1084
Ferumoxytol Dose Optimization for 3D Whole-Heart Congenital Heart Disease Imaging1Cardiac MRI, Children's Medical Center, UT Southwestern, Dallas, TX, United States
Synopsis
Keywords: Heart, Cardiovascular, image quality, ferumoxytol, contrast
With its concomitant ability to shorten the T1 relaxivity of blood and long intravascular half-life, ferumoxytol has become a popular “blood pool” contrast agent. The optimum contrast dose is not known. Reducing the ferumoxytol dose to 2 mg/kg is an efficient method to optimize the image quality, diagnostic performance, and achieve reduction in Gibbs’ truncation artefact.Introduction
Ferumoxytol is an ultrasmall superparamagnetic iron oxide (USPIO) approved for intravenous treatment of iron-deficiency anemia. Due to its large size, ferumoxytol remains in the intravascular space for a long time (half-life 14 hours). Its concomitant ability to shorten the T1 relaxivity of blood, has resulted in its popularity as an intravascular “blood pool” contrast agent.1 The optimum dose is not known, but commonly used doses vary between 3-5 mg/kg (IV) for all age groups given over 15 minutes.2 However, we observed that T1-weighted three-dimensional (3D) Whole-Heart Imaging using the standard dose resulted in Gibbs’ truncation artefact due to the high signal in the blood pool. In this study we compared the image quality and diagnostic performance among patients receiving reduced ferumoxytol dose of 2 mg/kg, to a group of patients receiving a standard 3 mg/kg dose.Methods
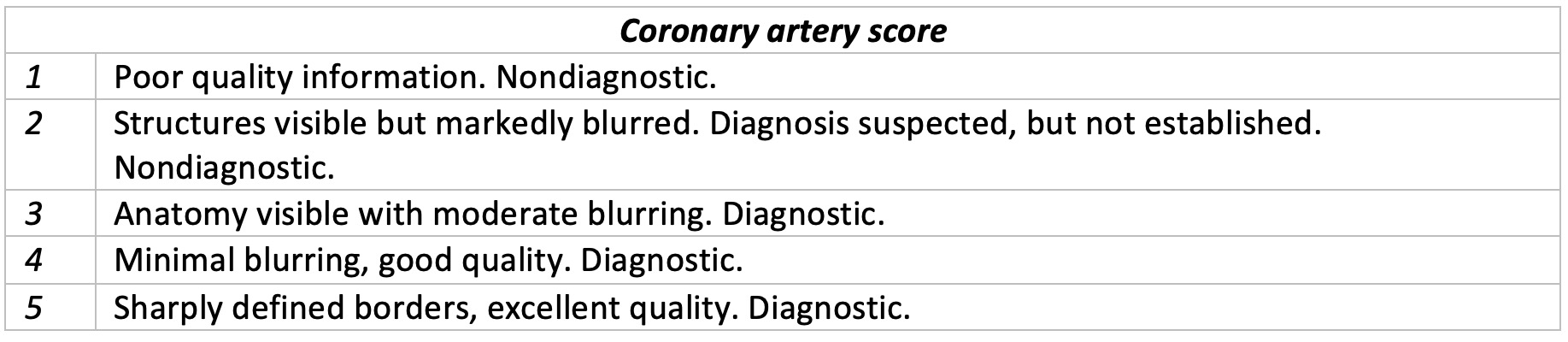
