0782
An advanced reconstruction framework in stack-of-stars golden-angle radial non-contrast enhanced 4D MRA with ultra-high temporal resolution
Tianrui Zhao1,2, Li Feng3, and Lirong Yan2
1Department of Biomedical Engineering, Northwestern University, Chicago, IL, United States, 2Department of Radiology, Northwestern University, Chicago, IL, United States, 3BioMedical Engineering and Imaging Institute (BMEII), Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States
1Department of Biomedical Engineering, Northwestern University, Chicago, IL, United States, 2Department of Radiology, Northwestern University, Chicago, IL, United States, 3BioMedical Engineering and Imaging Institute (BMEII), Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
Keywords: Blood vessels, Image Reconstruction
In the present study, we developed an advanced reconstruction framework for ASL-based 4-dimensional (4D) MRA dubbed GraspMRA, which combines stack-of-stars golden-angle radial sampling with low-rank subspace-based image reconstruction to achieve ultra-high temporal resolution. The performance of GraspMRA was evaluated by comparison with three other reconstruction methods at different acceleration rates. Our results have demonstrated that GraspMRA has superior performance to the other methods, and it provides real flow dynamics at an ultra-high temporal resolution of up to 25ms per 3D volume while preserving good image quality.
Introduction
Characterization of fast flow events in cerebrovascular disorders, such as arteriovenous fistula and aneurysm, is desired in clinical practice1,2. Recently developed arterial spin labeling (ASL) based time-resolved 4-dimensional MR angiography3,4 (4D MRA) shows promise in delineating the dynamic blood flow through the intracranial vasculature with high spatial (1mm) and temporal resolution (100ms), specially equipped with stack of stars golden-angle radial acquisition and sparsity constraint image reconstruction. However, the image quality dramatically drops using the previously developed reconstruction methods when pursuing a higher temporal resolution. Recently, we have introduced a subspace-based reconstruction in 4D MRA, however, the performance remains limited at a higher acceleration rate. In this work, we aim to develop an advanced and reliable subspace-base reconstruction framework in accelerated 4D MRA named GraspMRA by incorporating a self-calibrating low-rank subspace-based model. Specifically, the temporal basis for subspace reconstruction is estimated from the centers of stack-of-stars k-space.Methods
MRI data acquisitionThe MRI scans were performed on a 3T Prisma MR scanner (Siemens) using a 20-channel head coil. 4D MRA data were acquired by combining a pulsed ASL preparation with golden-angel radial stack-of star 3D bSSFP readout sequence5. The key parameters in the imaging protocol included: field of view = 256x256x48 $$$mm^{3}$$$; TR/TE = 4.86/2.43ms; bandwidth = 814 Hz/pixel; flip angle = 25 degree; spatial resolution = 1x1x1.5 $$$mm^{3}$$$; 36 slices with each slice having 500 radial spokes, scan time of 3 min.
Image reconstruction
The reconstruction workflow of GraspMRA is shown in Figure 1. In the first step, the temporal basis $$$U\in C^{T\times T}$$$ is estimated by extracting the central point of k-space and being integrated into groups for matching the target temporal resolution (total spoke number/spoke number used for reconstruction per frame). The principal component analysis is then applied to get and sort the key temporal features. To accelerate the image reconstruction, K dominant basis $$$U_{k}\in C^{T\times K}$$$ is picked over full temporal basis in the second step, and the image is decomposed into two compartments as temporal basis $$$U_{k}$$$ and spatial basis $$$V_{k}\in C^{K\times N^{2}}$$$. In the third step, the optimization problem is now aimed for spatial basis $$$V_{k}$$$ instead of the full image. The spatial and temporal sparsity are considered for total variation constraint, and the corresponding penalty weights are $$$\lambda_{1}$$$=0.0001, $$$\lambda_{2}$$$=0.001. The label and control images are reconstructed simultaneously to maintain the correct image correlations. In the last step, the images are reconstrued with the composition of the optimized spatial basis $$$\widetilde{V_{k}}$$$ and temporal basis $$$U_{k}$$$.
