1081
3.0T Whole-Heart Contrast‑Enhanced Coronary Magnetic Resonance Angiography Using Ferumoxytol: A Feasibility Study1Beijing Chaoyang Hospital, Capital Medical University, Beijing, China, Beijing, China, 2Fujian Medical University Union Hospital, Fuzhou, China, 3MR Scientific Marketing, Siemens Healthcare, Beijing, China, 4Central Hospital Affiliated to Xinxiang Medical University, Xinxiang, China, 5Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
Keywords: Vessels, Blood vessels, Ferumoxytol
This study suggested the feasibility of combining low-dose ferumoxytol (2.0-3.0 mg/kg) with ECG-triggered, navigator-gated, inversion-recovery prepared, segmented gradient-echo sequence to obtain high-quality sub-millimeter 3D whole-heart CMRA images under free-breathing for approximately 7 mins on MR 3.0T scanner. Compared to gadobenate, ferumoxytol produced more intense and prolonged cardiac vessel enhancement (24-36 hours) Ferumoxytol could help to reduce acquisition time of CMRA while maintaining a high signal-to-noise ratio, great image quality, and clear delineation of the coronary arteries. This study of healthy volunteers also suggested that ferumoxytol-enhanced CMRA has the potential to identify patients without coronary artery disease.Introduction
