1072
Effects of double-ECG gating in synchronized breathing myocardial arterial spin labeling1Radiology, Clínica Universidad de Navarra, Pamplona, Spain, 2IdiSNA, Instituto de Investigación Sanitaria de Navarra, Pamplona, Spain, 3Siemens Healthineers, Madrid, Spain
Synopsis
Keywords: Heart, Perfusion
Myocardial perfusion can be quantitatively measured noninvasively using arterial spin labeling (ASL). Motion due to the cardiac cycle is tackled with the use of single- or double-ECG gating. The goals of this study were to investigate the performance of double-gating, in synchronized breathing myocardial ASL with presaturation pulses by comparison with single-gating, and to compare the different quantification strategies for double-gated data. This study showed that double-gating is more robust to heart rate variability than single-gating in synchronized breathing ASL sequences with presaturation pulses, but accurate saturation-recovery fitting requires the acquisition of several baseline images.INTRODUCTION
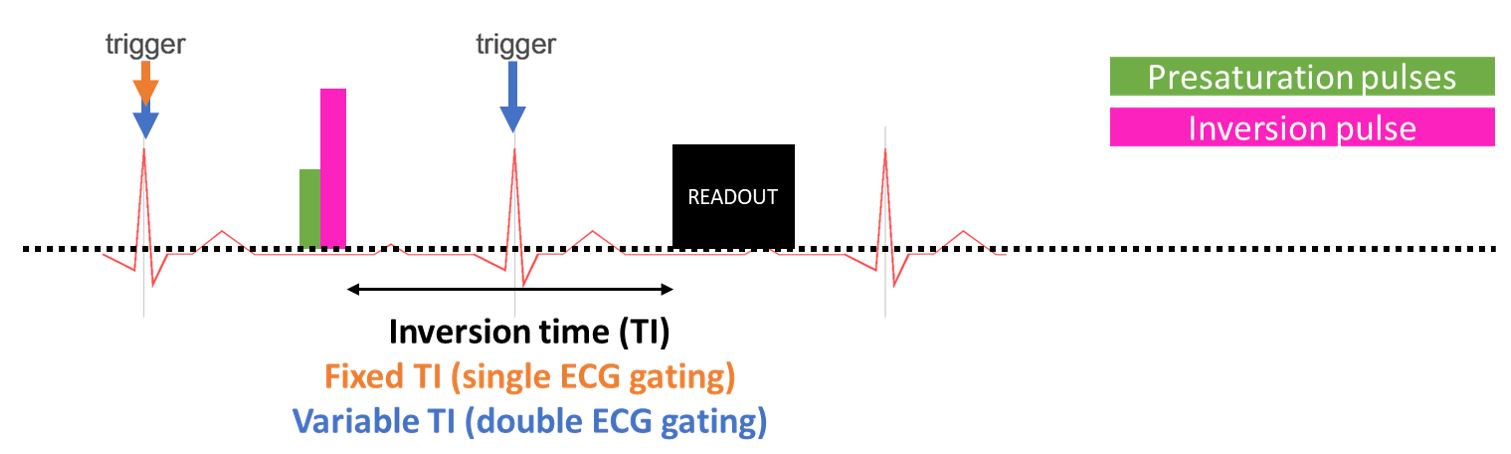
Myocardial blood flow (MBF) can be quantitatively measured noninvasively in MRI using arterial spin labeling (ASL) and most typically a flow-sensitive alternating inversion recovery (FAIR-ASL) approach has been used. The ASL signal is computed by subtraction of label from control images acquired with different time stamps, increasing the likelihood of motion