GraspMRA reconstruction was performed three times for each raw date with 5, 10, and 20 spokes per time frame. Conventional sub-space reconstruction (GRASP-pro)6, standard GRASP reconstruction with temporal constraint, and Non-Uniform Fast Fourier Transform (NUFFT) were also applied for quality comparison. After reconstruction, maximum intensity projection (MIP) was conducted on the subtraction of reconstructed control and label images to display blood flow dynamics.
Results & Discussion
Figure 2 shows several representative frames of MIP images and the collapsed MIP (cMIP) across frames reconstructed with 10 spokes per frame (acceleration factor = 50) using the proposed GraspMRA, GRASP-pro, GRASP, and NUFFT. The proposed GraspMRA outperformed GRASP and NUFFT with significantly less noise and streaking artifacts. Compared to GRASP-pro, the proposed GraspMRA offered improved image quality with reduced overall noise level and better visualization of fine vessel structures as indicated by arrows while the computational time was reduced by approximately 1/2.Figure 3 shows several MIP dynamic images and cMIP image reconstructed using GraspMRA with 5, 10, and 20 spokes per frame, corresponding to the temporal resolution of 25ms, 50ms, and 100ms, respectively. The image quality with different spoke numbers looked comparable in preserving the integrity of vascular structures.
Figure 4 shows the signal intensity time course of GraspMRA images in 4 selected ROI regions in the middle cerebral arteries (MCA) and posterior cerebral arteries (PCA) with 5, 10, and 20 spokes per frame. The time courses from 10-spoke NUFFT reconstructed images were used as reference for dynamic information. The time courses of GraspMRA at 5, 10, and 20 spokes showed no obvious temporal shifts or blur compared to the NUFFT dynamics, suggesting that GraspMRA can reveal the actual temporal dynamics even with a higher acceleration factor (5 spokes per frame).
GraspMRA also demonstrated good image quality in the original label and control images. Figure 5 shows the slice-wise comparison for label and control images at 5,10, and 20 spokes. All label and control images presented good image quality without visible streaking artifacts or noise in either case.
Conclusion
This work has demonstrated the feasibility of GraspMRA--an advanced reconstruction framework in 4D MRA, which employs self-calibrating temporal basis estimation in the low-rank subspace-based reconstruction to achieve an ultra-high temporal resolution while preserving good image quality. GraspMRA could be a potentially useful 4D MRA technique in clinical applications to characterize fast-flow events.Acknowledgements
This work is supported by grants of NIH R01NS118019, RF1AG072490, and BrightFocus Foundation A20201411S.References
- Willinsky RA, Taylor SM, TerBrugge K, Farb RI, Tomlinson G, Montanera W. Neurologic complications of cerebral angiography: prospective analysis of 2,899 procedures and review of the literature. Radiology. 2003 May;227(2):522-8.
- Yu S, Yan L, Yao Y, Wang S, Yang M, Wang B, Zhuo Y, Ai L, Miao X, Zhao J, Wang DJ. Noncontrast dynamic MRA in intracranial arteriovenous malformation (AVM): comparison with time of flight (TOF) and digital subtraction angiography (DSA). Magnetic resonance imaging. 2012 Jul 1;30(6):869-77.
- Zhou Z, Han F, Yu S, Yu D, Rapacchi S, Song HK, Wang DJ, Hu P, Yan L. Accelerated noncontrast‐enhanced 4‐dimensional intracranial MR angiography using golden‐angle stack‐of‐stars trajectory and compressed sensing with magnitude subtraction. Magnetic resonance in medicine. 2018 Feb;79(2):867-78.
- Song HK, Yan L, Smith RX, Xue Y, Rapacchi S, Srinivasan S, Ennis DB, Hu P, Pouratian N, Wang DJ. Noncontrast enhanced four‐dimensional dynamic MRA with golden angle radial acquisition and K‐space weighted image contrast (KWIC) reconstruction. Magnetic resonance in medicine. 2014 Dec;72(6):1541-51.