3.0T gadolinium-enhanced whole-heart coronary MR angiography (Gd-CMRA) using 32-channel cardiac coils had a high specificity for obstructive coronary artery disease (CAD) in intermediate symptomatic patients[1]. However, the blood pool signal with gadolinium-based contrast agents (GBCA) varies over time and among subjects. Ferumoxytol is a potent iron-based blood pool contrast agent with a prolonged intravascular half-life of more than15 hours that can support a plethora of applications and workflows beyond those available with GBCA[2]. The China Food and Drug Administration recently approved clinical trials of domestic ferumoxytol for MR diagnosis. This study aims to assess the feasibility of 3.0T whole-heart CMRA using low-dose domestic ferumoxytol (FE-CMRA).Methods
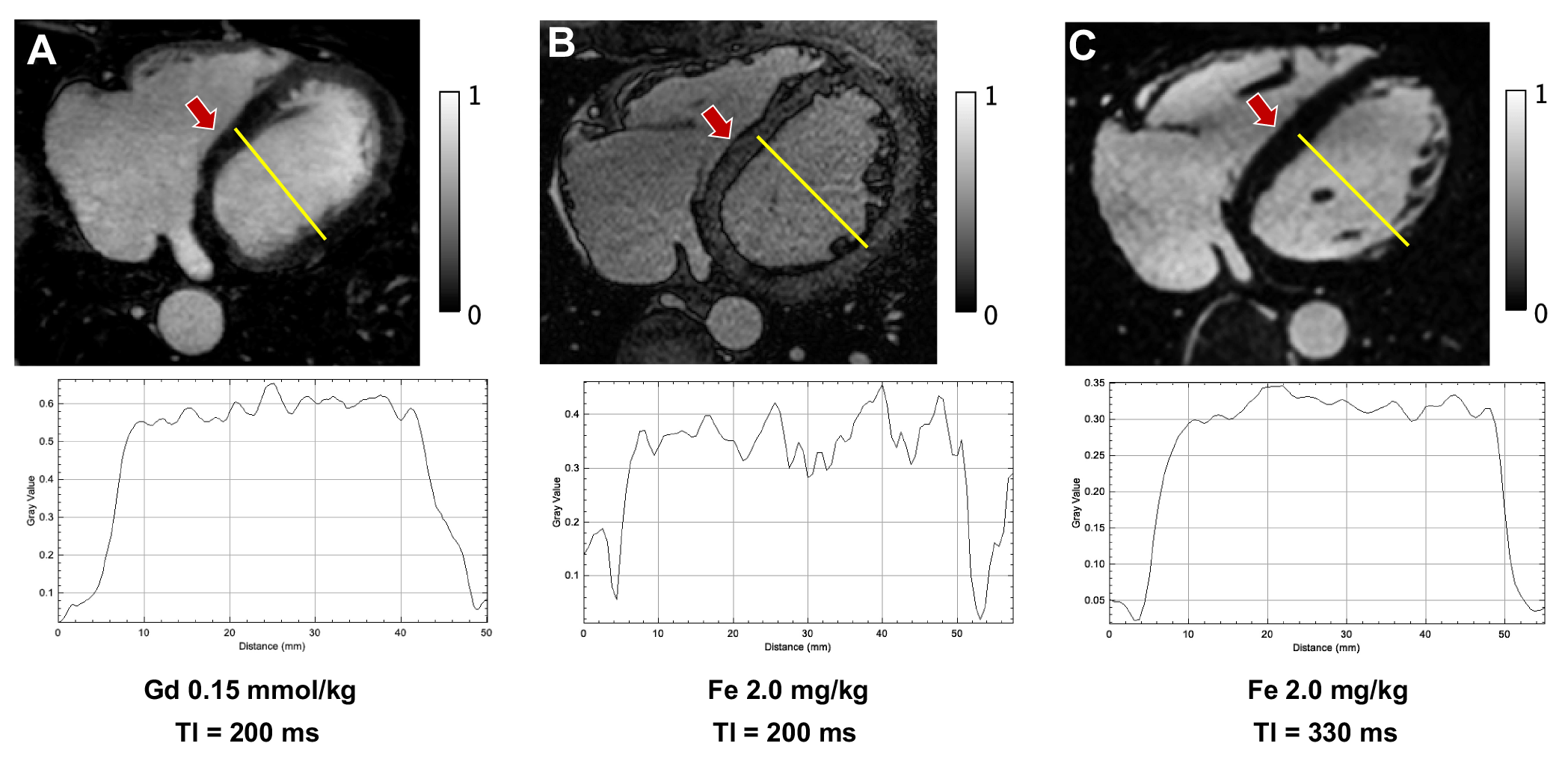
Institutional review board approval and informed consent were obtained for this study. In 7 healthy male volunteers (age: 31.1 ± 4.8 years; BMI: 23.6 ± 1.9 kg/m2), an ECG-triggered, navigator-gated, inversion-recovery prepared, segmented gradient-echo sequence (IR-FLASH) was performed on a 3.0T MAGNETOM Skyra (Siemens Healthcare, Erlangen, Germany) with 18-channel body coils. Ferumoxytol (Chia Tai Tianqing Pharmaceutical Group Co., Ltd., Jiangsu, China) was administered at a total dose of 2.0/2.5/3.0 mg/kg for 2, 2, and 3 participants, respectively, and at a flow rate of 0.07 mL/s. Key parameters were: TR/TE = 2.8/1.2 ms, flip angle = 20°, TI = 315~450 ms, spatial resolution = 0.6×0.6×0.9 mm3 (interpolated), GRAPPA acceleration factor = 2. One healthy subject underwent FE-CMRA (2.0 mg/kg Fe) with a TI of 200 ms. We retrospectively reviewed the image data set of Gd-CMRA (gadobenate dose of 0.15 mmol/kg body, flow rate of 0.3 mL/s) with 3.0T MAGNETOM TrioTim (Siemens Healthcare, Erlangen, Germany) and 32-channel cardiac coil. Three male subjects (age: 59.7±10.4 years; BMI: 23.7±2.5 kg/m2) with normal coronary arteries were chosen to compare the difference between FE-CMRA and Gd-CMRA. TR/TE = 3.3/1.5ms, flip angle = 20°, TI=200ms, spatial resolution = 0.6×0.6×0.9 mm3 (interpolated), GRAPPA acceleration factor = 3. Two radiologists independently rated FE-CMRA and Gd-CMRA image quality. The Kappa analysis was used for consistent evaluation. The ranking results among different Fe dosage groups were compared using Kruskal-Wallis test. Vessel sharpness and length of the coronary arteries were evaluated. The images were reconstructed using Ziostation (Version 2.4.0, Tokyto, Japan).Results
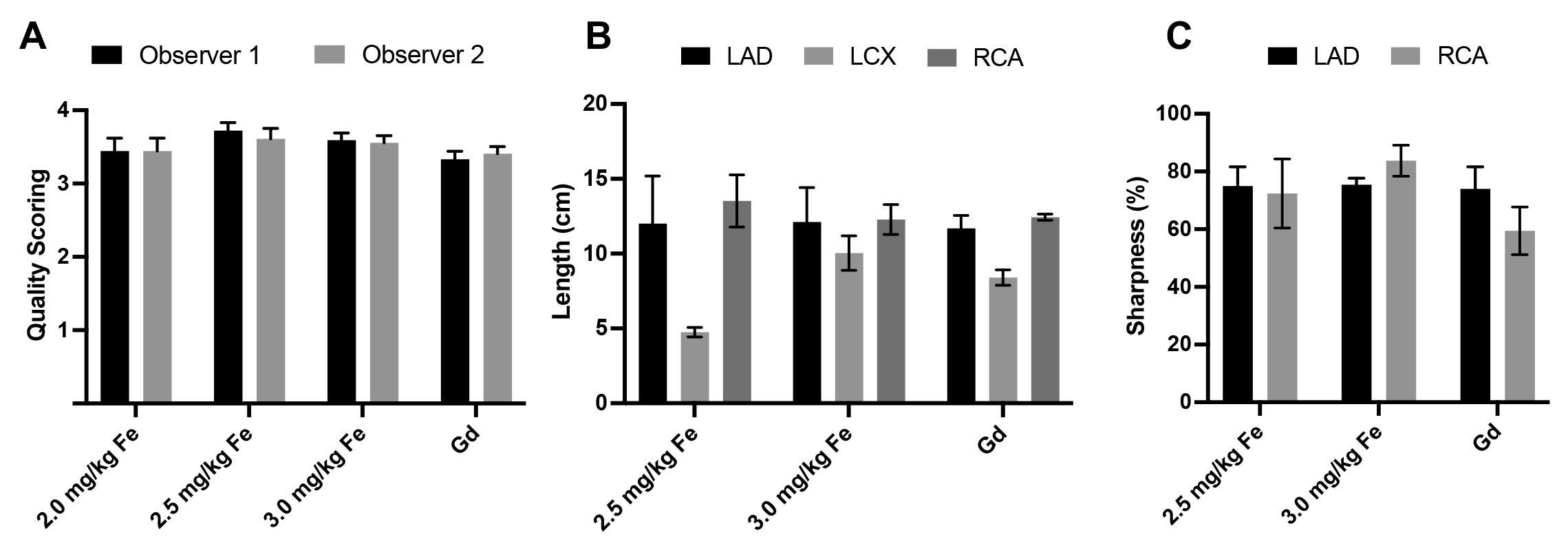
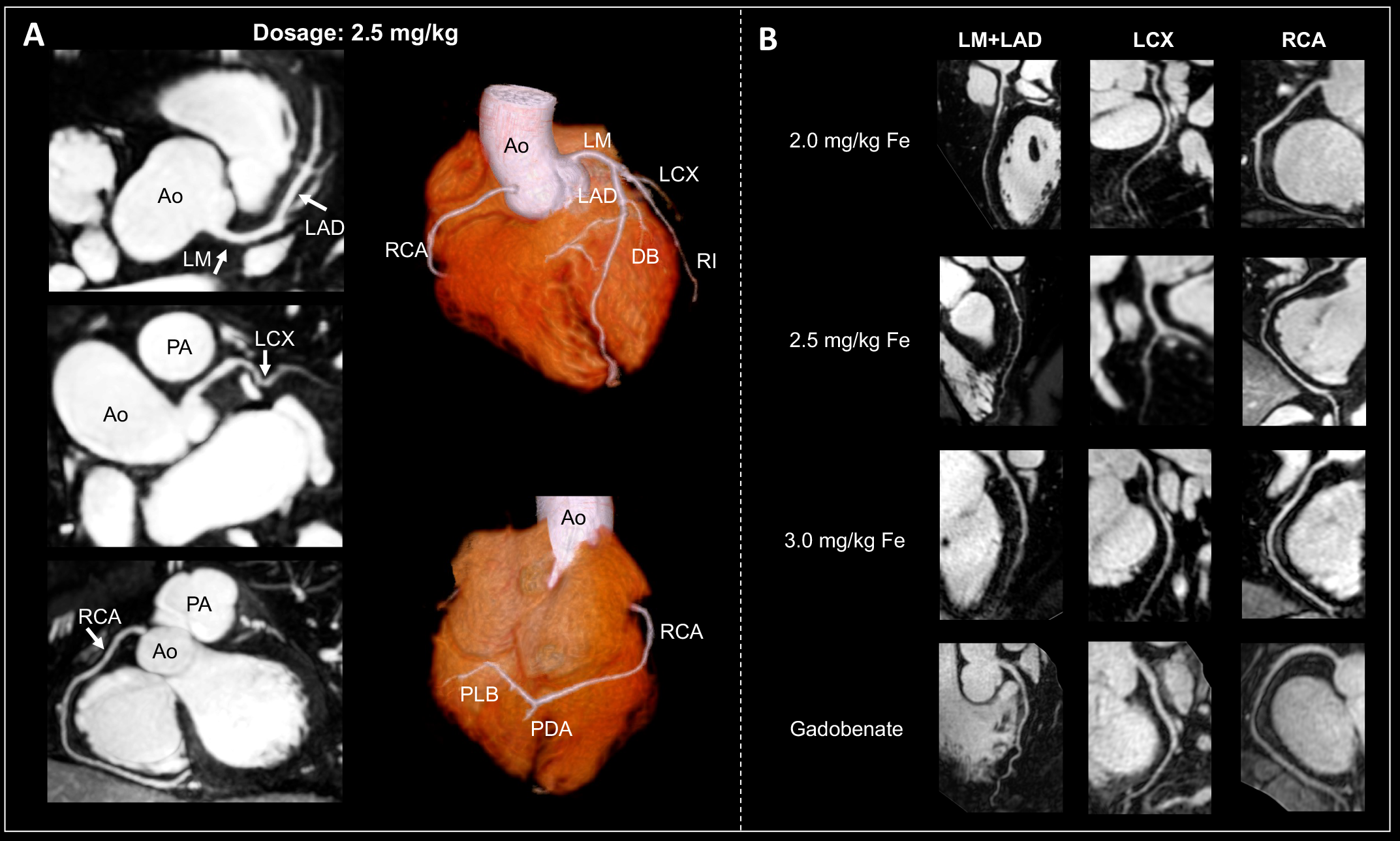
All healthy subjects successfully underwent whole-heart FE-CMRA without any adverse events. Average scan time of FE-CMRA and Gd-CMRA was 7.7 ± 2.2 min and 7.6 ± 2.1 min, respectively. A TI value between 315 and 450 ms effectively nulled myocardium for FE-CMRA. Figure.1 displays one of the cases. The image quality scores (Figure. 2A) of FE-CMRA (6 subjects, 54 segments) and Gd-CMRA (3 subjects, 27 segments) were highly consistent between the two radiologists (κ = 0.83, 95% CI: 0.73-0.95, P < 0.001). The mean image quality score for FE-CMRA was 3.6 ± 0.5, and for Gd-CMRA