1094
Simultaneous T1-T2 mapping, CINE and Multi-contrast Anatomical 3D whole-heart MRI1Millennium Institute for Intelligent Healthcare Engineering (iHEALTH), Santiago, Chile, 2Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 3King's College London, London, United Kingdom, 4Electrical Engineering Department, Pontificia Universidad Católica de Chile, Santiago, Chile, Santiago, Chile, 5ShanghaiTech University, Shanghai, China
Synopsis
Keywords: Quantitative Imaging, Myocardium, Motion Correction
Cardiac T1-T2 mapping provides information about focal and diffuse fibrosis and inflammation of the myocardium. A recently proposed free-running 3D mapping technique allows time efficient and simultaneous whole-heart T1-T2 mapping within a single scan, with retrospective respiratory motion correction. However, this approach loses the information about the temporal contrast evolution and does not reconstruct multi-contrast 3D whole-heart images, which may carry useful clinical information in patients with myocardial infarction and, acute and subacute thrombus. In this work, we propose to extend this approach to enable joint T1-T2 mapping, CINE, and multi-contrast 3D whole-heart imaging from a single free-running scan.
Introduction
Quantitative T1 and T2 mapping allows myocardial tissue characterization, which is useful for detection of focal and diffuse fibrosis (T1) and inflammation (T2). A recently proposed framework for joint 3D T1 -T2 mapping and CINE imaging with whole-heart coverage allows simultaneous quantification of left ventricular (LV) function and myocardial tissue characterization in ~11 minutes 1. The method consists of a free-running self-navigated spoiled gradient echo sequence with a 3D radial trajectory with golden-angle step, motion corrected high-dimensionality patch-based low-rank reconstruction (HD-PROST) 2 and dictionary matching. However, this approach loses the information about the temporal contrast evolution and does not reconstruct multi-contrast 3D whole-heart