artifacts. Thus, strategies to mitigate the effects of motion are critical to obtain a reproducible signal. In cardiac ASL, motion due to the cardiac cycle is tackled with the use of either single- or double-ECG gating. The former uses one trigger to gate the labeling pulse, and the latter two independent triggers (one for labeling and another for readout) to assure they both occur in the same cardiac phase even in the presence of heart rate variability (HRV) [1]. However, despite the potential of double-gated myocardial ASL observed under breath-holding conditions, this technique has not been tested using other breathing strategies. Moreover, different quantification approaches for double-gated data have been reported [2], [3]. Therefore, the goals of this study were to investigate the performance of double-gating, in synchronized breathing myocardial FAIR-ASL with presaturation pulses by comparison with single-gating, and to compare the different quantification strategies for double-gated data.METHODS
Data acquisition: 4 healthy volunteers (2 female, 31 ± 6 years) underwent a cardiac MRI scan at 1.5 T (Siemens, AERA). The cardiac MRI protocol consisted on: localizers to identify a mid-ventricular short axis slice, myocardial FAIR-ASL sequences with double and single-ECG gating with presaturation and hyperbolic secant inversion pulses(Figure 1) and T1 mapping using MOLLI. For each FAIR-ASL series, 15 pairs of label/control images were acquired. For single-gating, inversion time (TI) was fixed at 1s. Additionally, 4 images at short TI and 6 images with no inversion (M0) were acquired and used for quantification. In FAIR-ASL sequence, a balanced steady-state (bSSFP) readout was used with the following parameters: field of view (FOV) = 300x243mm2, matrix = 128x104, repetition time (TR) = 5s, pixel size = 2.3x2.3 mm2 and GRAPPA-2. Volunteers were instructed to synchronize their breathing to the sequence sounds to minimize respiratory motion. Heart rate was recorded for each sequence.Data analysis: All FAIR-ASL images were pairwise registered [4]. Outliers were identified based on the final metric obtained after registration and discarded. Regions of interest covering the left ventricular myocardium were manually drawn for each sequence.
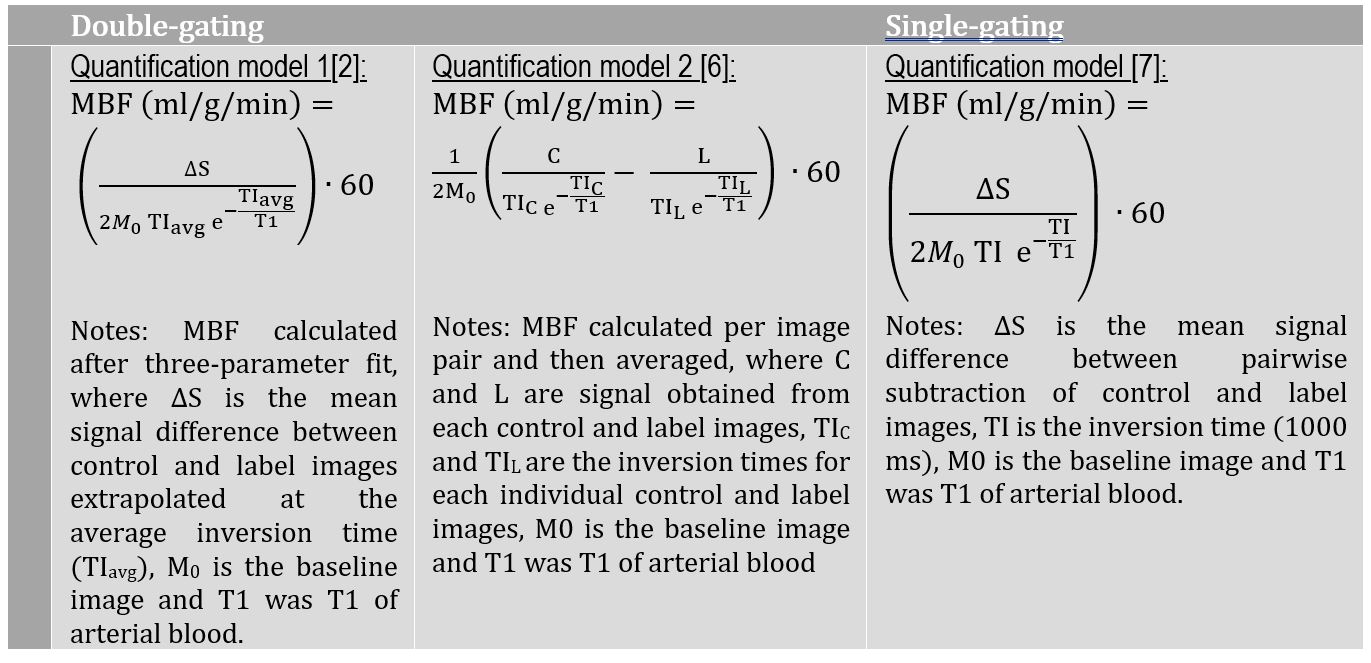
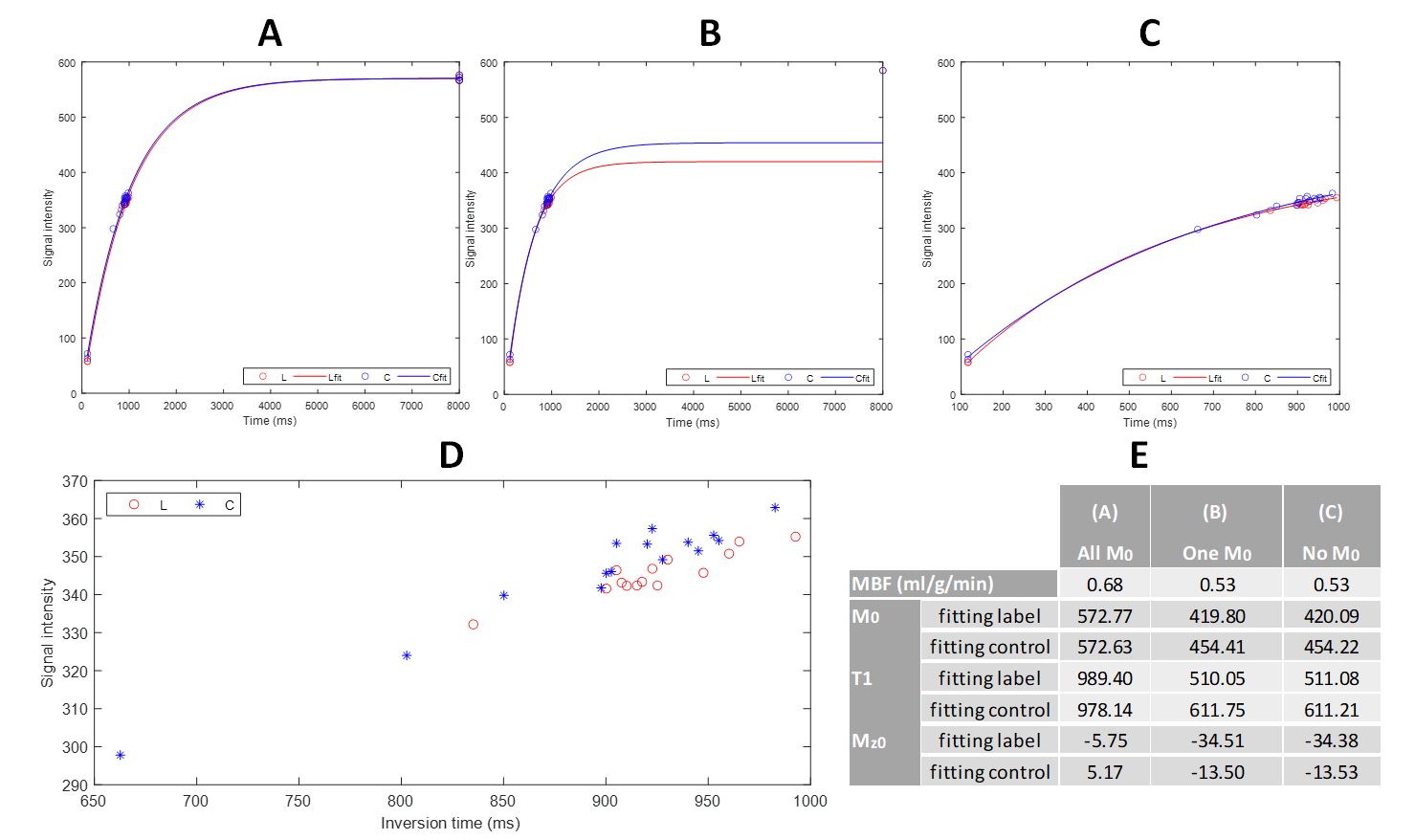
For double-gating, a three-parameter (M0, Mz0, T1) saturation recovery model was used to fit the label and control image data separately. Fitting was repeated employing different number of baseline images (6, 1 and 0). MBF was quantified using two different models (Figure 2). For single-gating, pairwise subtraction between individual control and label image pairs was performed and MBF was estimated using the equation derived from Buxton’s general kinetic model (Figure 2). T1 of arterial blood at 1.5T was 1.434s [5].
