0799
Utility of Thin-Slice Fat-Suppressed Single-Shot T2-Weighted MRI with Deep Learning Image Reconstruction for Pancreatic Cancer1Center of Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan, 2Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 3GE Healthcare, Hino, Japan
Synopsis
Keywords: Pancreas, Cancer
We investigated the utility of breath-hold (BH) fat-suppressed single-shot T2-weighted MRI with deep learning image reconstruction (DLIR) in 42 patients with pancreatic cancer. Three fat-suppressed T2-weighted sequences of 1) single-shot fast-spin echo (SSFSE) of 6mm thickness with 1BH, 2) SSFSE of 3mm thickness with 2BH and 3) FSE of 6mm thickness with 3BH were compared. SSFSE sequences improved signal-to-noise ratio on anatomical organs, pancreas-to-lesion contrast, and image quality in terms of motion artifacts, image sharpness, and anatomical clarity in comparison with conventional FSE. The T2-weighted SSFSE with DLIR can be a useful sequence for the evaluation of pancreatic cancer.【INTRODUCTION】
T2-weighted imaging is one of the essential sequences in MRI of the pancreas for the evaluation of focal lesion, pancreatic duct continuity, and shape of the pancreas. Single-shot fast-spin echo (SSFSE) sequence with breath hold (BH) is widely used for upper abdominal T2-weighted imaging as a fast-imaging technique. Recent technical improvements enable the shortened echo space period, high parallel imaging factor, and the extended echo train length with modulation of refocusing flip angles, which can be expected to achieve high resolution full-Fourier SSFSE. The usefulness of T2-weighted SSFSE with full-Fourier acquisition has been reported in pelvic MRI (1). Recently, the use of deep learning image reconstruction (DLIR) has been reported to improve signal-to-noise ratio (SNR) in T2-weighted SSFSE (2・3). However, there is no report regarding the use