0789
Abbreviated MRI with Second Shot Arterial Phase for HCC Evaluation: Modified Version of LI-RADS and Recall Reduction Strategy1Radiology, Korea University Guro Hospital, Seoul, Korea, Republic of
Synopsis
Keywords: Liver, Liver
A modified version of LI-RADS was devised for abbreviated MRI (AMRI) with second shot arterial phase (SSAP) by referring to CEUS LI-RADS. The modified LI-RADS scores using AMRI with SSAP showed a high concordance rate with the conventional LI-RADS score using full-protocol MRI. The recall rate significantly decreased when the HCC surveillance and diagnosis strategy was changed from strategy 1 (AMRI without SSAP; surveillance then recall test) to strategy 2 (AMRI with SSAP; simultaneous surveillance and diagnosis).INTRODUCTION
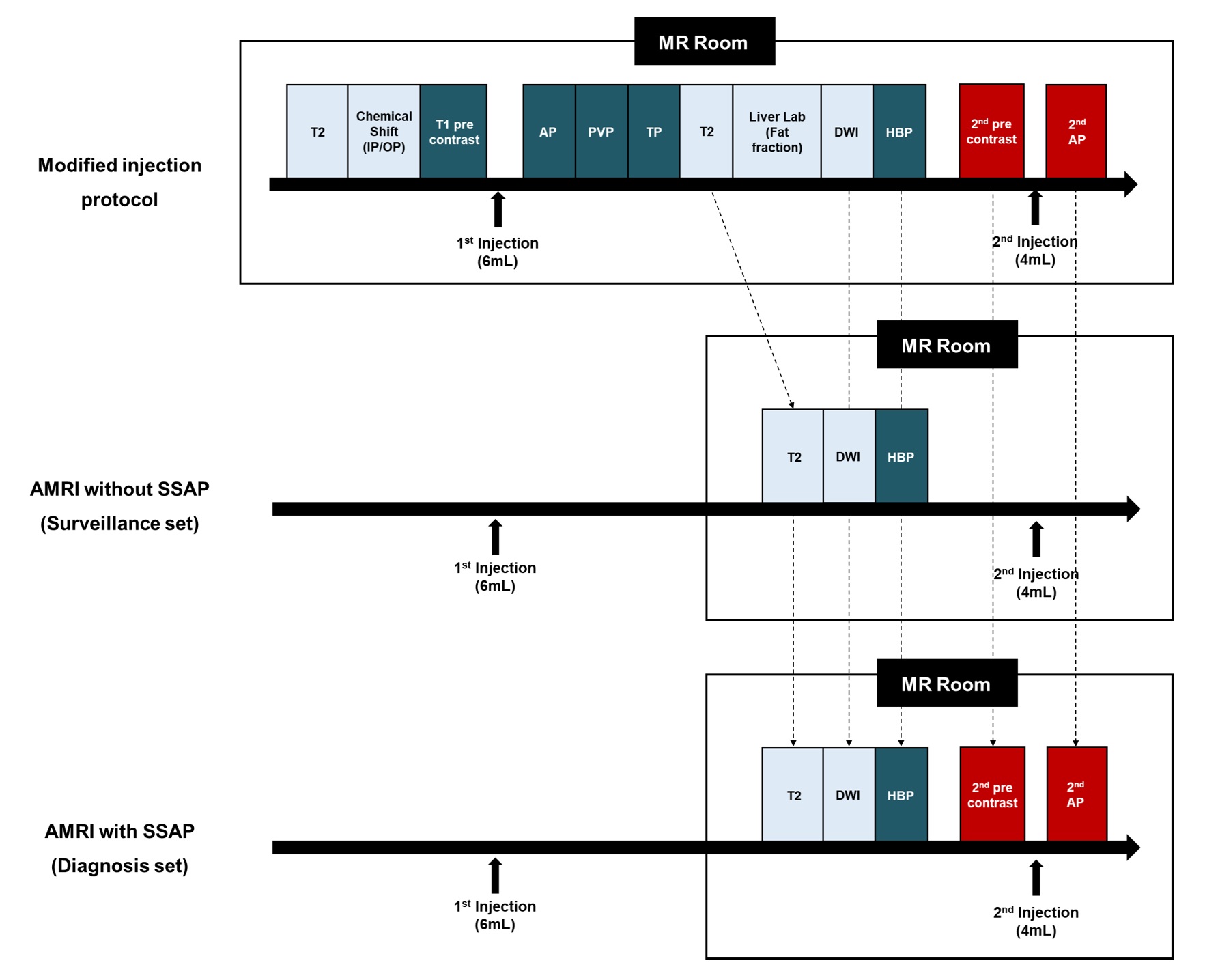
Although dynamic contrast-enhanced CT and MRI are widely used imaging modalities for the HCC diagnosis, the applicability of CT and MRI as surveillance tools for patients with cirrhosis is controversial from a health economic perspective1. There have been several studies that use various abbreviated MRI (AMRI) strategies in the HCC surveillance in patients with cirrhosis1-9.In our institution, a modified injection protocol was developed to overcome arterial phase (AP) degradation, which consisted of routine dynamic imaging after a first injection of 6 ml and second shot AP (SSAP) imaging after a second injection of 4 ml. This modified injection protocol demonstrated that motion artifacts were reduced while maintaining vascularity in the SSAP images of patients with HCC and hepatic metastasis10-11.
