1202
Evaluation of Brachial Plexus Injuries in Infants with DTI and Tractography1National Magnetic Resonance Research Center (UMRAM), Bilkent University, Ankara, Turkey, 2Department of Radiology, Hacettepe University, Ankara, Turkey, 3Department of Radiology, University of California, Davis, Sacramento, CA, United States, 4Department of Anatomy, Ege University, Izmir, Turkey, 5Department of Orthopedics and Traumatology, Hacettepe University, Ankara, Turkey
Synopsis
Keywords: Nerves, Diffusion Tensor Imaging, Brachial plexus, peripheral nerve tractography
Neonatal brachial plexus injury (NBPI) is caused by traction on the neck during birth and presents with flaccid paralysis of the upper extremity. 10-20% of the cases result in neurological sequelae and require surgical intervention; the treatment decisions principally depend on the clinical assessments through the first six months of life. Early stratification of NBPI cases may lead to earlier intervention for severe injuries, better disease outcomes, and higher quality of life. Here, we investigated the use of DTI and tractography for infants with NBPI; our results suggest that this approach might be suitable as a diagnostic and prognostic tool.
Introduction
Neonatal brachial plexus injury (NBPI) is caused by traction on the neck during birth and presents with flaccid paralysis of the upper extremity1. NBPI is most commonly associated with shoulder dystocia and macrosomia; however, the majority of cases do not have an identifiable risk factor2. Estimates for the incidence of NBPI range from 0.5-4 per 1000 live births3, and most children with the condition will show almost complete neurological and functional recovery2. Even so, around 10-20% of the cases result in neurological sequelae and require surgical intervention4. The decision to pursue conservative treatment or perform microsurgery depends on serial clinical examinations through the first six months of age3. However, early intervention might benefit children with severe injuries, contributing to better outcomes and higher quality of life.While MRI methods are increasingly used in conjunction with clinical findings to assess the location, extent, and severity of brachial plexus injuries, there are discrepancies between imaging results, surgical findings, and histopathologic examinations1. Diffusion tensor imaging (DTI) can characterize tissue microstructure and provide information on axonal integrity in a non-invasive, in vivo manner5; consequently, it has been utilized to evaluate brachial plexus in healthy adults5 and those with traumatic injuries6. However, assessing NBPIs using DTI or tractography was not attempted in a pediatric cohort. This imaging modality might aid the early stratification of patients and guide treatment decisions and surgical planning in children with NBPI4.
In this study, we evaluated infants with brachial plexus palsy using DTI and subsequent tractography; the scans were acquired during natural sleep without anesthesia. We aimed to demonstrate the feasibility of DTI acquisitions for NBPI diagnosis and stratification of cases.
Methods
Twenty-two infants (11 boys, 11 girls; mean age: 13.6 weeks) with NBPI diagnosis were imaged during natural sleep with a 3-Tesla SIGNA Architect scanner (GE Healthcare, Illinois, USA) and a 32-channel head coil with an additional multi-purpose AIR coil.For anatomical imaging, coronal 2D STIR (TR/TE=5241/46.24 ms, TI=200 ms, NEX=2.5, flip angle=120º, echo train length=15, resolution=0.35 × 0.35 × 1.2 mm3, slice thickness= 1.2 mm, acquisition matrix=512 × 512 × 30) and 3D FIESTA (TR/TE=6.148/2.432 ms, NEX=1.5, flip angle=55º, resolution=0.156 ×0.156 ×0.49 mm3, slice thickness= 0.49 mm, matrix=1024 × 1024 × 160) sequences were employed. A coronal FOV Optimized & Constrained Undistorted Single-shot (FOCUS) sequence was used for diffusion-weighted MRI with the following acquisition parameters: TR/TE=3500/72 ms, NEX=2, flip angle=90º, resolution= 0.625 ×0.625 ×2.5 mm3, slice thickness= 2.5 mm, matrix=256 × 256 × 400; 24 diffusion directions, b value= 600 s/mm2. Scanning sessions were around 25 minutes in total for each child.