Temporal signal-to-noise ratio (tSNR) was computed as the mean quantitative perfusion signal divided by its temporal standard deviation. For the double-gating quantification model that used the fitting approach, temporal data were obtained by subtracting each control image data minus the fitted label signal obtained at the corresponding inversion time.
Statistical analysis: MBF and tSNR results were compared between double and single-gating using Wilcoxon signed-rank test.
RESULTS AND DISCUSSION
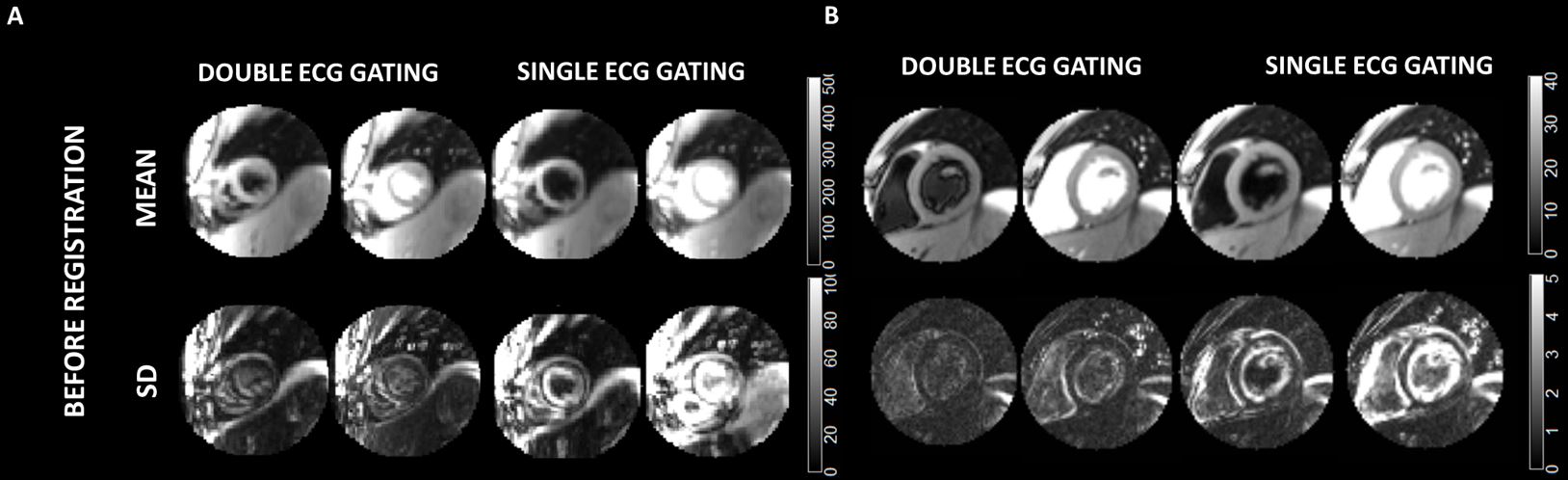
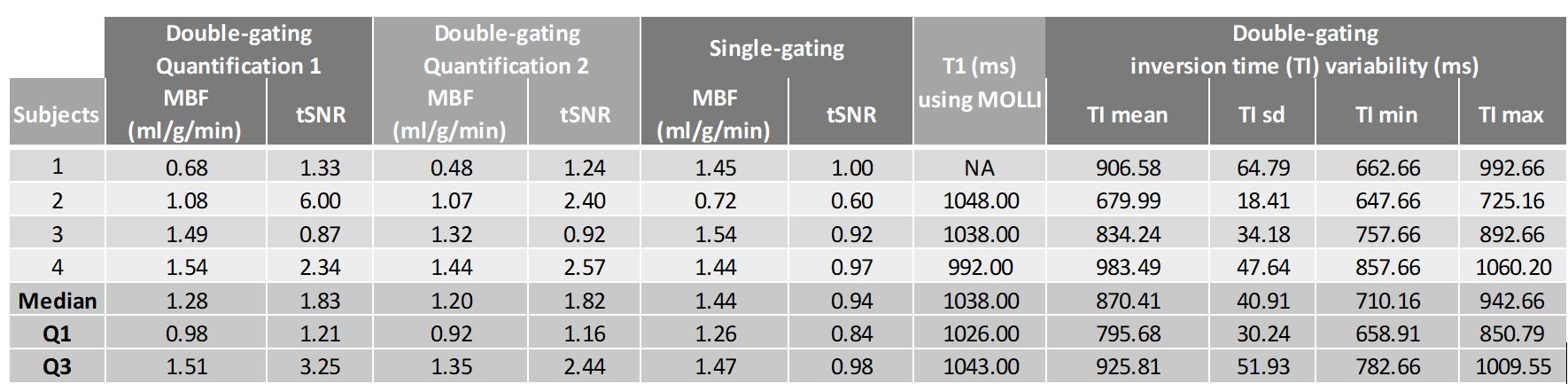
Figure 3 shows the mean and standard deviation of label and control images separately for two representative subjects with different levels of heart rate variation. It can be observed that images obtained with double-gating present a lower degree of motion.Figure 4 shows quantitative data obtained per subject together with the median and interquartile range across subjects. MBF values obtained with double and single-gating were not different (p=1,p=0.57 for quantification model 1 and 2, respectively), in agreement with previous work [1]. MBF values obtained with both quantitative methods show similar results. tSNR was greater for double-gating than single-gating sequences, although differences were non-significant (p=0.14 and 0.09 for quantification model 1 and 2, respectively), likely due to the small sample size. Median TI variabilities of 40.91 (30.24-51.93) ms were observed.
Figure 5 shows three-parameter fitting comparison using different numbers of baseline images. Although similar MBF values were obtained, T1 estimates were closer to myocardial T1 (measured with MOLLI) if more than one M0 image was used.
CONCLUSION