of SSFSE with DLIR and full-Fourier acquisition nor the use of thin-slice acquisition in abdominal T2-weighted imaging. The purpose of this study was to investigate the clinical utility of thin-slice T2-weighted SSFSE sequence with DLIR for the evaluation of pancreatic cancer in comparison with conventional FSE sequence.【METHODS】
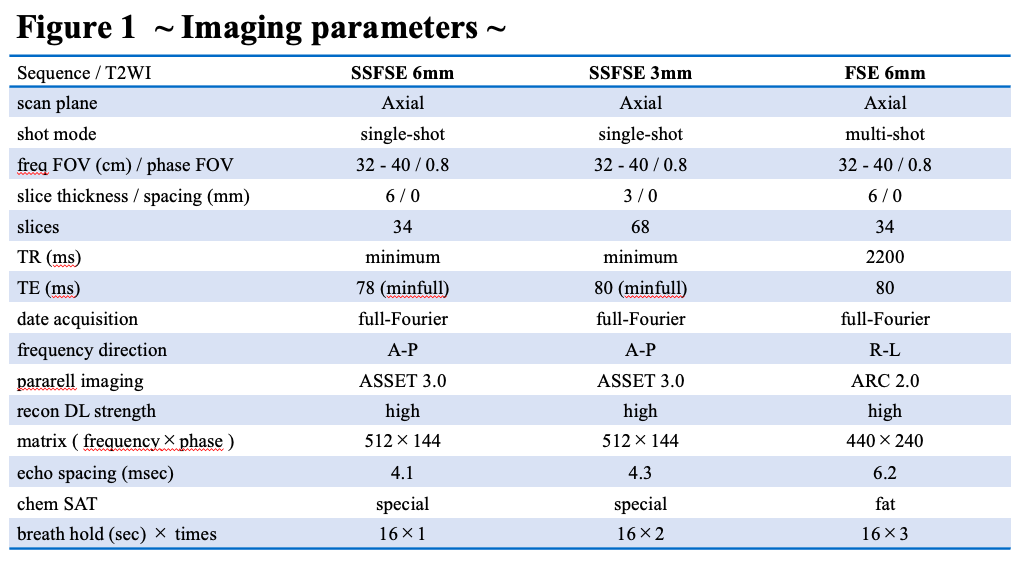
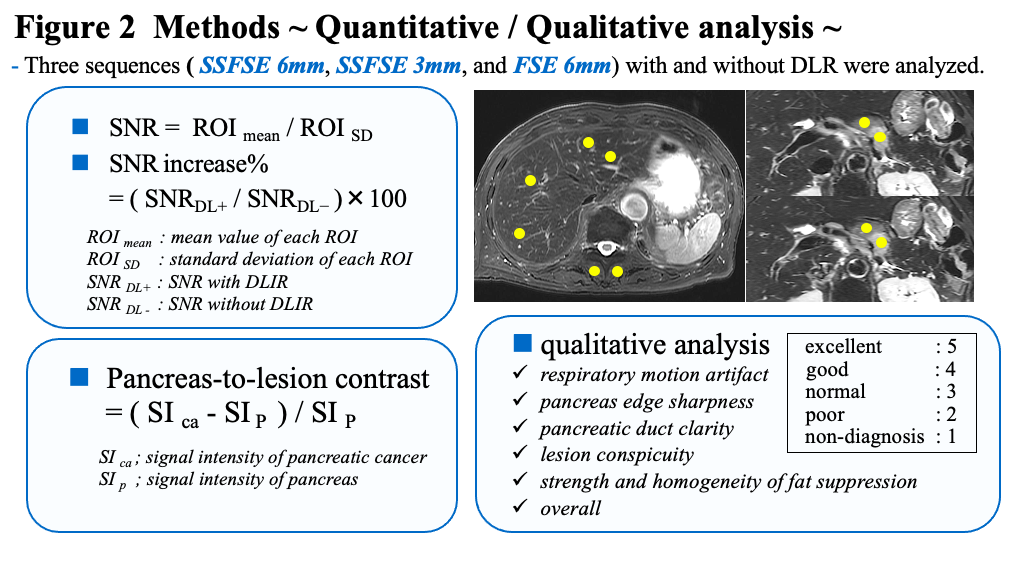
This study included 42 patients (age:70.2±10.8, male: female; 27:15, BMI: 22.4±3.5) with pancreatic cancer who underwent gadoxetic-acid enhanced MRI from January 2021 to September 2022. Three fat-suppressed T2-weighted sequences of 1) SSFSE of 6mm thickness with 1BH, 2) SSFSE of 3mm thickness with 2BH, and 3) conventional FSE of 6mm thickness with 3BH were acquired on a 3.0T MR scanner (Signa Premier, GE Healthcare). The detailed scan parameters were shown in Fig.1, and the images with and without DLIR were reconstructed from the same raw data. For quantitative analysis, the signal intensities (SI) of the liver (right and left lobes), pancreas, pancreatic cancer, paraspinal muscle, and intra-abdominal fat were measured on the respective images. The SNR was calculated by the SI of the organ divided by standard deviation. The increase in SNR by applying the DLIR (SNR increase%) and pancreas-to-lesion contrast on images with DLIR were also calculated using the equations presented in Fig.2. For qualitative analysis, two abdominal radiologists visually scored the image quality on a 5-point scale, in terms of respiratory motion artifacts, pancreas edge sharpness, pancreatic duct clarity, lesion conspicuity, strength and homogeneity of fat suppression, and overall image quality (Fig.2). For the statistical analyses, the SNRs of each organ were compared with and without DLIR using paired t-test. Pancreas-to-lesion contrasts and qualitative analyses were