- Yan L, Wang S, Zhuo Y, Wolf RL, Stiefel MF, An J, Ye Y, Zhang Q, Melhem ER, Wang DJ. Unenhanced dynamic MR angiography: high spatial and temporal resolution by using true FISP–based spin tagging with alternating radiofrequency. Radiology. 2010 Jul;256(1):270.
- Feng L, Wen Q, Huang C, Tong A, Liu F, Chandarana H. GRASP‐Pro: imProving GRASP DCE‐MRI through self‐calibrating subspace‐modeling and contrast phase automation. Magnetic resonance in medicine. 2020 Jan;83(1):94-108.
Figures
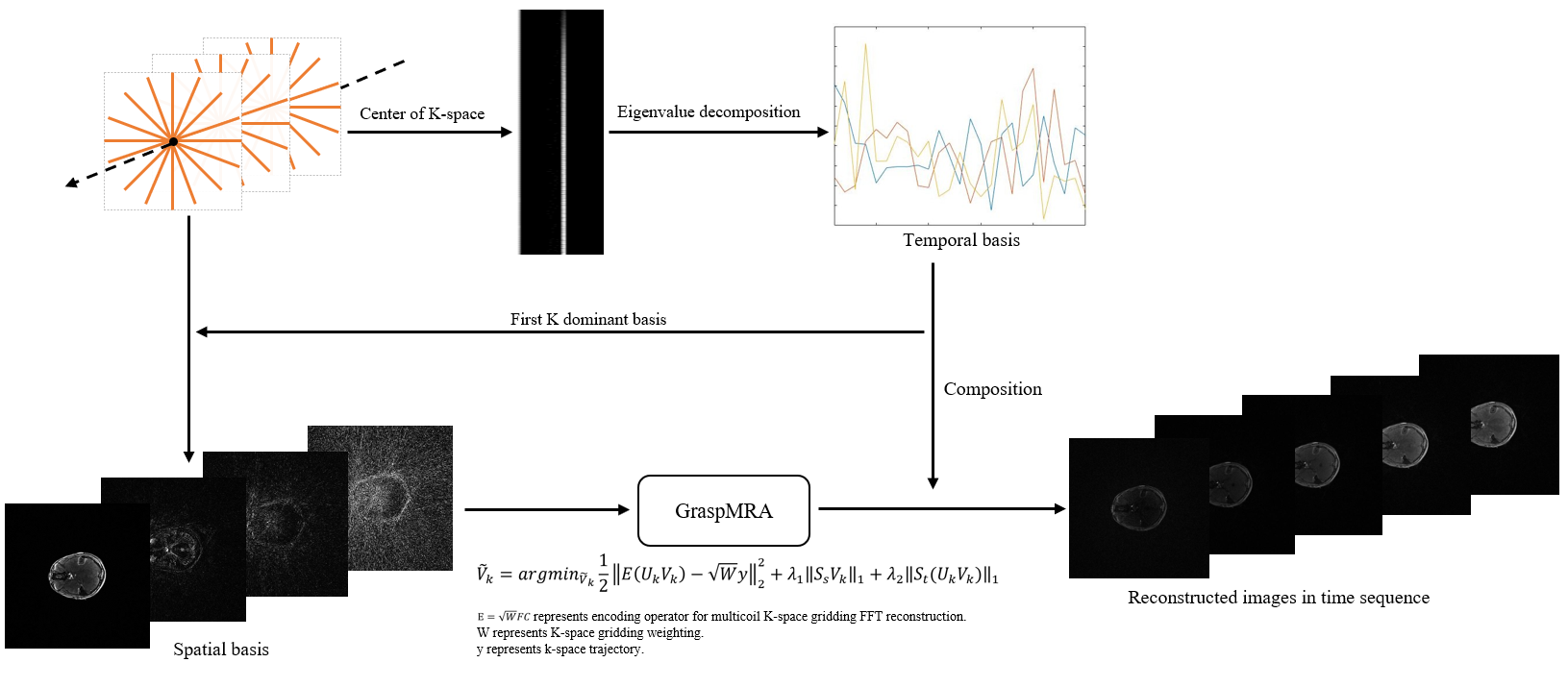
Figure 1. Flowchart of the
image reconstruction of GraspMRA.
