1088
Evaluation of hemodynamic parameters for prediction of aortic growth in patients with chronic Stanford type B aortic dissection using 4D flow MRI.1Diagnostic Radiology, Tohoku University Hospital, Sendai, Japan, 2Radiology, Tohoku University Hospital, Sendai, Japan
Synopsis
Keywords: Flow, Vessels, Aortic Dissection
Uncomplicated type B aortic dissection (AD) has a poor long-term outcome and further optimization of predictors for aortic expansion is required. Seventeen patients with chronic type B AD who underwent 4D flow MRI were included and divided into two groups based on the aortic growth rate. The morphological and hemodynamic parameters in each group were retrospectively analyzed. The forward flow and volume in true lumen and ratio of these parameters at entry and false lumen to true lumen were significantly higher in the fast growth-rate group than in the slow one; no morphological parameters showed a significant difference.
Introduction
Uncomplicated Stanford type B aortic dissection (AD) can be managed with medical treatment in the acute phase, but its long-term outcome is sobering because of aneurysmal expansion and a 30% cumulative mortality at 5 years 1. Recent reports have indicated that thoracic endovascular aortic repair (TEVAR) in addition to optimal medical treatment is associated with improved survival and delayed disease progression 2. However, such invasive pre-emptive treatment should be performed for those whose aorta is expected to be enlarged. Therefore, predictors of aortic expansion are a major area of interest in the management of AD. Although some morphological parameters such as aortic diameter and entry size have been reported as predictors, inconsistency in the results of morphologic features is left unsolved. Four-dimensional flow magnetic resonance imaging (4D flow MRI) allows the assessment of the three-directional, time-resolved blood flow, providing various hemodynamic parameters such as flow velocity, jet angle, vorticity, helicity, tortuosity, wall share stress, energy loss, and turbulent kinetic energy. In AD, blood flow in the false lumen (FL) has been reported to show complex, abnormal, and nonlaminar flow patterns and frequent occurrence of systolic retrograde flow 3. This complex blood flow in FL also has been reported a significant correlation with the rate of FL expansion 4–6. The hemodynamic parameters in AD can provide additional qualitative and quantitative values in the current morphological assessment that may play a role in establishing treatment strategy as an emerging biomarker.We retrospectively reviewed patients with chronic Stanford type B AD who underwent 4D flow MRI and analyzed the relationship between the aortic growth rate and hemodynamic parameters.
Methods
A total of 17 patients with chronic type B AD, who underwent 4D flow MRI from October 2015 to March 2021 (mean age, 66 years, male, 13) were included in the study. All patients were imaged with a 3T whole-body MR scanner (MAGNETOM Trio Tim or MAGNETOM Vida; Siemens Healthineers, Erlangen, Germany). Scanning protocols included time-resolved MR angiography with gadolinium-based contrast agent and 4D flow MRI. Acquisition parameters are shown in figure 1. From 4D flow MRI, the average and peak flow (ml/s), forward, reverse, and net flow volume (ml), and regurgitation fraction (%) at entry, TL, and FL were evaluated (Figure 2). The ratio of average and peak flow, forward, reverse, and net flow volume at entry and FL to TL were calculated. The diameters of the descending aorta and entry, and the recent growth rate in diameter (mm/year) were evaluated from serial contrast-enhanced CT angiography images. The patients were divided into two groups based on the growth rate: slow or fast growth-rate groups (SGR and FGR groups). The hemodynamic parameters were compared between the two groups using Wilcoxon signed-rank test with JMP® Pro version 16.0.0. P < 0.05 was considered statistically significant.Results