compared among the three T2-weighted sequences with DLIR using Kruskal-Wallis H-test, and post-hoc pairwise comparison was performed using the Dunn-test for statistically significant sequences. P values less than 0.05 were considered as statistically significant for all the statistical analyses. Statistical analysis was performed using GraphPad Prism9 (GraphPad Software).【RESULTS】
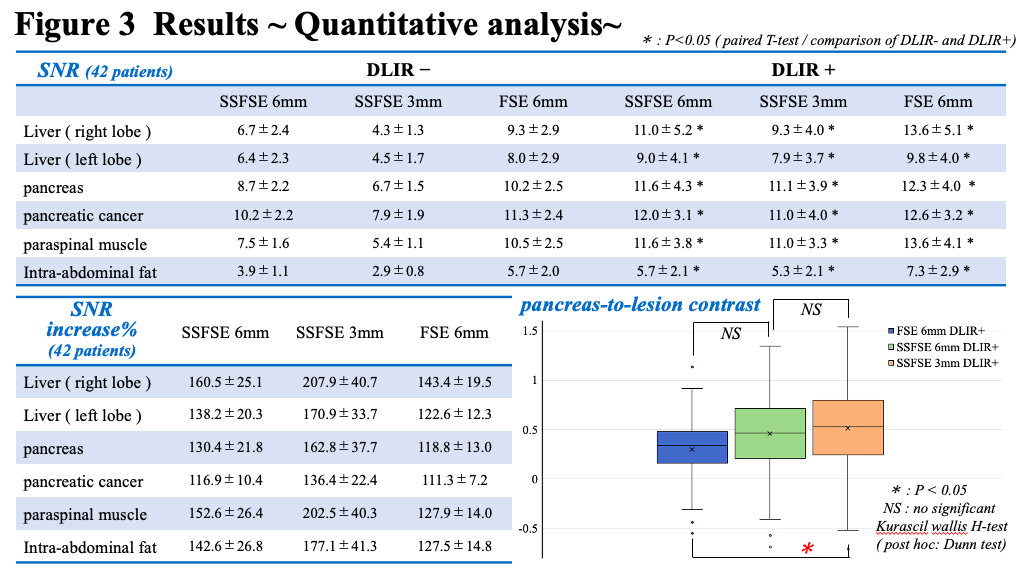
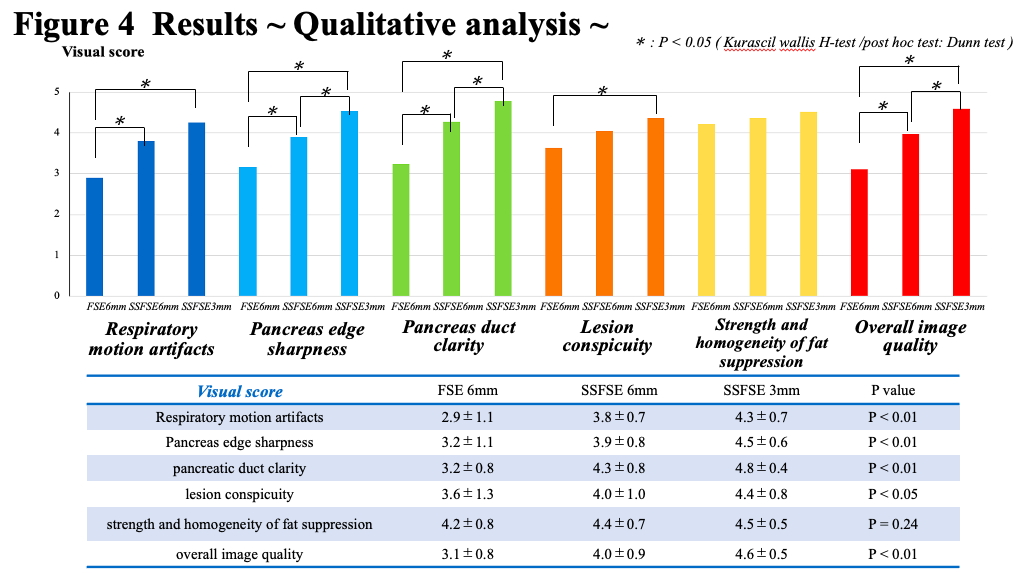
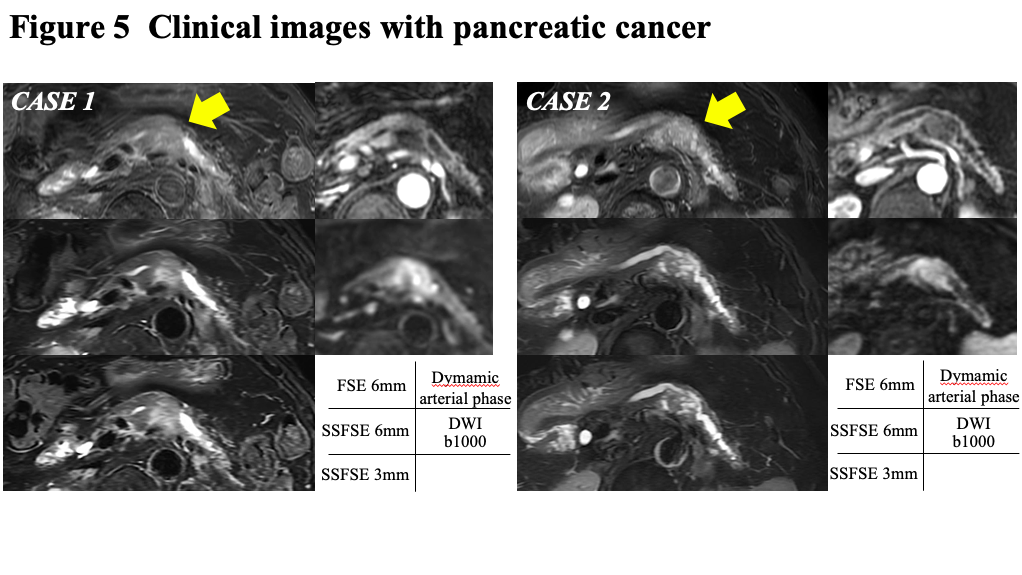
The results of quantitative analysis were shown in Fig.3. SNRs improved significantly in all organs with and without DLIR (P<0.05). The SNR increase% of SSFSE 3mm was higher than those of SSFSE 6mm and FSE 6mm in all measured organs. With DLIR, the SNRs were increased by 63%, 30% and 19% in the pancreas, and 36%, 17% and 11% in the pancreatic cancer on SSFSE 3mm, SSFSE 6mm and FSE 6mm, respectively. Pancreas-to-lesion contrast of SSFSE 3mm was higher than those of SSFSE 6mm and FSE 6mm, with the statistical difference from FSE 6mm. The results of qualitative analysis were shown in Fig.4. Visual score of SSFSE 3mm was higher than those of SSFSE 6mm and FSE 6mm in all the evaluations. Regarding respiratory motion artifacts, SSFSE 3mm and 6mm were significantly better than FSE 6mm. For lesion conspicuity, SSFSE 3mm was significantly better than FSE 6mm. Overall image quality was the best with SSFSE 3mm (4.6±0.5), followed by SSFSE 6mm (4.0±0.9) and FSE 6mm (3.1±0.8). Fig.5 shows the representative images obtained from two patients.【DISCUSSION】
We investigated the utility of SSFSE 3mm and SSFSE 6mm sequences with DLIR in comparison with conventional FSE 6mm sequence with DLIR for pancreatic cancer. The SNR increase% after applying the DLIR was the higher in SSFSE 3mm than those in SSFSE 6mm and FSE 6mm, which means significant denoising effect of SSFSE 3mm compared