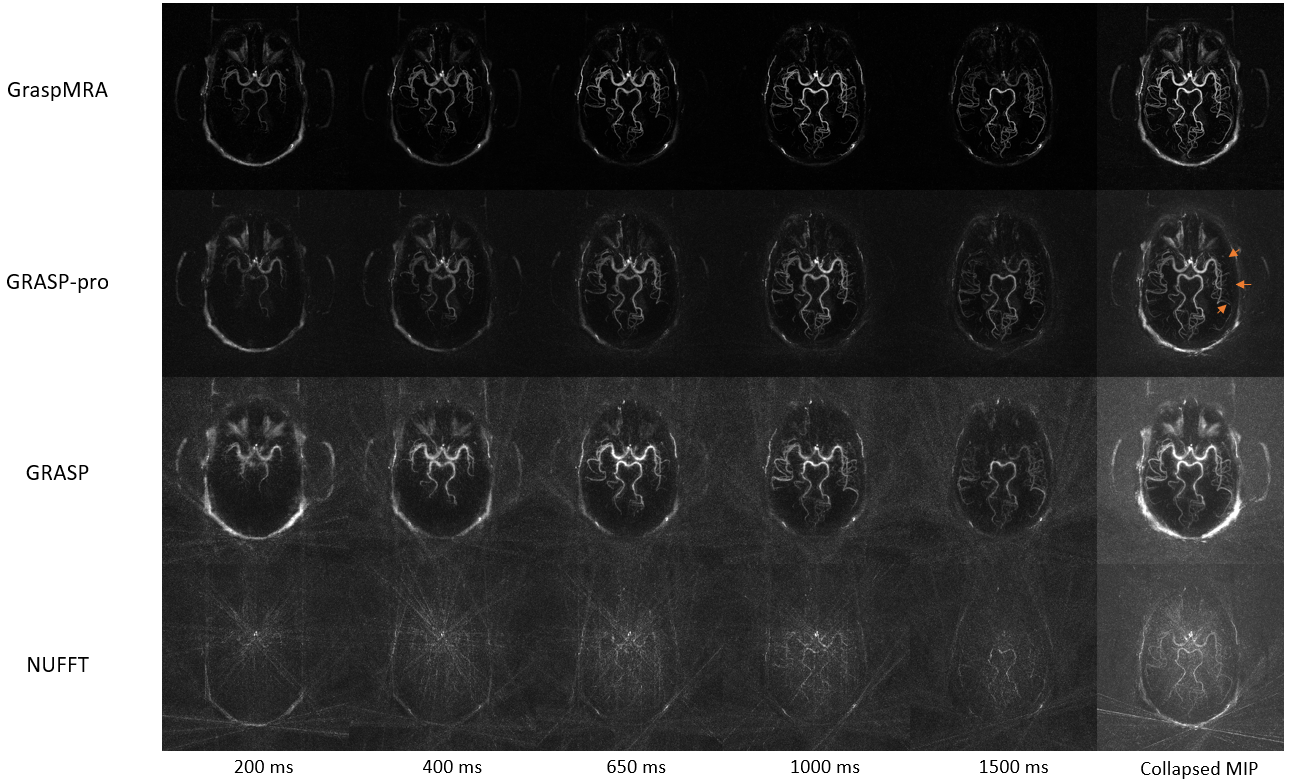
Figure 2. MIP images of
selected frames and collapsed MIP image over phases reconstructed with 10
spokes per frame using GraspMRA, GRASP-pro, GRASP, and NUFFT.
