o) and in-plane resolution (1.2 to 2.1 mm2). Other parameters include TE/TR=0.71/5.32ms; FOV=24cm; slice thickness=4mm. We acquired 10-20second recordings of key cardiac views including 4-chamber, short-axis, and long-axis. Additionally, we acquired volumes of 20-60mm thickness, by running an automated “real-time sweep”, where the imaging was performed for 2-5seconds per slice, then shifted by 1-4mm, until the entire volume was covered.
Reconstruction: Spatiotemporally constrained image reconstruction4 was preformed using the gradient impulse response function (GIRF) corrected spiral trajectory5. Reconstruction parameters were selected through a parameter sweep and qualitative evaluation by two board certified cardiologists. Images were reconstructed at a ~40ms/frame and ~320ms/frame temporal resolutions to visualize cardiac dynamics and cardiovascular anatomy, respectively. In addition, slice-to-volume registration (SVR)6 was performed on the 320ms/frame reconstructions.
Results
Figure 1 shows images acquired with different FAs and spatial resolutions. We found that FA of 90o or 120o and spatial resolution of 1.5 or 1.7 mm2 generally provided good image quality. We also note that SNR changes according to the coil placement and fetal position, thus the spatial resolution needs to be adjusted for different volunteers.Figure 2 shows representative 4-chamber scans from each experiment, which is the cardiac view that cardiologists found most useful and easy to track for cardiac motion and great vessel crossings. We show both the 40ms/frame video at one slice location and the 320ms/frame volumetric images at one time frame.
In all 9 experiments, real-time videos reconstructed at 40ms/frame were able to capture the cardiac motion in multiple cardiac views (4-chamber view is shown in Figure 2, others not shown). The four cardiac chambers and their motion were clearly depicted. The sequence also captured fetal arrhythmia in one subject as shown in Figure 3.
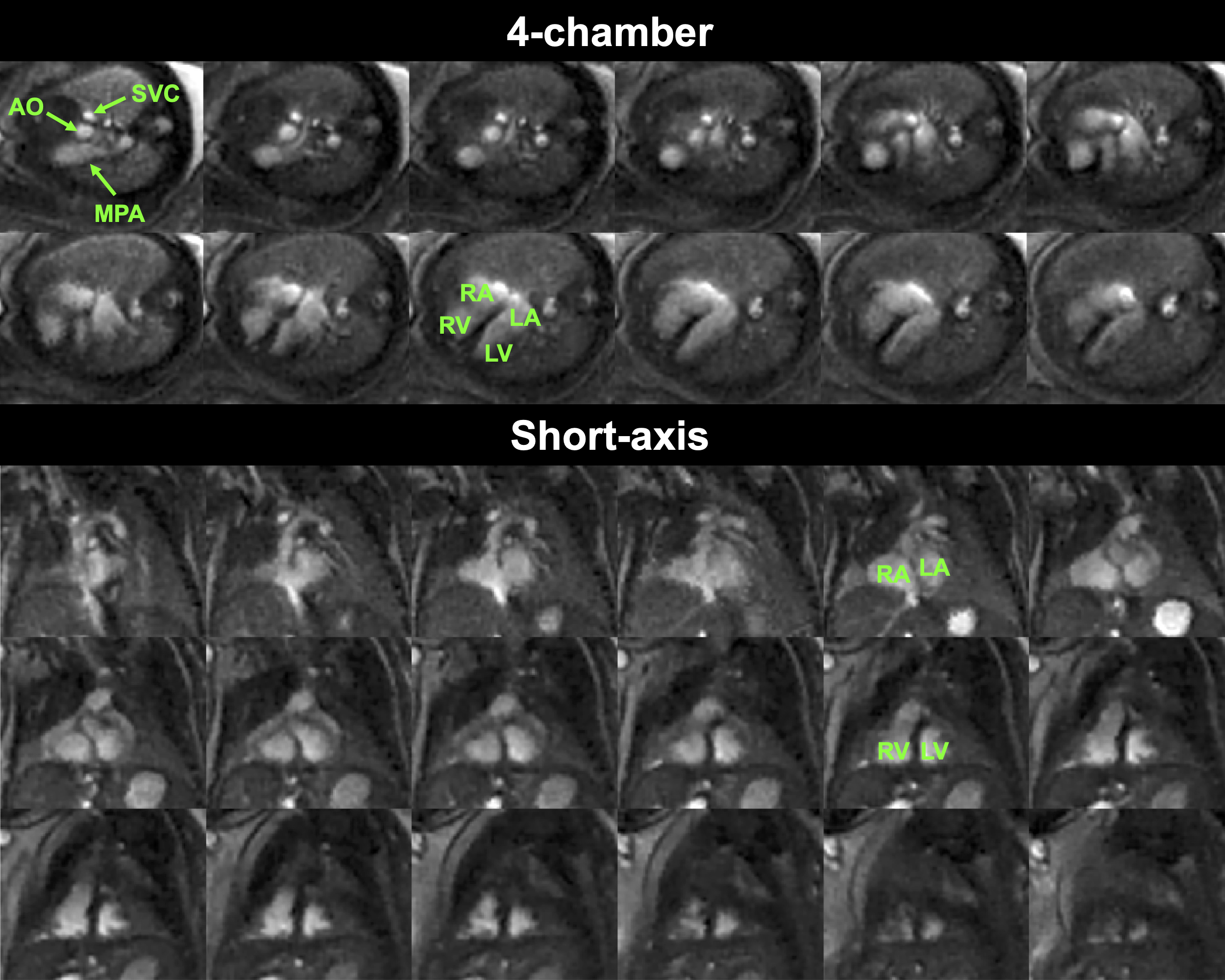
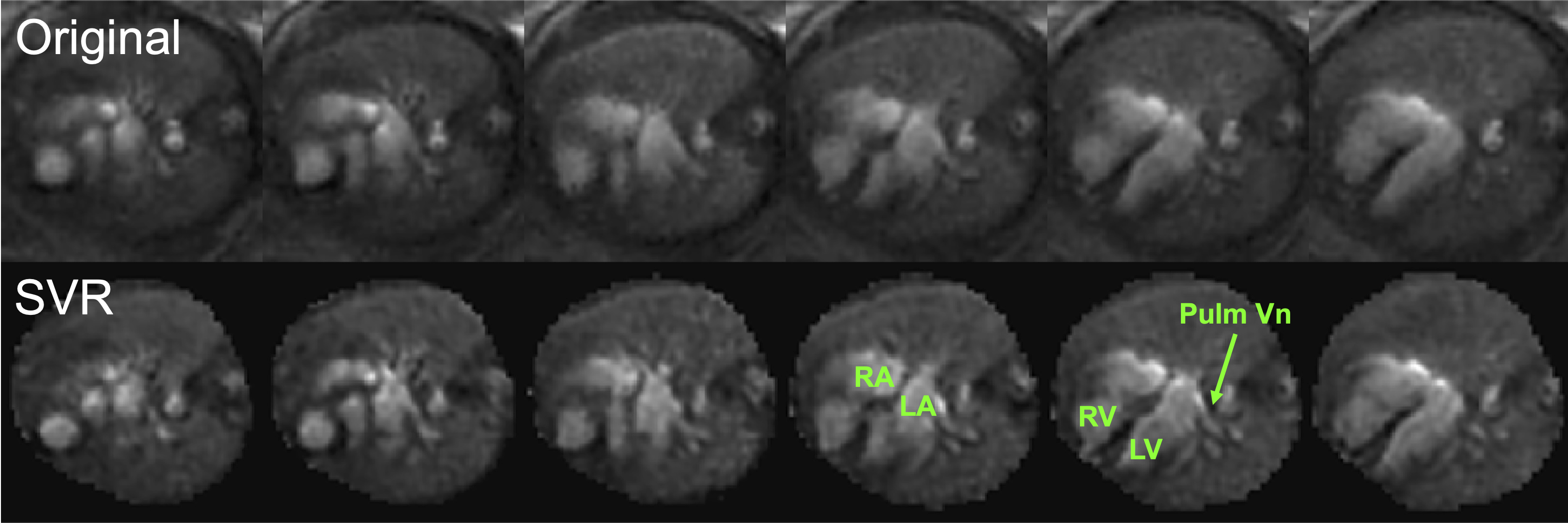
In the real-time volumetric sweep, reconstruction at 320ms/frame was adequate to assess normal cardiac anatomy and great artery relationships. Figure 4 shows the 4-chamber and short-axis sweeping from one representative subject. Specifically, we could see the great vessels crossing, no significant ventricular septal defects, and the pulmonary arteries arising properly. Figure 5 compares SVR results with the original images, where the palmary vine shows up clearly after SVR reconstruction. The added details are revealed which increases diagnosis confidence.