The growth rate in SGR and FGR groups were 0.8 (0.2-1.4) and 3.0 (2.8-7.6) mm per year, respectively. The diameter of the descending aorta and entry showed no significant difference between the two groups (SGR vs. FGR: 52 [44-58] mm and 56 [53-57] mm, and 15.8 [4.4-21.7] vs. 18.8 [12.0-34.1], respectively). Among flow parameters, the average net flow, peak flow, forward flow volume, and net forward flow volume in TL were significantly higher in the SGR group than in the FGR group (figure 3,4). The ratio of peak flow and forward flow volume at entry and TL were significantly higher in the FGR group than in the SGR group (figure 3,4). The ratio of average net flow, peak flow, and net forward flow volume at FL to TL were significantly higher in the FGR group than in the SGR group. Other hemodynamic parameters in the entry and FL were not significantly different between the two groups.Discussion
Some reports showed that flow velocity, forward flow volume, and regurgitation fraction at entry or FL correlated with the aortic growth rate in AD 4–6. In this study, the fast aortic growth-rate group showed significantly lower flow velocity or volume in TL, nevertheless, morphological parameters showed no significant difference between the two groups. Flow velocity and volume in TL and FL usually depend on cardiac function and blood volume. But we showed FGR group had a higher ratio of these parameters at entry and FL to TL than the slow growth-rate group, indicating this ratio can become a novel biomarker for the prediction of aortic expansion. Some past reports used 2D phase-contrast (PC) images for assessment of blood flow, but 4D flow MRI allows visual assessment of hemodynamics and retrospective flow analysis in any direction within the field of view; especially, the entry is difficult to set appropriate planes during a scan with 2D PC. In some cases, the accelerated flow at entry caused wraparound artifacts, which required correction. Further study with multi-VENC acquisition and a larger sample size is warranted to confirm our results.Conclusion
Beyond the morphologic parameters, flow velocity and volume in TL and the ratio of these parameters at entry and FL to TL can be predictive factors for aortic growth rate in patients with chronic Stanford type B aortic dissection.Acknowledgements
The authors thank Mayuki Tawara for helping with the data analysis. We also thank Yoshiaki Komori, Daniel Giese, and Ning Jin for providing a suitable scan protocol.
References
1. Tsai TT, Fattori R, Trimarchi S, et al. Long-Term Survival in Patients Presenting With Type B Acute Aortic Dissection. Circulation. 2006;114(21):2226-2231.
2. Nienaber CA, Kische S, Rousseau H, et al. Endovascular Repair of Type B Aortic Dissection. Circ Cardiovasc Interv. 2013;6(4):407-416.
3. Takahashi K, Sekine T, Ando T, Ishii Y, Kumita S. Utility of 4D Flow MRI in Thoracic Aortic Diseases: A Literature Review of Clinical Applications and Current Evidence. Magn Reson Med Sci. 2022 Mar 1;21(2):327-339.
4. Burris NS, Nordsletten DA, Sotelo JA, et al. False lumen ejection fraction predicts growth in type B aortic dissection: preliminary results. Eur J Cardiothorac Surg. 2020;57(5):896-903.
5. Clough RE, Waltham M, Giese D, Taylor PR, Schaeffter T. A new imaging method for assessment of aortic dissection using four-dimensional phase contrast magnetic resonance imaging. J Vasc Surg. 2012;55(4):914-923.
6. Arturo Evangelista MD, Victor Pineda MD, Andrea Guala P, et al. False Lumen Flow Assessment by Magnetic Resonance Imaging and Long-Term Outcomes in Uncomplicated Aortic Dissection. J Am Coll Cardiol. 2022 Jun 21;79(24):2415-2427.
