0887
Pseudo-continuous arterial spin labeling evaluation of collateral circulation at 7T and 3T MRI in Moyamoya disease
Jinhao Lyu1, Qi Duan2, Caohui Duan2, Xiangbing Bian2, Danny JJ Wang3, Chenyang Zhao3, Jianxun Qu4, and Lou Xin2
1Radiology, Chinese PLA General Hospital, Beijing, China, 2Chinese PLA General Hospital, Beijing, China, 3Mark & Mary Stevens Neuroimaging and Informatics Institute Keck School of Medicine University of Southern California (USC), Los Angeles, CA, United States, 4MR Collaboration, Siemens Healthineers Ltd., Beijing, China
1Radiology, Chinese PLA General Hospital, Beijing, China, 2Chinese PLA General Hospital, Beijing, China, 3Mark & Mary Stevens Neuroimaging and Informatics Institute Keck School of Medicine University of Southern California (USC), Los Angeles, CA, United States, 4MR Collaboration, Siemens Healthineers Ltd., Beijing, China
Synopsis
Keywords: Stroke, Perfusion
We compared the performance of pseudo-continuous arterial spin labeling (ASL) between ultrahigh field 7T MRI and 3T MRI in evaluating collateral circulation based on arterial transit artifact (ATA) in Moyamoya disease (MMD). 7T ASL shows more subtle hypoperfusion and more prominent ATA as compared with 3T ASL. The performance of collateral circulation assessment is more favorable by 7T ASL. These findings render 7T ASL a competing none-invasive approach in the management of MMD.INTRODUCTION
Collateral circulation assessment is pivotal for patients’ management in patients with Moyamoya disease (MMD). Arterial transit artifact (ATA) is an established none-invasive imaging marker derived from arterial spin labeling (ASL) to depict leptomeningeal collaterals in cerebrovascular occlusive disease1. We aimed to compare the performance of ASL between ultrahigh field 7T MRI and 3T MRI in evaluating collateral circulation based on ATA.METHODS
Patients suspected MMD were prospectively recruited in the study from August 2022 to October 2022 in a hospital center. Participants were analyzed in this study if they had performed both 3T (GE Discovery MR 750, GE Healthcare, Milwaukee, WI), and 7T ASL (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) and conventional angiography within 1 month. Whole brain ASLs acquired from 3T and 7T scanners were both with pseudo-continuous labeling scheme and with a post-labeling delay (PLD) of 2000 ms. The voxel size of 7T ASL was 2.2 x 2.2 x 4.0 mm3 or 2.2 x 2.2 x 5.0 mm3. A modified Alberta Stroke Program Early Computed Tomography Score (ASPECTS) system, which assessed the global changes of both hemispheres from 0 to 22, is applied for the evaluation of hypoperfusion and ATA in accordance with insular, M1–M6, A1-A2 and P1-P2 regions in the original ASPECTS (Figure 1A). A larger hypoperfusion-ASPECTS or ATA-ASPECTS indicated more prominent hypoperfusion or ATA. In the collateral circulation evaluation, an established scoring system 0-3 was employed which based on the identification of the hypoperfusion region and ATA on ASL2. The hypoperfusion was used to determine the ischemic region, and ATA was used to depict the presence and robustness of the collaterals. A larger collateral grade on ASL indicated better collaterals. The gold standard of collateral evaluation was American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) scale assessed by conventional angiography. Imaging reading was performed by two experienced neuroradiologists (with 6 and 12 years of experience). The differences in opinions between them were resolved by consensus reading. Collateral grades, ATA-ASPECTS and hypoerfusion-ASPECTS from different modalities were statistically compared.RESULTS
Nine patients were recruited in the final analysis. There were 4 men and 5 females. The mean age was 41.44±11.50 years. Global ATA-ASPECTS on 7T ASL was significantly higher compared with Global ATA-ASPECTS on 3T ASL (median 7 [Interquartile range 2.75-7.25] versus median 3 [Interquartile range 1.75-4], P=0.016, Wilcoxon test). Global Hypoperfusion-ASPECTS on 7T ASL was significantly higher compared with Global ATA-ASPECTS on 3T ASL (median 5 [Interquartile range 2.75-7] versus median 3 [Interquartile range 1.75-4.75], P=0.031, Wilcoxon test) (Figure 1B). In collateral assessment, eleven hemispheres were analyzed since 2 patients were bilateral lesions. Collateral grades on 7T ASL were higher but not significantly compared with collateral grades on 3T ASL (median 2 [interquartile range 2-2] versus median 2 [interquartile range 1-2], P=0.156, Wilcoxon test). Collateral grades on 7T ASL were not significantly correlated with Collateral grades on 3T ASL (rho=0.578, p=0.063, Spearman correlation). Collateral grades on 3T ASL were not significantly correlated with ASITN/SIR grades (rho=0.512, p=0.107, Spearman correlation). Collateral grades on 7T ASL were significantly correlated with ASITN/SIR grades (rho=0.831, p=0.002, Spearman correlation). Representative case was shown in Figure 2.CONCLUSION
As compared with 3T ASL, 7T ASL shows more subtle hypoperfusion and more prominent ATA. The accuracy of collateral circulation assessment is more favorable by 7T ASL. These findings render 7T ASL a competing none-invasive approach in the management of MMD.Acknowledgements
This work was supported by The National Natural Science Foundation of China (Contract grant number: 81901708 to J.H.L. and Contract grant number: 81825012, 81730048 and 82151309 to X.L.).References
1.Zaharchuk G, Do HM, Marks MP, et al. Arterial spin-labeling MRI can identify the presence and intensity of collateral perfusion in patients with moyamoya disease. Stroke. 2011;42(9):2485-91.