If SSAP is combined with AMRI strategy, it may be more cost-effective as diagnosis can be made simultaneously with surveillance, which eliminates the need for additional recall tests. The aim of this study was to evaluate the feasibility of simulated AMRI with SSAP for HCC surveillance and diagnosis.
METHODS
PatientsThis retrospective study was approved by our Institutional Review Board, and the requirement for informed consent was waived. A total 129 consecutive patients (92 men and 37 women; mean age, 58.8 ± 11.4 years; age range, 37–82 years) underwent gadoxetic acid-enhanced MRI using a modified injection protocol for HCC evaluation from July 2017 to February 2018. The modified injection protocol consists of routine dynamic imaging (6-ml) and SSAP imaging (4-ml).
Image analysis
Two radiologists independently reviewed full-protocol MRI and two AMRI sets: AMRI without SSAP (surveillance set) and AMRI with SSAP (diagnosis set). To reduce recall bias, image interpretation was performed during three separate sessions with a 4-week interval and the images were randomly given to both reviewers.
1) First session: Full-protocol MRI
In the full-protocol MRI, both reviewers assigned observations according to conventional Liver Imaging Reporting and Data System (LI-RADS).
2) Second session: Surveillance set (AMRI without SSAP)
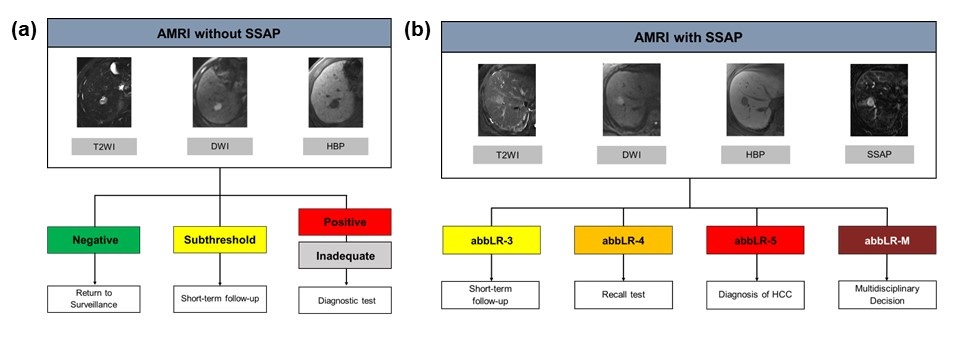
The surveillance set consists of T2-weighted image (T2WI), diffusion-weighted imaging (DWI), and HBP image (Figure 1). In the surveillance set, patients and lesions were assigned to four categories (negative, subthreshold, positive, and inadequate).