Figures
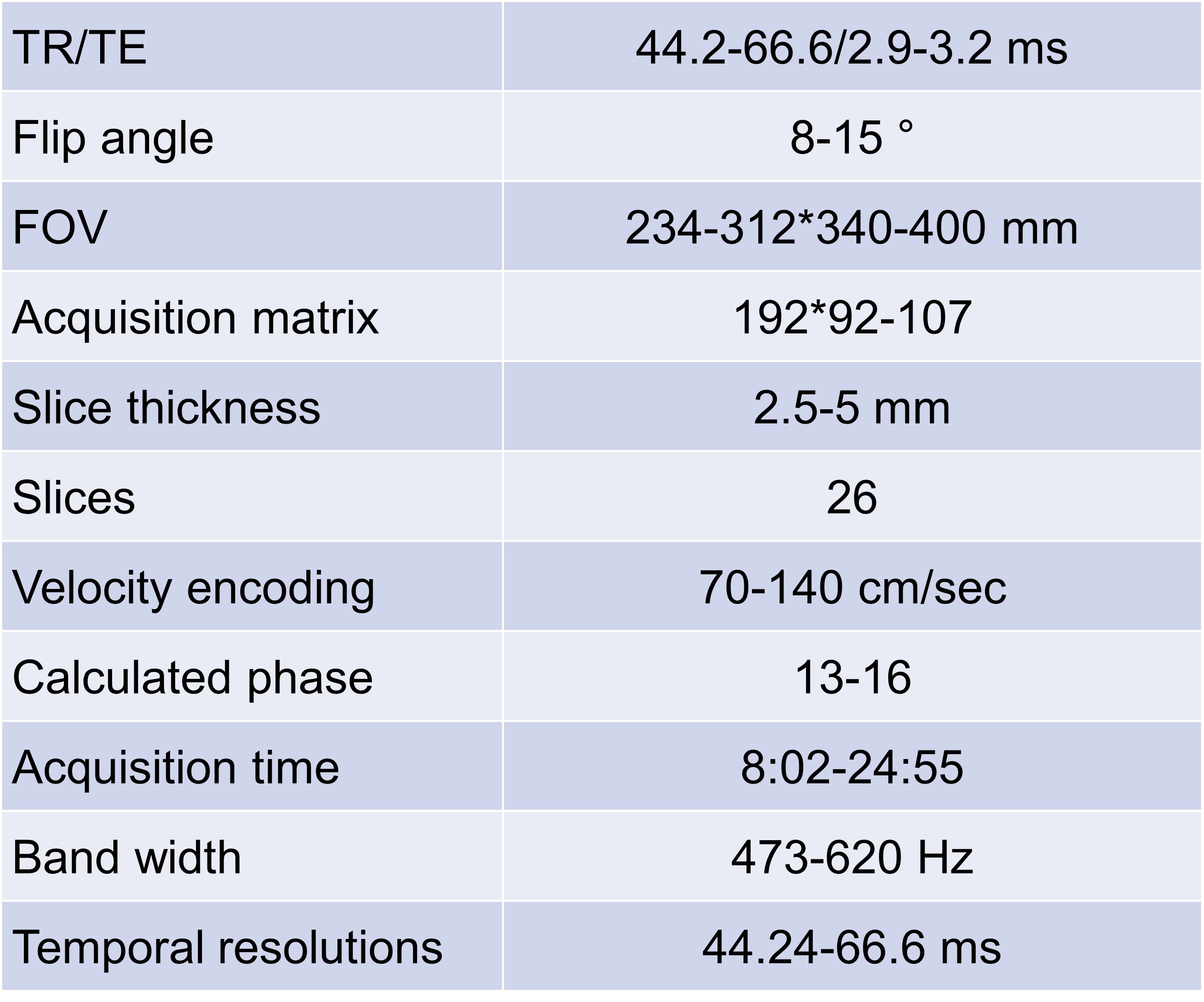
Acquisition parameters for 4D flow MRI.