Acquired images were processed with AW Server 3.2 software (GE Healthcare), and tensor metrics (i.e., FA, ADC) were calculated. A neuroradiologist with ten years of experience manually placed ROIs on the brachial plexus trunks at affected levels. GraphPad Prism software (version 9; California, USA) was employed for the statistical comparisons of FA and ADC measurements. MRtrix3 software (www.mrtrix.org)7 was used for further processing and tractography. Preprocessing steps included denoising, correction for eddy currents, and bias correction; tractography was performed using the deterministic tracking algorithm.
Results and Discussion
In this study, we demonstrated the feasibility of diffusion MRI acquisitions in the neonatal period without the use of anesthesia. As the parents were instructed to keep the infants awake overnight and feed them immediately before the scans, infants could sleep undisturbedly with minimal movements for the duration of the imaging session.The statistical comparison of tensor metrics from the affected (ipsilateral) and contralateral trunks of the brachial plexus revealed significant differences in FA and ADC values (Figure 1). Ipsilateral trunks had significantly lower FA values reflecting a loss of orderly axonal microstructure. ADC values were also lower on the injured side, possibly associated with inflammatory infiltrates restricting free diffusion.
Among the infants with NBPI diagnosis, nine had both preganglionic and postganglionic damage, while the rest (n=13) only presented postganglionic findings. Avulsion injuries proximal to the dorsal root ganglion are categorized as ‘preganglionic’ while the ‘postganglionic’ type involves nerve root ruptures distal to the ganglion8; postganglionic injuries tend to show better prognosis due to higher rates of spontaneous recovery and surgical success. We found that preganglionic injuries were associated with significantly lower FA values on the affected side than the postganglionic type (Figure 2), which might point to worse disease outcomes.
In addition to the assessment of tensor metrics, we performed deterministic tractography on the DTI data (Figure 3). Conventional MR myelography and STIR sequences (Figure 4) are beneficial for the diagnosis and localization of lesions1. However, these methods may be inadequate as prognostic markers and have limited value for clinical decisions. We reason that diffusion MRI and subsequent use of tractography algorithms might aid the early stratification of cases for better treatment planning.
This study is currently ongoing with active recruitment of patients. Moreover, we plan to schedule additional MRI acquisitions for this cohort of children to see the evolution of injury and correlate our initial findings with the clinical outcome for each patient. Thus, it will enable us to define potential DTI biomarkers for NBPI prognosis.
Acknowledgements
No acknowledgement found.References
1. Gunes, A., Bulut, E., Uzumcugil, A. & Oguz, K. K. Brachial Plexus Ultrasound and MRI in Children with Brachial Plexus Birth Injury. AJNR Am J Neuroradiol 39, 1745–1750 (2018).
2. Zuarez-Easton, S., Zafran, N., Garmi, G., Nachum, Z. & Salim, R. Are there modifiable risk factors that may predict the occurrence of brachial plexus injury? Journal of perinatology : official journal of the California Perinatal Association 35, (2015).
3. Lin, J. S. & Samora, J. B. Brachial Plexus Birth Injuries. Orthop Clin North Am 53, 167–177 (2022).
4. Shen, P. Y. et al. Non-Sedated Rapid Volumetric Proton Density MRI Predicts Neonatal Brachial Plexus Birth Palsy Functional Outcome. J Neuroimaging 27, 248–254 (2017).
5. Wade, R. G. et al. Diffusion tensor imaging of the roots of the brachial plexus: a systematic review and meta-analysis of normative values. Clin Transl Imaging 8, 419–431 (2020).
6. Wade, R. G. et al. Diffusion Tensor Imaging for Diagnosing Root Avulsions in Traumatic Adult Brachial Plexus Injuries: A Proof-of-Concept Study. Front. Surg. 7, 19 (2020).