images, which may carry useful clinical information, especially in patients with myocardial infarction (late gadolinium enhancement) and those with acute and subacute thrombus (T1 weighted pre-contrast images). In this work, we propose to extend this approach for joint T1-T2 mapping, CINE, and multi-contrast 3D whole-heart imaging from a single free-running scan.Methods
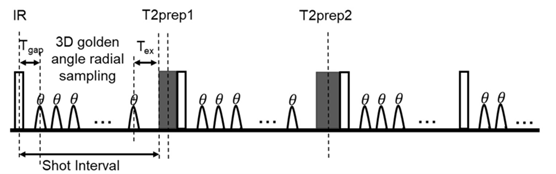
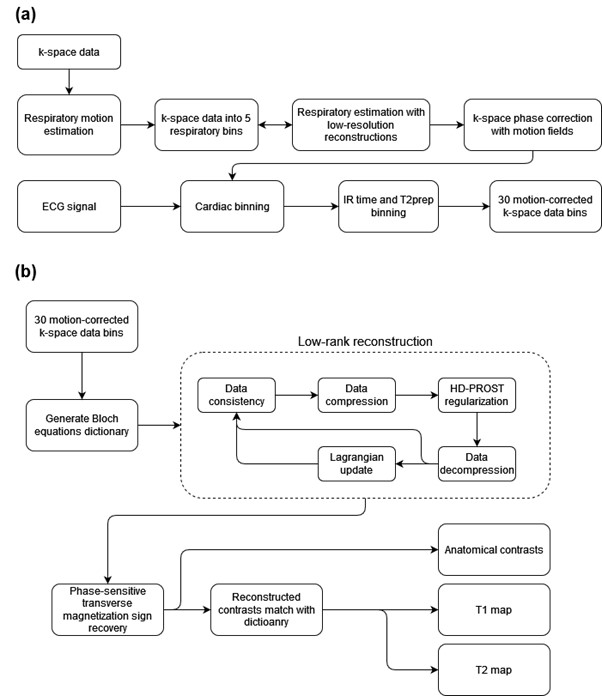
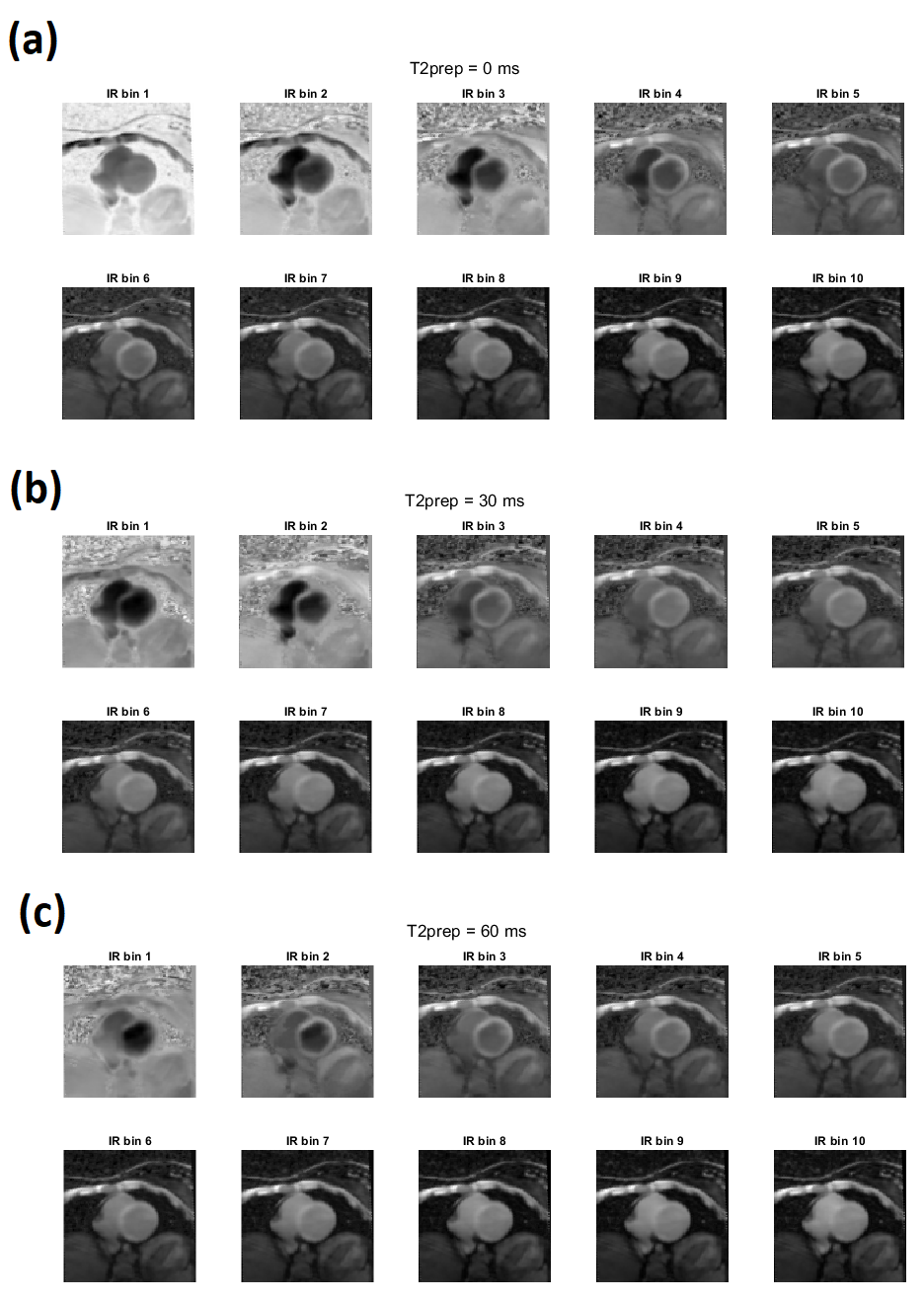
The free-running joint T1-T2 mapping and CINE sequence 1 consists of water selective spoiled gradient echo readout with 3D golden-angle radial trajectory. Each shot interval is preceded by an inversion recovery (IR) pulse with T2 preparation pulses (T2-prep) with varying echo times of 0 ms (no T2-prep), 30ms and 60ms (Figure 1). This acquisition pattern is repeated several times. Respiratory motion is estimated from the center of k-space 3 and radial spokes are sorted into 5 different respiratory bins. Low resolution images are reconstructed from each bin, and translational motion fields are estimated for each bin with respect to a reference bin. Respiratory motion correction is then performed by applying the estimated motion as phase shift to the k-space data.Retrospective cardiac binning was achieved via ECG synchronization, allowing the reconstruction of several cardiac phases independently. For each cardiac phase (120 ms), k-space data was binned into 10 different IR times for each T2-prep, resulting in a total of 30 contrasts to be reconstructed (Figure 2.a). A Bloch equation dictionary was generated for different T1, T2 and B1 field inhomogeneities. The reconstruction of the 30 contrasts was performed using L2 norm data consistency for all contrasts and high-dimensional patch-based low-rank regularization (HD-PROST) 2 on dictionary-based compressed images. Thus, the contrast images were recovered by minimizing the following Lagrangian with the Alternating Direction Methods of Multipliers (ADMM):