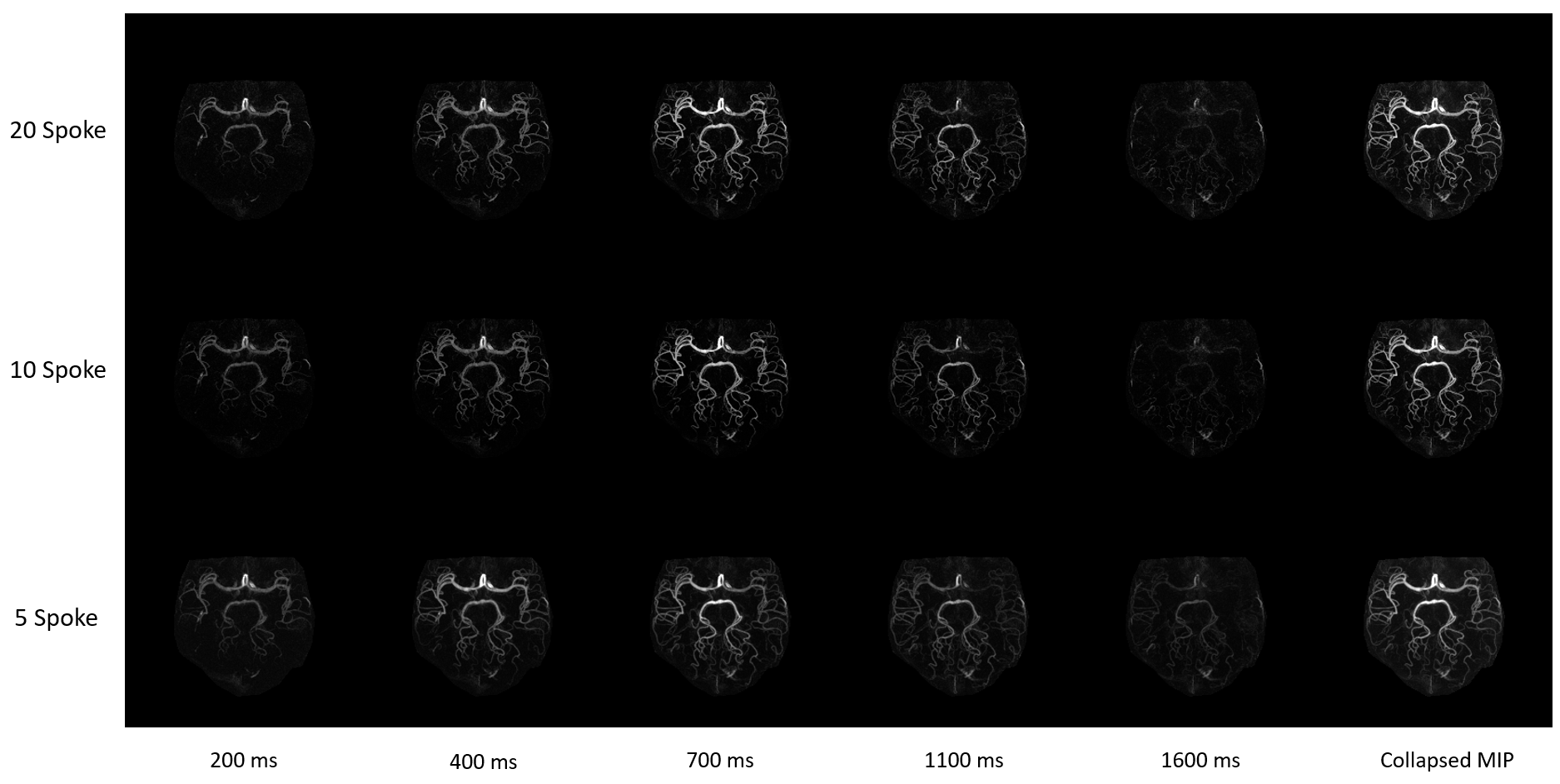
Figure 3. MIP images of
selected frames and collapsed MIP image over phases reconstructed using
GraspMRA with 20, 10 and 5 spokes per frame, respectively.