3) Third session: Diagnosis set (AMRI with SSAP)
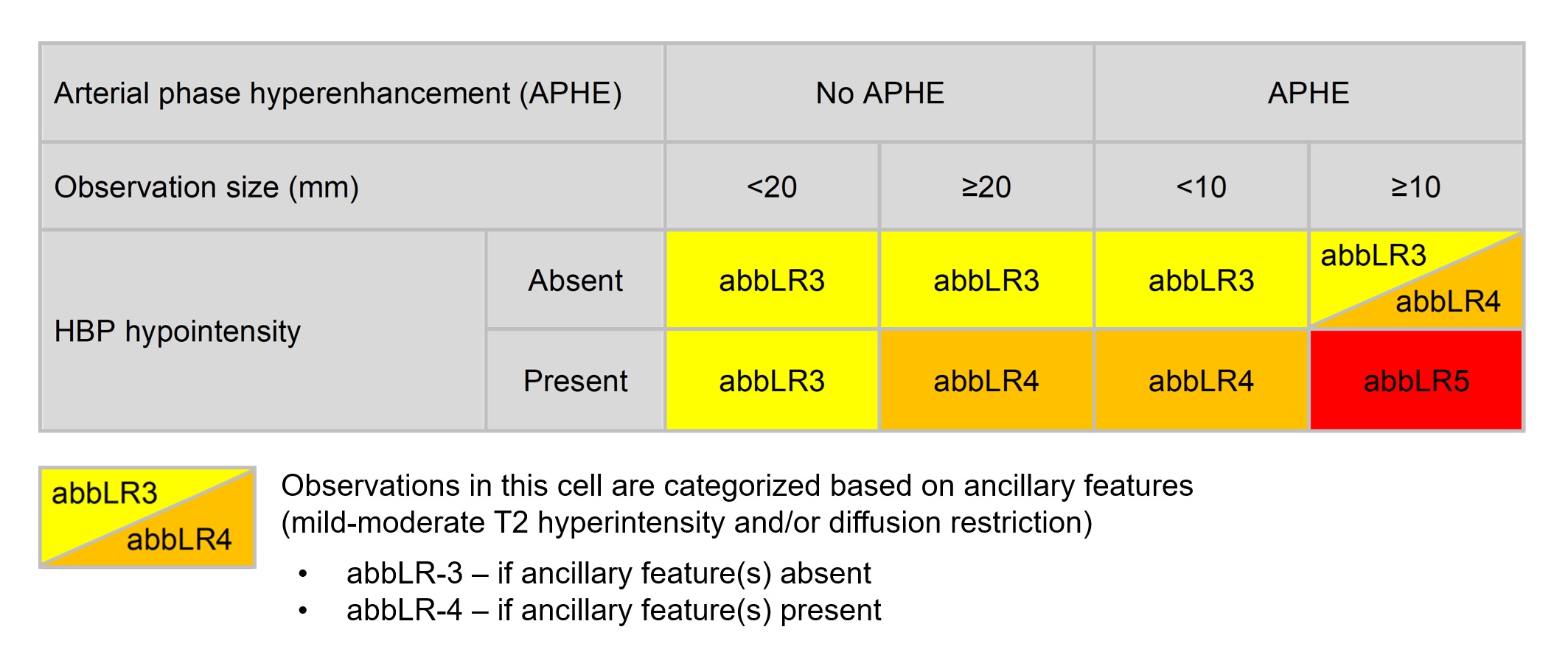
The diagnosis set consists of T2WI, DWI, HBP image, and SSAP image (Figure 1). In the diagnosis set, both reviewers additionally evaluated arterial phase hyperenhancement (APHE) using SSAP and its subtraction images. Because AMRI did not include portal venous and delayed (or transitional) phase images, washout and enhancing capsule could not be evaluated. Therefore, we devised a modified version of CT/MRI LI-RADS for the diagnostic algorithm using AMRI with SSAP by referring to CEUS LI-RADS (Figure 2). In the modified version of LI-RADS, observations were assigned from abbLR-3 to abbLR-5 according to observation size, APHE, and HBP hypointensity (Figure 2). Since the portal venous phase (PVP) was not included in AMRI with SSAP, HBP hypointensity was adopted as a major feature instead of washout appearance.
Recall strategy
In the strategy 1 (AMRI without SSAP), patients classified as negative are returned to surveillance, those classified as subthreshold are subject to short-term follow-up, and those classified as positive and inadequate are subject to recall tests (Figure 3a).
In the strategy 2 (AMRI with SSAP), patients classified as abbLR-3 are subject to short-term follow-up, those classified as abbLR-4 are subject to recall tests, those classified as abbLR-5 are confirmed with HCC, and those classified as abbLR-M are referred for multidisciplinary decision (Figure 3b).