$$L(x,T, Y)=∥Ex−Wk∥^2_2+λ∑_p∥T_p∥_∗+μ/2∑_p∥T_p−P_p(U_r^Tx)−P_p(U_r^TY)∥^2_F$$
Where $$$x∈C^{NL×1}$$$ is the multi-contrast complex image with $$$N$$$ voxels and $$$L$$$ different contrasts, $$$k∈C^{KN_c×1}$$$ is the k-space acquired data with $$$K$$$ samples and $$$N_c$$$ coils, $$$W$$$ is a k-space density compensation matrix, $$$E=WFS$$$ is the encoding operator with $$$S∈C^{NN_cL×NL}$$$ being the estimated sensitivity maps and $$$F∈C^{KN_c×NN_cL}$$$ the non-uniform Fourier transform. $$$T_p$$$ is the HD-PROST tensor formed with similar patches centered at voxel $$$p$$$, $$$P_p(∙)$$$ is the patch-selecting operator centred at voxel $$$p$$$, $$$U_r∈R^{NL×Nr}$$$ is the compressed dictionary with the highest $$$r$$$ singular values, $$$Y$$$ are the augmented Lagrange multipliers, $$$λ$$$ and $$$μ$$$ are regularization parameters, and $$$∥∙∥_*$$$, $$$∥∙∥_F$$$ are the nuclear and Frobenius norms.
In each iteration of ADMM, $$$L=30$$$ different contrasts were reconstructed in the data consistency step and were compressed to $$$r=5$$$ singular images 4 (with operator $$$U_r$$$) for the HD-PROST regularization, to save memory and processing power. To use the output of the denoising in the next iteration, the singular images were decompressed by minimizing $$$∥U_rx−x_c∥^2_2$$$, where $$$x_c$$$ are the compressed singular contrasts. A phase-sensitive dictionary matching was used to obtain T1 and T2 maps. Transverse magnetization sign was recovered for each complex-image $$$x$$$ 5 and a real image $$$x_s$$$ was obtained. A diagram of the reconstruction is shown in Figure 2.b.
The proposed approach was evaluated in healthy subjects. Acquisitions were performed on a 3T scanner (Philips, Ingenia) with a 23-channel cardiac coil. Main acquisition parameters include: FOV= 200 mm, isotropic resolution = 2 mm, flip angle = 6°, TR/TE=10.3 ms/4.6 ms, acquisition pattern repeated 300 times with 195 readouts in each shot, IR repetition time = 2200 ms, total scan time ~11 min. All images were reconstructed with Matlab (R2021a).