with SSFSE 6mm and FSE 6mm. Regarding the evaluation of respiratory motion artifacts, SSFSE was better than FSE, which is thought to be because that single-shot sequence is more robust to motion than multi-shot sequence. The thin-slice acquisition could contribute to reduce the partial volume effect, resulting in the better results of SSFSE 3mm in terms of pancreas-to-lesion contrast, pancreas edge sharpness, duct clarity and overall image quality. These findings of our results suggest that DLIR enables thin-slice acquisition of fat-suppressed T2-weighted images by improving SNR of the upper abdominal organs, pancreas-to-lesion contrast, and image quality for the evaluation of pancreatic cancer.【CONCLUSION】
Thin-slice fat-suppressed T2-weighted SSFSE sequence with DLIR can provide better pancreas-to-lesion contrast and image quality than conventional FSE sequence, which is clinically useful for the evaluation of pancreatic cancer.Acknowledgements
I would like to thank MRI staffs in Center of Radiology and Radiation Oncology for help with data collection and useful discussions.References
1. Loening AM, Litwiller DV, Saranathan M, et al. Increased speed and image quality for pelvic single-shot fast spin-echo imaging with variable refocusing flip angles and full- fourier acquisition. Radiology.2017;282(2):561-568.
2. Shanbhogue K, Tong A, Smereka P, et al. Accelerated single-shot T2-weighted fat-suppressed (FS) MRI of the liver with deep learning-based image reconstruction: qualitative and quantitative comparison of image quality with conventional T2-weighted FS sequence. Eur Radiol.2021 Nov;31(11):8447-8457.
3. Sheng RF, Zheng LY, Jin KP, et al. Single-breath-hold T2WI liver MRI with deep learning-based reconstruction: A clinical feasibility study in comparison to conventional multi-breath-hold T2WI liver MRI. Magn Reson Imaging.2021 Sep;81:75-81.
Figures