2.Lyu J, Hu J, Wang X, et al. Association of fluid-attenuated inversion recovery vascular hyperintensity with ischaemic events in internal carotid artery or middle cerebral artery occlusion. Stroke Vasc Neurol. 2022. doi: 10.1136/svn-2022-001589.
Figures
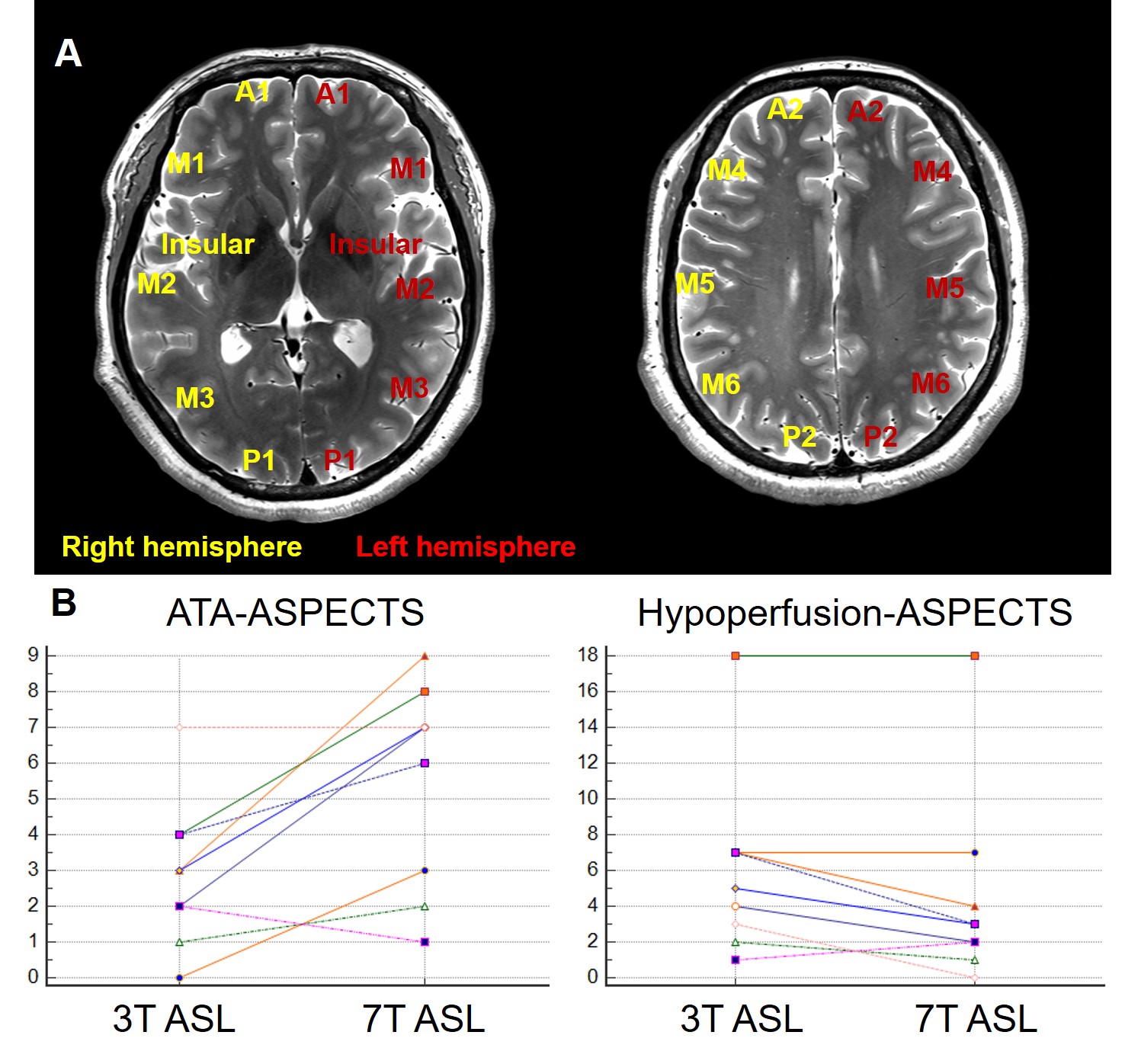
A
modified Alberta Stroke Program Early Computed Tomography Score (ASPECTS)
system is applied in this study as the figure A showed, which assesses the
global changes of arterial transit artifacts (ATAs) and hypoperfusion in both
hemispheres. Figure B shows the comparison of ATA-ASPECTS and
hypoperfusion-ASPECTS between 3T arterial spin labeling (ASL) and 7T ASL. ASL, arterial spin labeling. ATA, arterial transit artifacts. ASPECTS, Alberta Stroke Program Early Computed Tomography Score.