Results and discussion
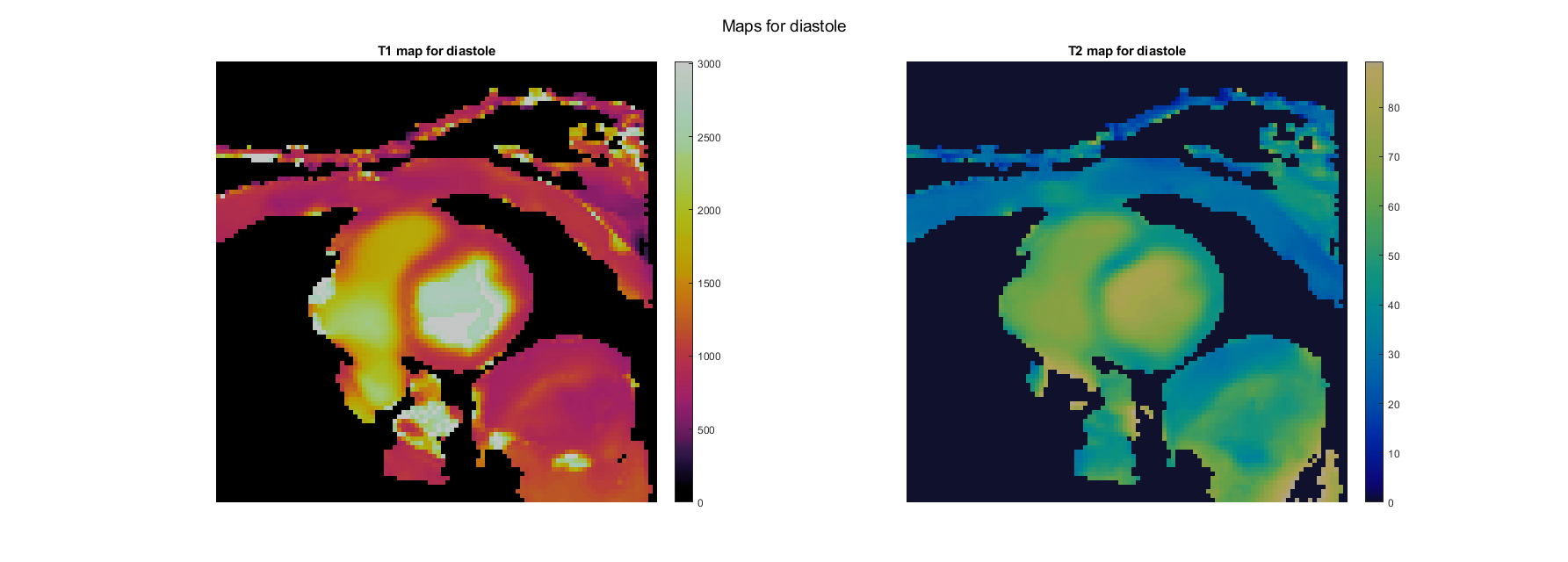
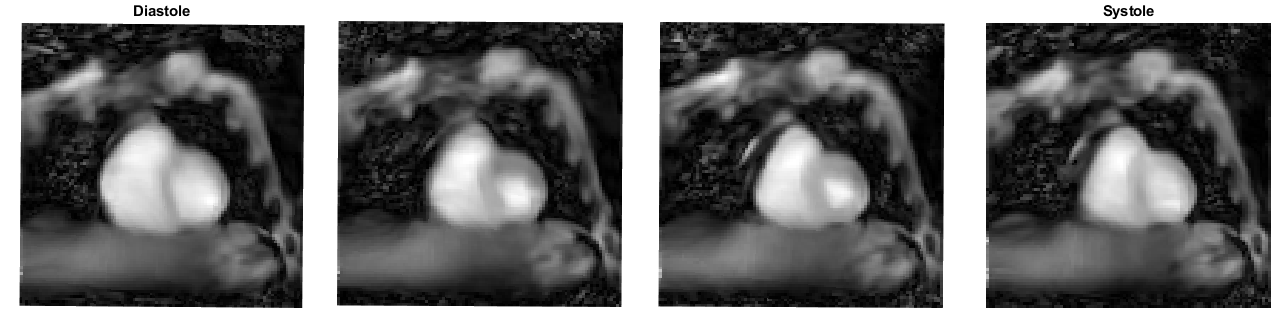
Proposed joint T1 and T2 maps for a representative healthy subject are shown in Figure 3 in diastole. Septum T1 and T2 values were measured to be $$$1102±93$$$ and $$$49±6$$$ ms, which are in agreement with literature values for healthy myocardium at 3T. CINE contrast images are shown in Figure 4. Results for all contrasts are shown in Figure 5. The method was able to recover good quality contrast images from heavily undersampled data, as each contrast has an undersampling factor of 30 on top of the undersampling inherent to the original method.Conclusion
In this study, we propose to extend a previous T1-T2 mapping sequence with 3D full-heart coverage and simultaneous CINE reconstruction, by adding the reconstruction of additional anatomical contrast images for all 30 combinations of inversion recovery times and T2-prep echo times. Future work will consist in further improving the quality of the contrast images and to demonstrate its clinical usefulness in patients with cardiovascular disease.Acknowledgements
This work was funded by ANID – Millennium Science Initiative Program – ICN2021_004.
References
1. Qi H, Bustin A, Cruz G, Jaubert O, Chen H, Botnar RM, Prieto C. Free-running simultaneous myocardial T1/T2 mapping and cine imaging with 3D whole-heart coverage and isotropic spatial resolution. Magn Reson Imaging. 2019 Nov; 63:159-169.
2. Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med. 2019 Jun;81(6):3705-3719.
3. Qi, H, Jaubert, O, Bustin, A, et al. Free-running 3D whole heart myocardial T1 mapping with isotropic spatial resolution. Magn Reson Med. 2019; 82: 1331– 1342.
4. McGivney DF, Pierre E, Ma D, Jiang Y, Saybasili H, Gulani V, Griswold MA. SVD compression for magnetic resonance fingerprinting in the time domain. IEEE Trans Med Imaging. 2014 Dec;33(12):2311-22.
5. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002 Feb;47(2):372-83
Figures