RESULTS
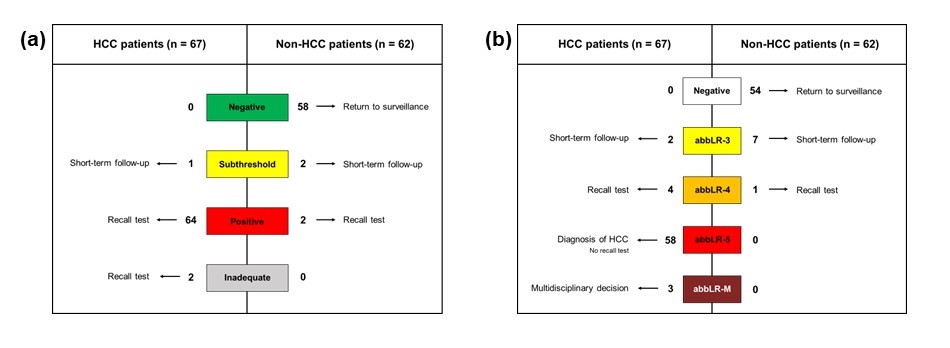
Sixty-seven patients with HCC and 62 patients without HCC were included. In the surveillance set, sensitivity and specificity for the detection of patients with HCC were 95.5% and 96.8%, and 94.0% and 96.8% in reviewer 1 and 2, respectively. In the diagnosis set, the scores of most HCCs (76/78, 97.4%) were consistent between LI-RADS of full-protocol and modified LI-RADS of AMRI with SSAP protocol. When the HCC surveillance and diagnosis strategy was changed from strategy 1 (AMRI without SSAP) to strategy 2 (AMRI with SSAP), the recall rate significantly decreased from 52.7% to 3.9% (p <0.001) (Figure 4a and 4b).DISCUSSION
In this study, we devised a modified version of LI-RADS using AMRI with SSAP. A previous study by Brunsing et al. introduced a structured reporting system for AMRI that classifies each examination into four categories (negative, subthreshold, positive, and inadequate) similar to US LI-RADS9. In our study, we devised a modified version of LI-RADS for AMRI with SSAP in which observations are categorized from abbLR-1 (definitely benign) to abbLR-5 (definitely HCC) using size, APHE, and HBP hypointensity, which is similar to CEUS LI-RADS.CONCLUSION
The modified LI-RADS score using the AMRI with SSAP demonstrated a high concordance rate with the LI-RADS score of the full-protocol MRI. The recall rate decreased when the HCC surveillance and diagnosis strategy was changed from a strategy of recall test after surveillance using AMRI without SSAP to a strategy of simultaneous surveillance and diagnosis with AMRI with SSAP. These results will enable AMRI with SSAP to diagnose HCC simultaneously with surveillance, which is expected to improve energy efficiency as well as cost-effectiveness.Acknowledgements
.References
1. Khatri G, Pedrosa I, Ananthakrishnan L et al. Abbreviated-protocol screening MRI vs. complete-protocol diagnostic MRI for detection of hepatocellular carcinoma in patients with cirrhosis: An equivalence study using LI-RADS v2018. J Magn Reson Imaging. 2020;51:415-425
2. Besa C, Lewis S, Pandharipande PV et al. Hepatocellular carcinoma detection: diagnostic performance of a simulated abbreviated MRI protocol combining diffusion-weighted and T1-weighted imaging at the delayed phase post gadoxetic acid. Abdom Radiol (NY). 2017;42:179-190
3. Chan MV, McDonald SJ, Ong YY et al.HCC screening: assessment of an abbreviated non-contrast MRI protocol. Eur Radiol Exp. 2019;3:49
4. Whang S, Choi MH, Choi JI, Youn SY, Kim DH, Rha SE. Comparison of diagnostic performance of non-contrast MRI and abbreviated MRI using gadoxetic acid in initially diagnosed hepatocellular carcinoma patients: a simulation study of surveillance for hepatocellular carcinomas. Eur Radiol. 2020;30:4150-4163
5. Vietti Violi N, Lewis S, Liao J et al. Gadoxetate-enhanced abbreviated MRI is highly accurate for hepatocellular carcinoma screening. Eur Radiol. 2020;30:6003-6013
6. Lee JY, Huo EJ, Weinstein S et al. Evaluation of an abbreviated screening MRI protocol for patients at risk for hepatocellular carcinoma. Abdom Radiol (NY). 2018;43:1627-1633
7. Marks RM, Ryan A, Heba ER et al. Diagnostic per-patient accuracy of an abbreviated hepatobiliary phase gadoxetic acid-enhanced MRI for hepatocellular carcinoma surveillance. AJR Am J Roentgenol. 2015;204:527-535
8. Tillman BG, Gorman JD, Hru JM et al. Diagnostic per-lesion performance of a simulated gadoxetate disodium-enhanced abbreviated MRI protocol for hepatocellular carcinoma screening. Clin Radiol. 2018;73:485-493
9. Brunsing RL, Chen DH, Schlein A et al. Gadoxetate-enhanced Abbreviated MRI for Hepatocellular Carcinoma Surveillance: Preliminary Experience. Radiol Imaging Cancer, 2019;1:e190010
10. Park YS, Lee J, Kim JW, Park CM, Lee CH. Second shot arterial phase to overcome degraded hepatic arterial phase in liver MR imaging. Eur Radiol. 2019;29:2821-2829
11. Kim JW, Lee CH, Park YS, Lee J, Kim KA. Abbreviated Gadoxetic Acid-enhanced MRI with Second-Shot Arterial Phase Imaging for Liver Metastasis Evaluation. Radiol Imaging Cancer. 2019;1:e190006
Figures