Double-gating is more robust to heart rate variability than single-gating in synchronized breathing ASL sequences with presaturation pulses, but accurate saturation-recovery fitting requires the acquisition of several baseline images.Acknowledgements
Spanish Ministry of Science and Innovation (grant: PI21/00578)References
[1] H. P. Do, A. J. Yoon, M. W. Fong, F. Saremi, M. L. Barr, and K. S. Nayak, “Double-gated myocardial ASL perfusion imaging is robust to heart rate variation,” Magn. Reson. Med., vol. 77, no. 5, pp. 1975–1980, 2016, doi: 10.1002/mrm.26282.
[2] B. P. Poncelet et al., “Measurement of human myocardial perfusion by double-gated flow alternating inversion recovery EPI,” Magn. Reson. Med., vol. 41, no. 3, pp. 510–519, 1999, doi: 10.1002/(SICI)1522-2594(199903)41:3<510::AID-MRM13>3.0.CO;2-G.
[3] M. Henningsson, C.-J. Carlhäll, and J. Kihlberg, “Myocardial arterial spin labeling in systole and diastole using flow-sensitive alternating inversion recovery with parallel imaging and compressed sensing,” NMR Biomed., vol. n/a, no. n/a, p. e4436, 2020, doi: 10.1002/nbm.4436.
[4] V. Aramendía-Vidaurreta et al., “Reduction of motion effects in myocardial arterial spin labeling,” Magn. Reson. Imaging, pp. 1261–1275, 2022.
[5] X. Zhang et al., “In vivo blood T 1 measurements at 1.5 T, 3 T, and 7 T,” Magn. Reson. Med., vol. 70, no. 4, pp. 1082–1086, 2013, doi: 10.1002/mrm.24550.
[6] M. Henningsson, C. J. Carlhäll, T. Ebbers, and J. Kihlberg, “Non-contrast myocardial perfusion in rest and exercise stress using systolic flow-sensitive alternating inversion recovery,” Magn. Reson. Mater. Physics, Biol. Med., no. 0123456789, 2021, doi: 10.1007/s10334-021-00992-3.
[7] R. B. Buxton, L. R. Frank, E. C. Wong, B. Siewert, S. Warach, and R. R. Edelman, “A general kinetic model for quantitative perfusion imaging with arterial spin labeling.,” Magn. Reson. Med., vol. 40, no. 3, pp. 383–396, 1998, doi: 10.1002/mrm.1910400308.
Figures