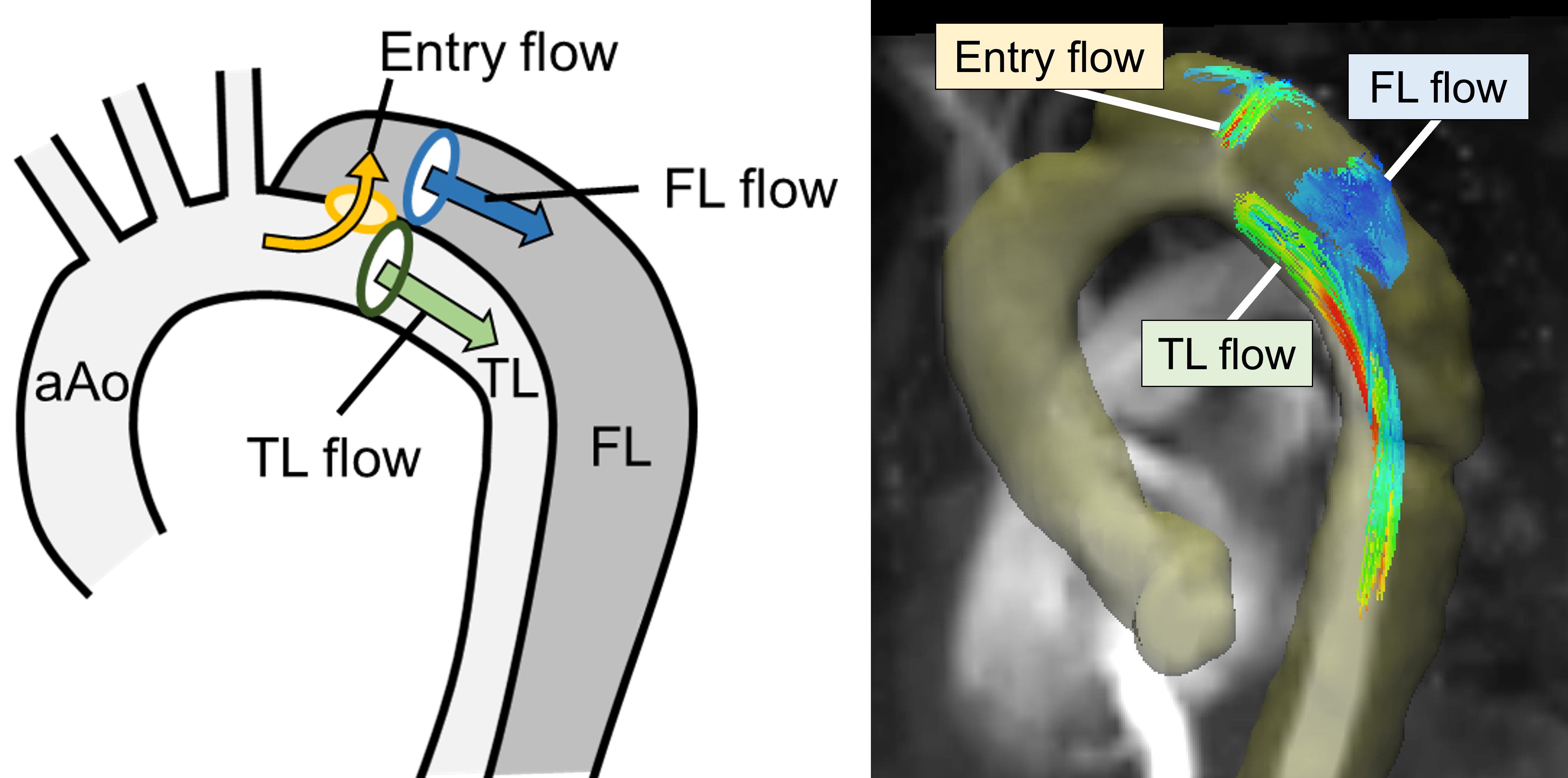
Location to obtain each flow parameter in aortic dissection. The entry flow was acquired at the entry in descending aorta. The flow at the true lumen was acquired at true lumen immediately after the entry. Flow at false lumen was acquired at false lumen with maximum diameters. aAo = ascending aorta, TL = true lumen, FL = false lumen, SGR = slow growth rate group, FGR = fast growth rate group