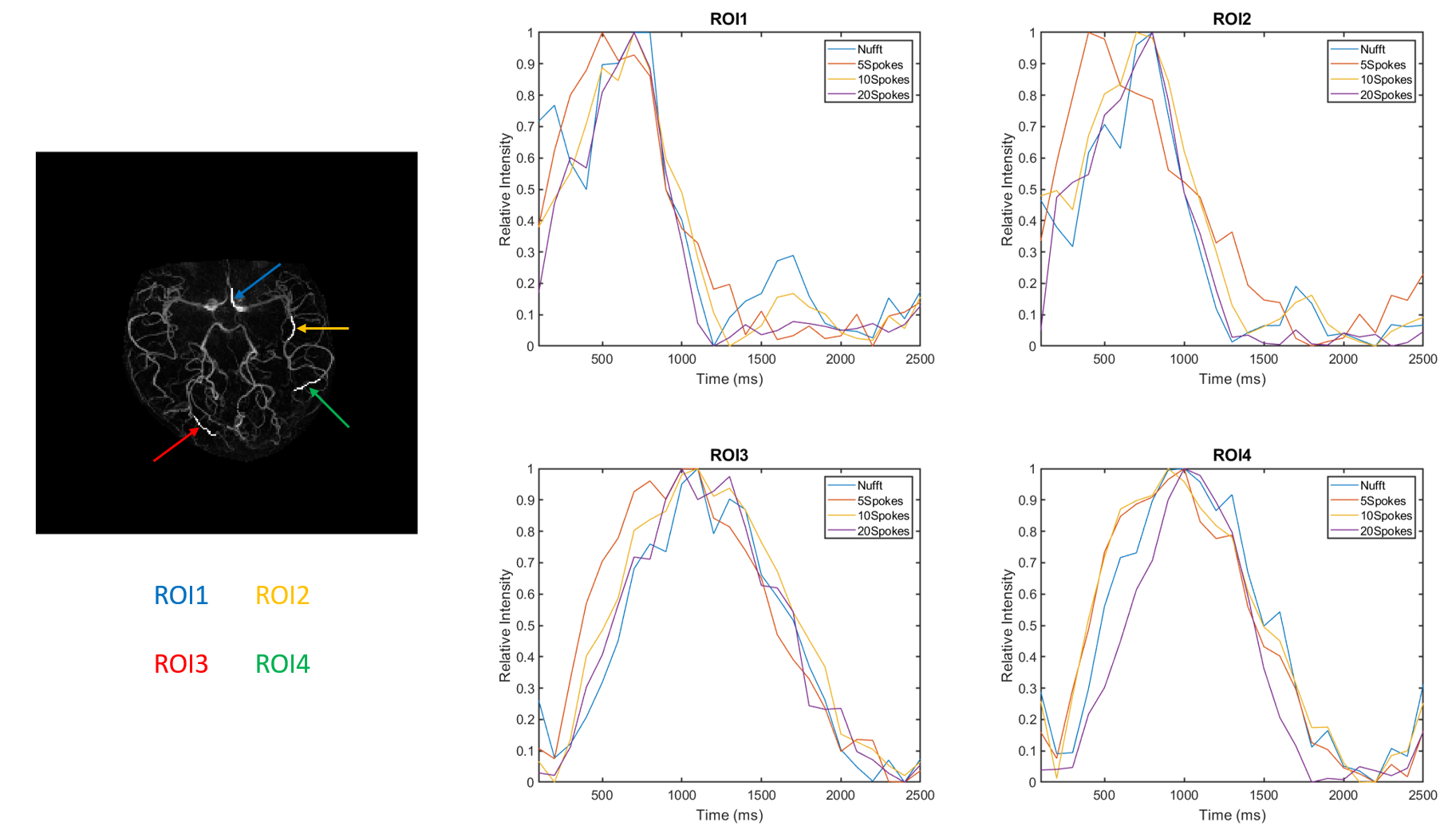
Figure 4. Signal intensity
time courses of GraspMRA with 20, 10, and 5 spokes extracted from 4 selected
ROIs in MCA and PCA. The time courses of 10-spoke NUFFT images were used as a
reference for flow dynamics.