Discussions
We have demonstrated a real-time bSSFP spiral sequence for fetal heart evaluations at 0.55T. Real-time sequences have several advantages for fetal heart evaluation, such as no need for maternal breathholding or fetal cardiac gating. While performing MRI in fetuses, the biggest challenge is unpredicted motion. The real-time sequence can reduce the challenge by allowing a flexible scan plane adjustment attributed to the real-time image feedback.The sequence uses a golden-angle spiral trajectory, which allows a flexible retrospective reconstruction temporal resolution. With images reconstructed at 40ms/frame the cardiac dynamics are better captured, and reconstruction at 320ms/frame depicts the structure better. Moreover, the SVR reconstructions depicted atria, ventricles, systemic veins, and pulmonary veins very well. The aortic arch, ductal arches, and head/neck vessels remain areas for improvement, likely due to their small size making registration challenging.
Conclusion
We have demonstrated a real-time sequence at 0.55T for fetal CMR examination. The method can provide high-temporal resolution images for functional evaluation and volumetric images for structural evaluation.Acknowledgements
Grant support: National Science Foundation (#1828736), USC Provost’s Strategic Directions in Research Award, and USC Dean’s Pilot Grant from the Keck School of Medicine. Research support: Siemens Healthineers. We thank Skorn Ponrartana and Sophia X. Cui for collaboration, Mary Yung for research coordination, and the volunteers for their participation.References
1. Roy CW, van Amerom JFP, Marini D, Seed M, Macgowan CK. Fetal Cardiac MRI: A Review of Technical Advancements. Top Magn Reson Imaging. 2019;28(5):235-44.
2. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-93.
3. Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med Biol Soc. 2004;2004:1048-51.
4. Adluru G, McGann C, Speier P, Kholmovski EG, Shaaban A, Dibella EV. Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging. J Magn Reson Imaging. 2009;29(2):466-73.
5. Campbell-Washburn AE, Xue H, Lederman RJ, Faranesh AZ, Hansen MS. Real-time distortion correction of spiral and echo planar images using the gradient system impulse response function. Magn Reson Med. 2016;75(6):2278-85.
6. Kuklisova-Murgasova M, Quaghebeur G, Rutherford MA, Hajnal JV, Schnabel JA. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Med Image Anal. 2012;16(8):1550-64.
Figures