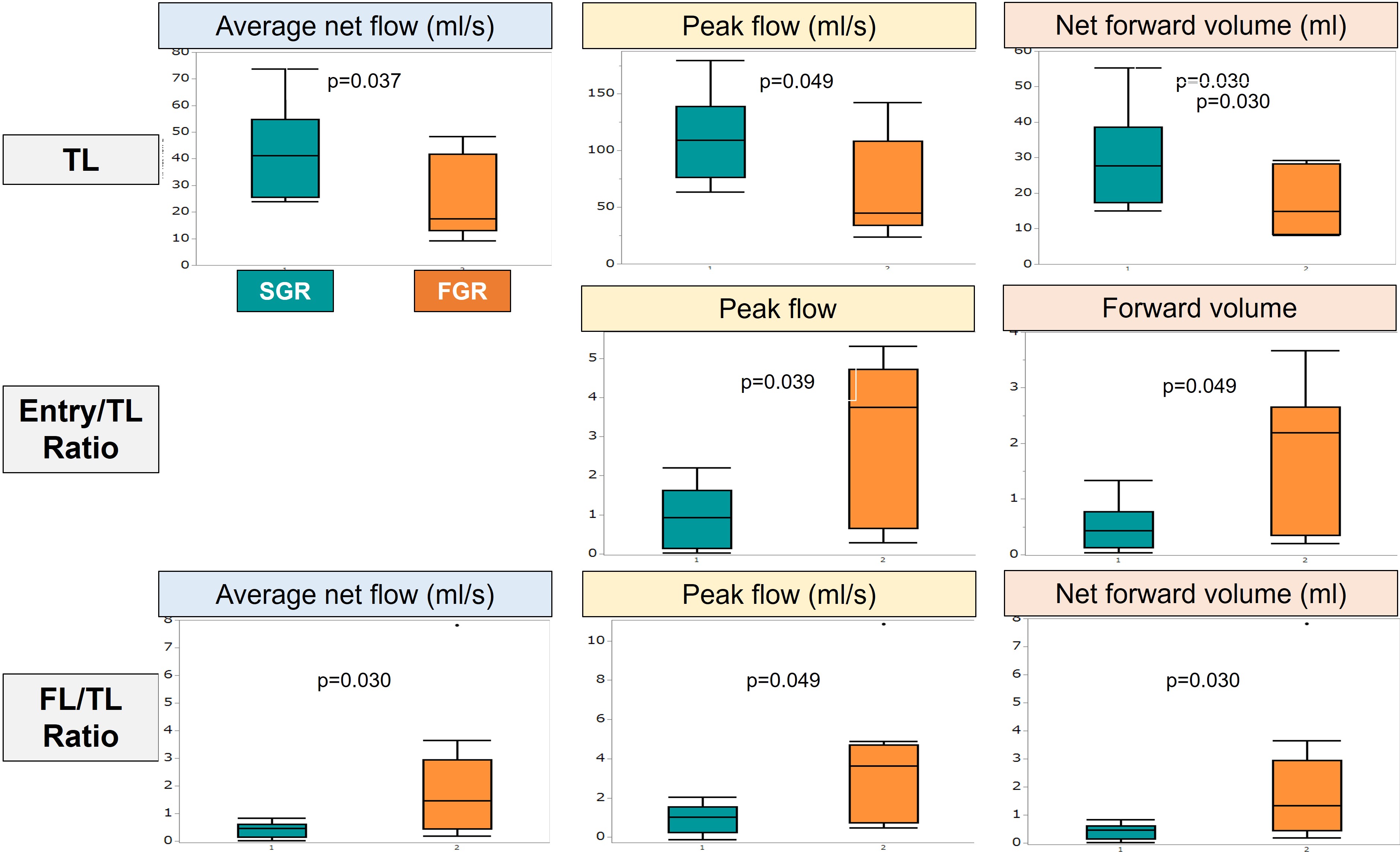
Results of hemodynamic evaluation between SGR and FGR groups. Average net flow, peak flow, and net forward volume at TL were significantly lower in the FGR group. The ratio of peak flow and forward flow volume at the entry to TL was significantly higher in the FGR group. The ratio of average net flow, peak flow, and net forward flow volume at FL to TL was significantly higher in the FGR