7. Tournier, J.-D. et al. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage 202, 116137 (2019).
8. Doshi, R. M. et al. Location of brachial plexus birth injury affects functional outcomes in a rat model. Journal of Orthopaedic Research 40, 1281–1292 (2022).
Figures
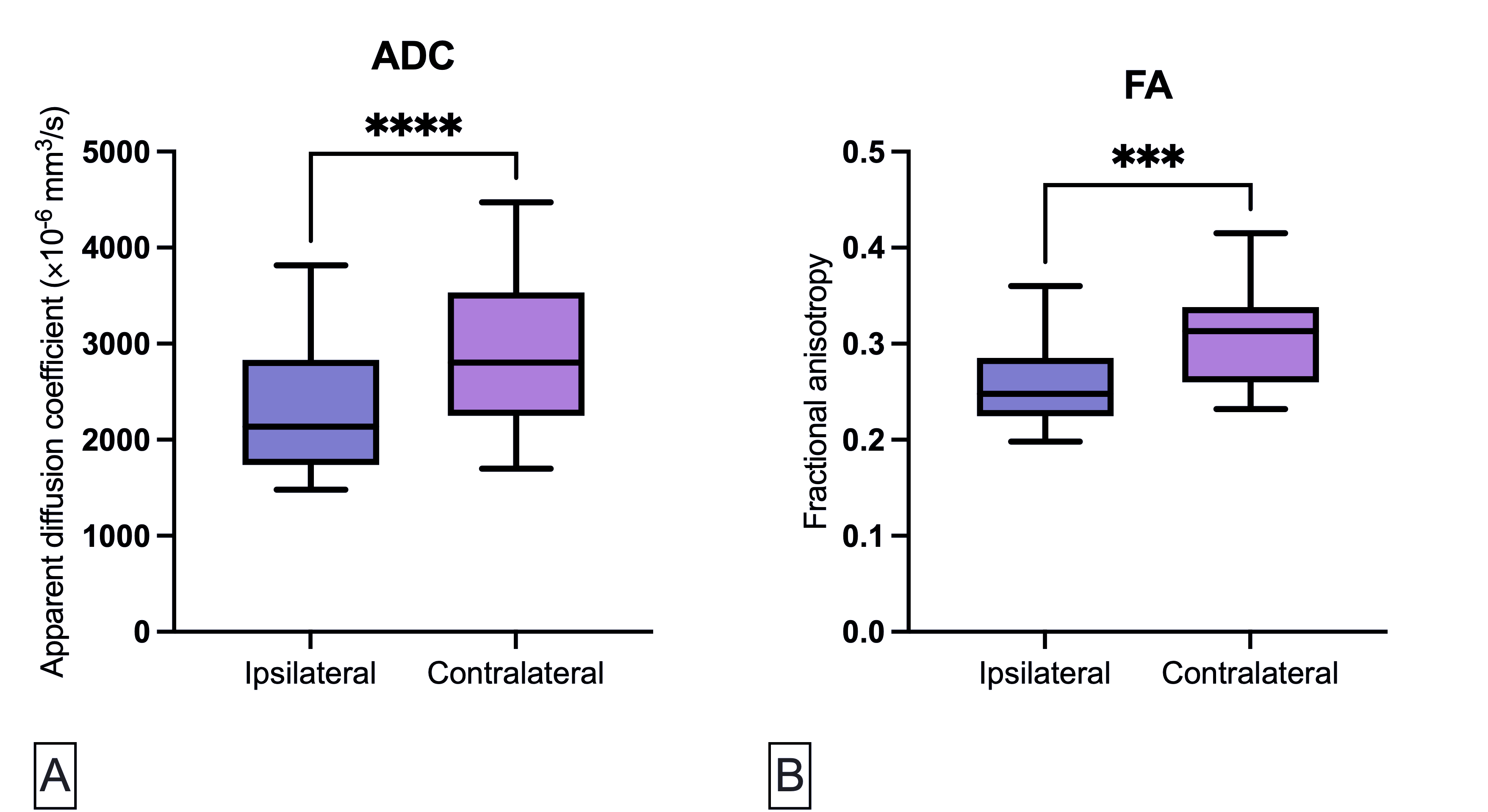
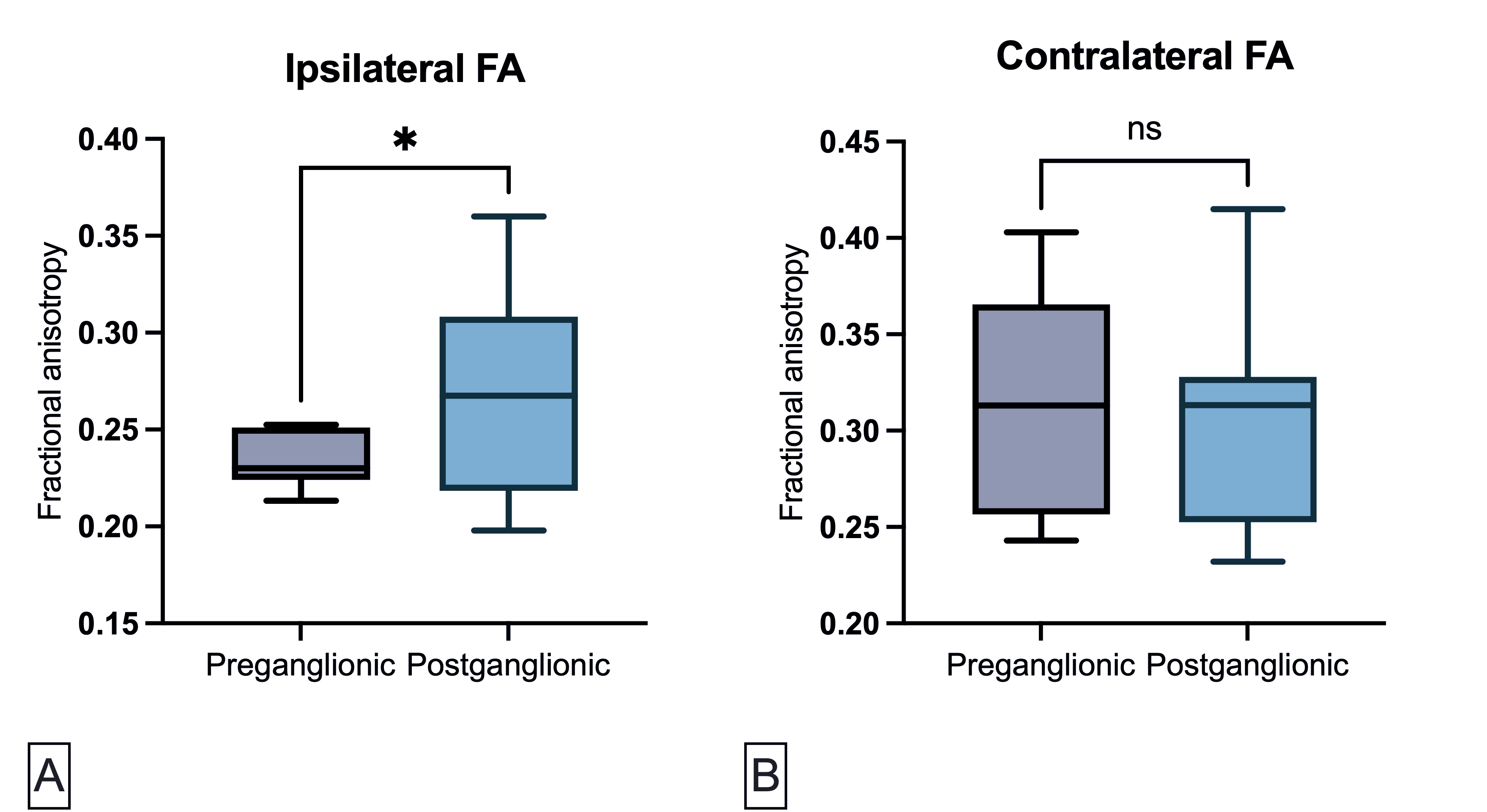
Figure 2. FA measurements from ipsilateral trunks at affected levels showed statistically significant differences between preganglionic and postganglionic injuries. A. Welch's t-test comparison of average ipsilateral FA for preganglionic and postganglionic injury types (p=0.0462). B. Welch's t-test comparison of average contralateral FA for preganglionic and postganglionic injury types (ns).