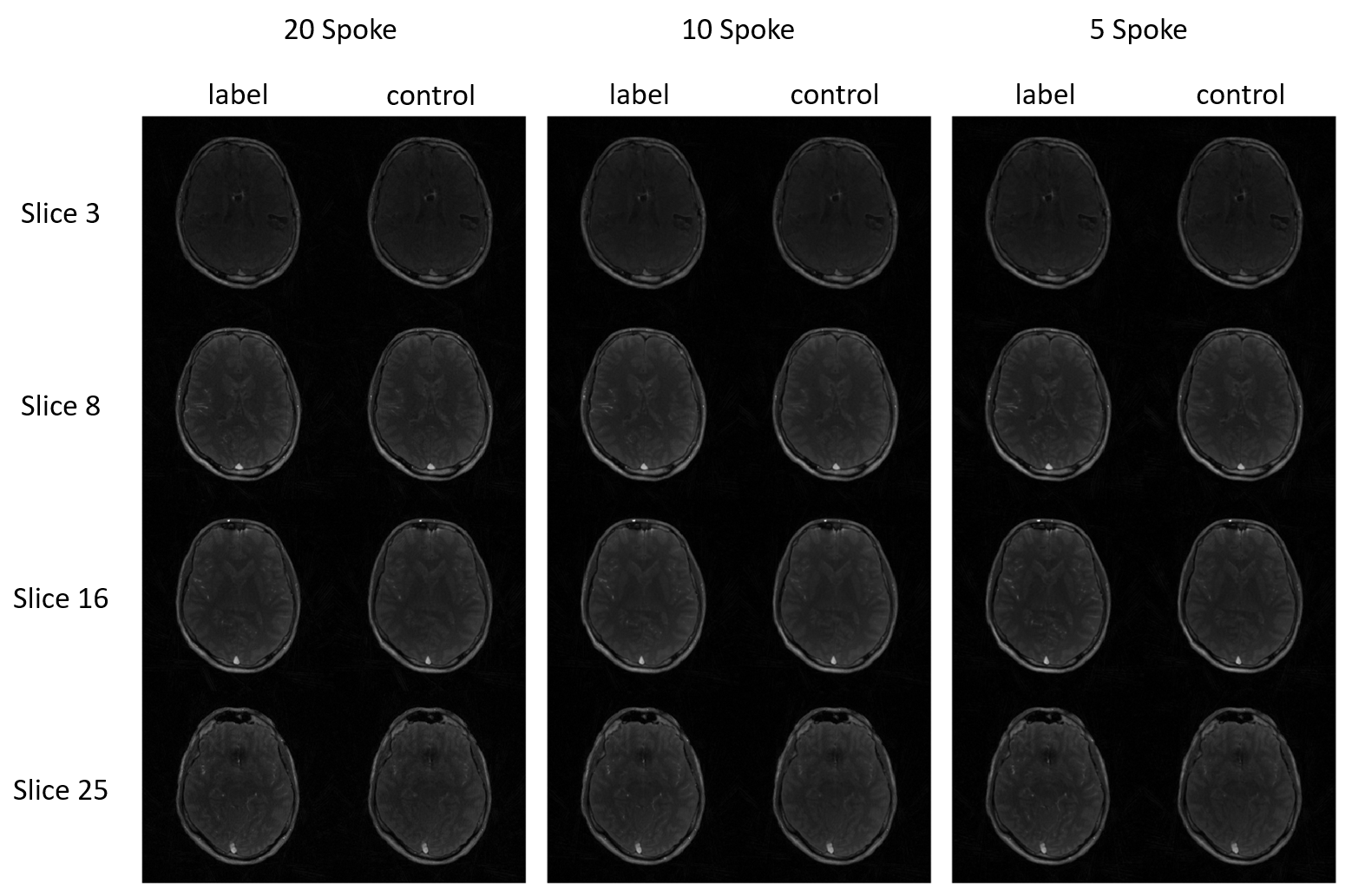
Figure 5. Selected label
and control images reconstructed by GraspMRA with 20, 10 and 5 spokes,
respectively.
DOI: https://doi.org/10.58530/2023/0782