group. TL = true lumen, FL = false lumen, SGR = slow growth rate group, FGR = fast growth rate group
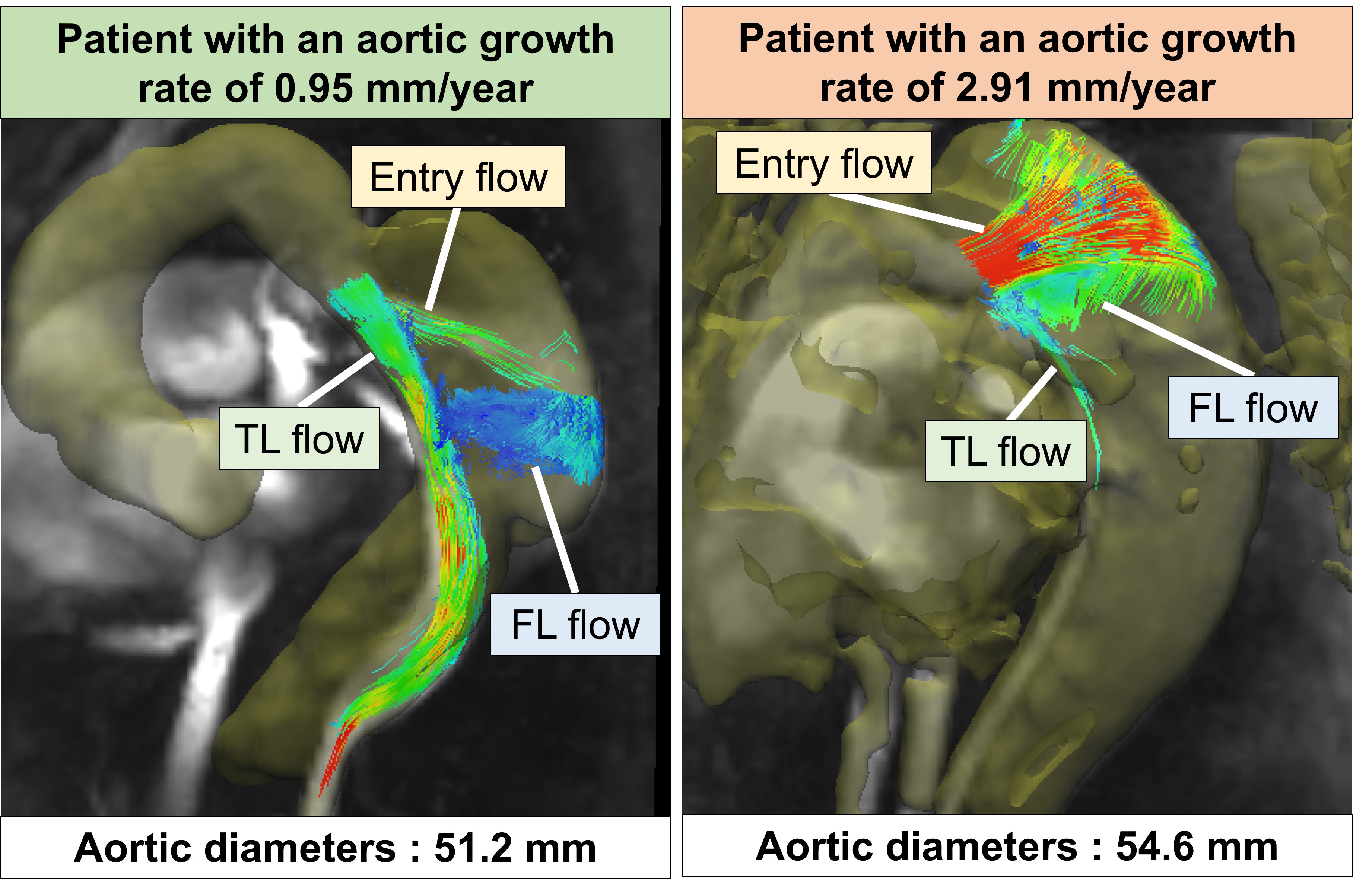
Representative cases in each SGR and FGR group. While a patient with an aortic growth rate of 0.95 mm/year showed higher flow at TL than at the entry and FL, a patient with an aortic growth rate of 2.91 mm/year showed lower flow at TL than at the entry and FL. TL = true lumen, FL = false lumen