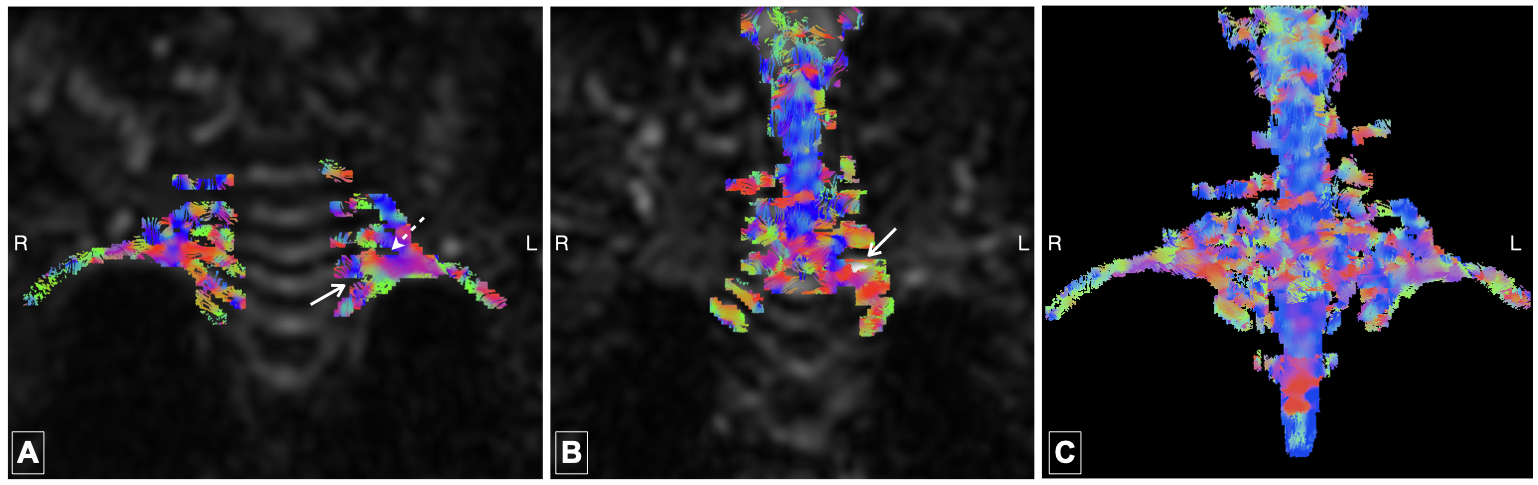
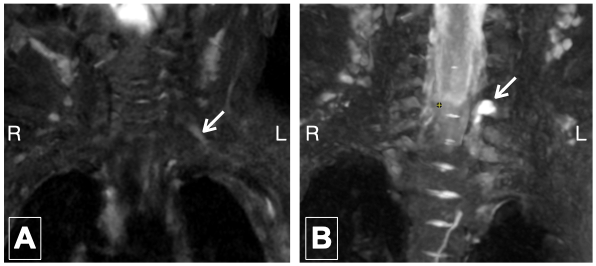
Figure 4. Conventional STIR images of the brachial plexus belonging to the same patient. A. Arrow shows hyperintense and dilated trunk. B. Pseudomeningocele at the level of avulsed C6 root.