was 3.3 ± 0.5. There was no significant difference in image quality score among the Fe dosage groups (P = 0.370). FE-CMRA and Gd-CMRA showed good delineation of the coronary arteries, permitting the full-length measurement for coronary arteries (Figure. 2B). Vessel sharpness (Figure. 2C) was improved with the ferumoxytol injection (first 4 cm, LAD: 75.2 ± 5.5%, RCA: 79.2 ± 12.3%) compared with Gd-CMRA (first 4 cm, LAD: 74.0 ± 13.1%, RCA:59.5 ± 14.3%). No significant narrowing of the coronary arteries was found in FE-CMRA or Gd-CMRA images. Representative CMRA images are shown in Figure. 3 and Figure. 4.Discussion
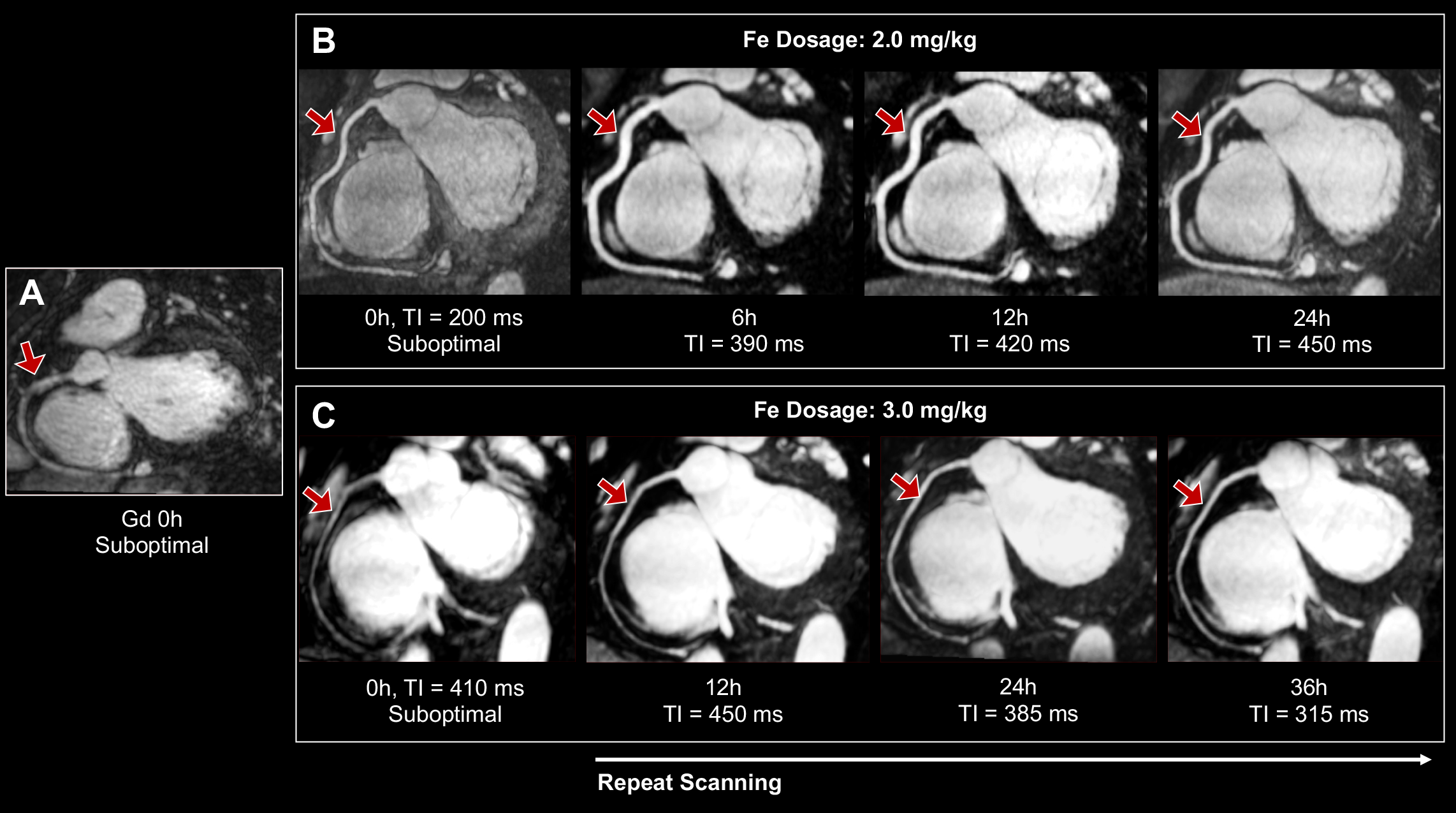
Ferumoxytol provides a significant T1-shortening effect in the blood pool that particularly benefits GRE sequences. It remains in the blood pool, and does not diffuse into the extracellular fluid space, which is useful to MRA[3]. In the current study, we investigated the feasibility of ferumoxytol for free-breathing CMRA using IR-FLASH. Considering the different MRI properties between ferumoxytol and GBCA, we selected the optimal TI values [4] for myocardial signal suppression when performing FE-CMRA with the IR-FLASH sequence. The intense vessel enhancement, qualitative scores for image quality, and coronary artery sharpness reflected the success of free-breathing sub-millimeter 3D whole-heart CMRA using both agents. Nevertheless, ferumoxytol has advantage in blood pool stability. We found that FE-CMRA can be