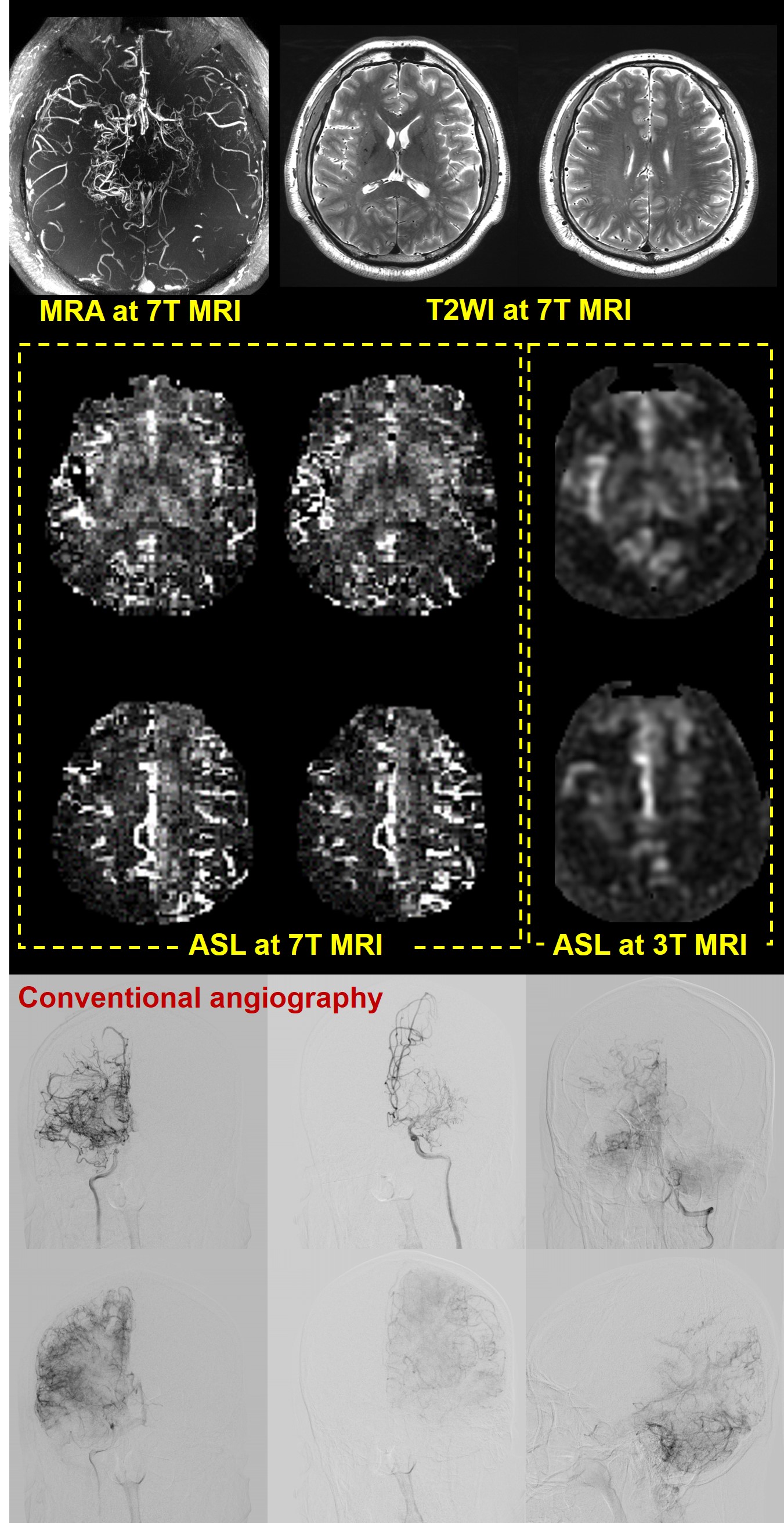
Figure
shows a 35-year-old male patient with imaging confirmed Moyamoya disease. On T2 weighted imaging, no
visible ischemic or hemorrhagic lesions are detected. On 7T arterial spin labeling (ASL), arterial transit artifacts (ATAs)
are prominent in both hemispheres, which is in line with the finding of
relative robustness collaterals and persistent ischemic regions on conventional angiography,
while ATAs are mild in right hemisphere and are none visible in left hemisphere
on 3T ASL.
MRA,
MR angiography. T2WI,
T2 weighted
imaging. ASL, arterial spin labeling.
DOI: https://doi.org/10.58530/2023/0887