Twenty-two patients with complex congenital heart disease were included in the study. Subjects were divided into two groups based on the ferumoxytol dose received (ferumoxytol 2 mg/kg vs. ferumoxytol 3 mg/kg). The patients were matched by age, gender, weight, and heart rate (Table 1). Inversion times, presence of Gibbs’ truncation artefact, image quality, and diagnostic performance were compared among these groups using inversion-recovery (IR) 3D SSFP sequence with respiratory navigator and EKG triggering. Sequence parameters included (FOV 330mm x 330mm; Acquired resolution 1.4 to 1.8 mm3; Compressed Sense Factor 3.5; TE =1.73ms; TR=3.6ms). The optimum inversion time (TI) was chosen using a Look-Locker TI scout. The cardiac rest period (end-systole or mid-diastole) was chosen according to the clinical question or according to which period was longer. Quantitative image quality was assessed by comparing contrast-to-noise ratios (CNR). Qualitative image assessment was conducted by using the five-point scoring scale.3,4 The coronary artery images were scored based on the presence of artefacts, qualitative sharpness, and diagnostic confidence (Table 2). Diagnostic performance was measured through the ability of each imaging method to reach complete diagnosis including the identification of all morphological segments, aortic arch branching, and coronary artery anatomy.Results
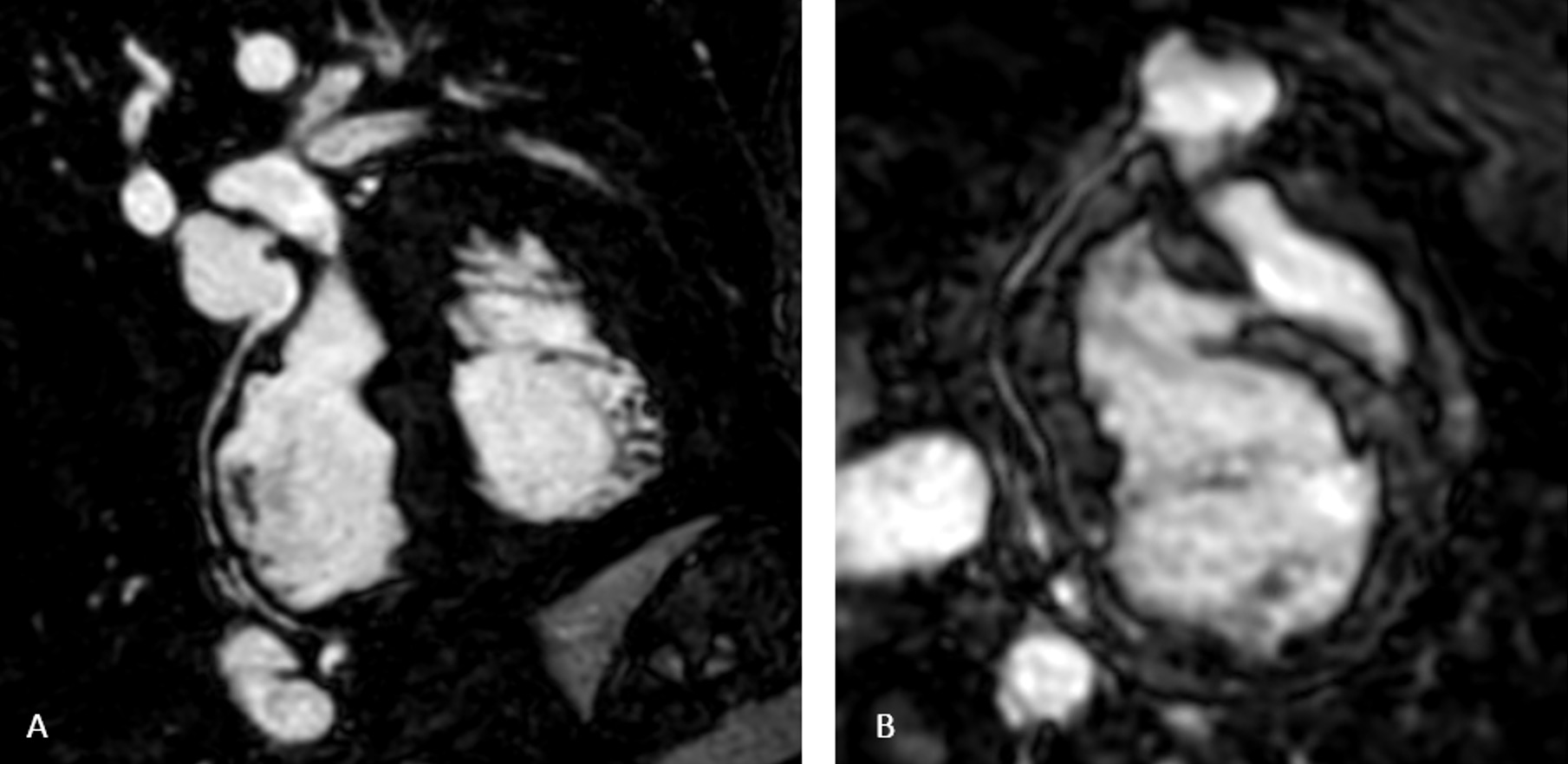
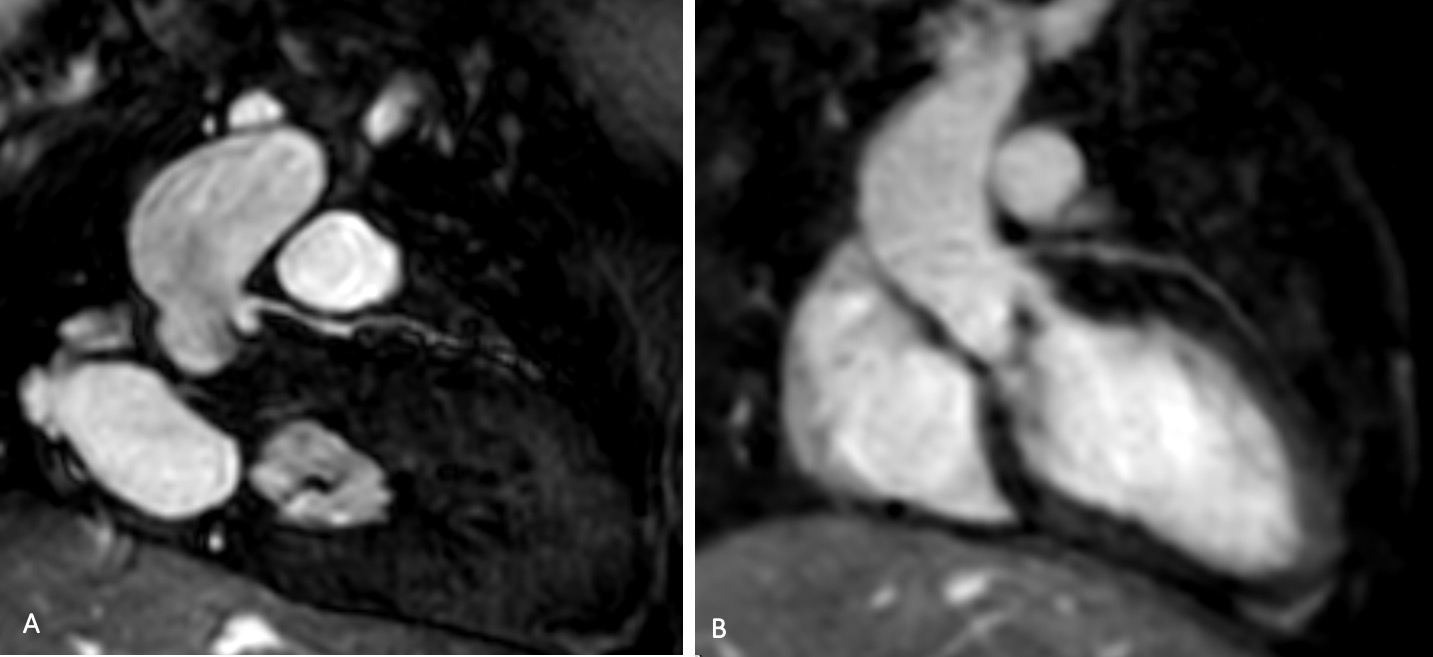
The use of lower ferumoxytol dose significantly reduced the occurrence of truncation artefact (Figure 1). Reducing the ferumoxytol dose (Table 3) significantly improved image quality (coronary artery score; p=0.02) and did not affect CNR (p=0.06). The TI used did not differ significantly between the two groups (p=0.76). Patients receiving lower ferumoxytol dose also had significantly higher diagnostic performance with 73% of patients in this group having a complete diagnosis (p=0.02).Discussion