repeated or modified until satisfactorily completed. Furthermore, ferumoxytol has higher r1 relaxivity than GBCA[5]. Thus, the SNR obtained with ferumoxytol can be used to trade off spatial and temporal resolution of CMRA with parallel imaging, reducing scanning time even more. Roy et al. [6] successfully used the fully self-gated free-running framework for motion-resolved 5D imaging of the whole heart in pediatric congenital heart disease patients injected with ferumoxytol over a wide range of heart rates, implying that ferumoxytol allows high spatial resolution and high temporal resolution CMRA. Nonetheless, a number of ferumoxytol limitations, including safety, must be addressed. Given this, the dose of domestic ferumoxytol we used in our study was 25%-50% lower than that used in previous vascular imaging studies (4 mg/kg), and the image quality was still excellent. Our study suggested that FE-CMRA has the potential to be used to identify the patient without CAD.Conclusion
Domestic low-dose ferumoxytol offers an almost ideal approach to high-resolution CMRA in healthy subject. It produces a more uniform and stable enhancement of the cardiac blood pool than gadolinium, providing a wider time window for optimal image acquisition.Acknowledgements
This work was supported by the National Science Foundation of China (NSFC 82025018).References
[1] Yang Q, Li K, Liu X, Du X, Bi X, Huang F, Jerecic R, Liu Z, An J, Xu D, Zheng H, Fan Z, Li D. 3.0T whole-heart coronary magnetic resonance angiography performed with 32-channel cardiac coils: a single-center experience. Circ Cardiovasc Imaging. 2012;5(5):573-9. doi: 10.1161/CIRCIMAGING.112.974972.
[2] Finn JP, Nguyen KL, Hu P. Ferumoxytol vs. Gadolinium agents for contrast-enhanced MRI: Thoughts on evolving indications, risks, and benefits. J Magn Reson Imaging. 2017 Sep;46(3):919-923. doi: 10.1002/jmri.25580.
[3] Nguyen KL, Moriarty JM, Plotnik AN, Aksoy O, Yoshida T, Shemin RJ, Suh WM, Finn JP. Ferumoxytol-enhanced MR Angiography for Vascular Access Mapping before Transcatheter Aortic Valve Replacement in Patients with Renal Impairment: A Step Toward Patient-specific Care. Radiology. 2018;286(1):326-337. doi: 10.1148/radiol.2017162899.
[4] Bi X, Li D. Coronary arteries at 3.0 T: Contrast-enhanced magnetization-prepared three-dimensional breathhold MR angiography. J Magn Reson Imaging. 2005;21(2):133-9. doi: 10.1002/jmri.20250.
[5] Knobloch G, Colgan T, Wiens CN, Wang X, Schubert T, Hernando D, Sharma SD, Reeder SB. Relaxivity of Ferumoxytol at 1.5 T and 3.0 T. Invest Radiol. 2018;53(5):257-263. doi: 10.1097/RLI.0000000000000434.
[6] Roy CW, Di Sopra L, Whitehead KK, Piccini D, Yerly J, Heerfordt J, Ghosh RM, Fogel MA, Stuber M. Free-running cardiac and respiratory motion-resolved 5D whole-heart coronary cardiovascular magnetic resonance angiography in pediatric cardiac patients using ferumoxytol. J Cardiovasc Magn Reson. 2022;24(1):39. doi: 10.1186/s12968-022-00871-3.
Figures