Our study showed that Gibbs’ truncation artefact was common in patients undergoing 3D Whole-Heart Imaging with IR after ferumoxytol infusion. Reducing the dose of the contrast to 2mg/kg decreased the occurrence of this artefact, improved image quality, and diagnostic performance without affecting CNR or the TI employed. Other approaches to reduce the truncation artefact may have included employing a longer TI or increasing the resolution of the image. However, using a longer TI would not allow systolic imaging (due to the inversion delay becoming longer than the desired trigger delay) in a large number of cases. Similarly, increasing the acquired resolution has an associated time and signal penalty. The dose reduction, as outlined in this study, is the most efficient method for image optimizationConclusion
The use of reduced ferumoxytol dose may lead to a better image quality and higher diagnostic performance.Acknowledgements
The authors would like to acknowledge the MRI team of technicians at Children's Medical Center, Dallas.References
1. Bashir MR, Bhatti L, Marin D, Nelson RC. Emerging applications for ferumoxytol as a contrast agent in MRI. J Magn Reson Imaging. 2015;41(4):884-898. doi:10.1002/jmri.246912.
2. Finn JP, Nguyen KL, Han F, et al. Cardiovascular MRI with ferumoxytol. Clin Radiol. 2016;71(8):796-806. doi:10.1016/j.crad.2016.03.0203.
3. Makowski MR, Wiethoff AJ, Uribe S, et al. Congenital heart disease: Cardiovascular MR imaging by using an intravascular blood pool contrast agent. Radiology. 2011;260(3):680-688. doi:10.1148/radiol.111023274.
4. Moyé DM, Hussain T, Botnar RM, et al. Dual-phase whole-heart imaging using image navigation in congenital heart disease. BMC Med Imaging. 2018;18(1):1-11. doi:10.1186/s12880-018-0278-0
Figures