0723
Stereotactic MR-guided Adaptive Radiotherapy for Pancreatic Cancers on a 1.5 Tesla MR-linac system
Danny Lee1,2, Seungjong Oh1,2, Min-Sig Hwang1,2, Daniel Pavord1, Jason Sohn1,2, Athanasios Colonias1, Mark Trombetta1, Alexander Kirichenko1,2, and Paul Renz1
1Allegheny Health Network, Pittsburgh, PA, United States, 2Drexel University College of Medicine, Philadelphia, PA, United States
1Allegheny Health Network, Pittsburgh, PA, United States, 2Drexel University College of Medicine, Philadelphia, PA, United States
Synopsis
Keywords: Cancer, Pancreas, MR-guided pancreas SBRT on MR-Linac
Ablative SBRT to pancreatic cancers on MRI-Linac is a novel and rapidly evolving technology allowing real-time visualization of tumor and nearby organs-at-risk (OAR). Reliable identification of pancreas tumors on MR-Linac has direct impact on radiotherapy planning and outcome. A novel workflow was clinically implemented for pancreas stereotactic body radiotherapy on Elekta Unity MR-Linac. Compared to T2W images, pancreas tumors on T1W images, were superiorly visible for accurate delineation during the entire treatment course. This study is the first to determine the impact of an optimized MR sequence for pancreas tumors and OARs during multi-fractionate MR-guided radiotherapy on 1.5T Elekta MR-Linac.INTRODUCTION
A high field MRI combined with a linear accelerator (a 1.5T Elekta MR-Linac, Elekta; Stockholm, Sweden) is a prominent technique that shows promise in stereotactic MRI-guided adaptive radiation therapy for pancreatic cancers (pancreas-SBRT). The feasibility of pancreas-SBRT using an abdominal compression belt has been undertaken and investigated the impact of intra-fraction target motion on the dose of Eletka MR-linac treatment plans.1 The previous study utilized the pre-set T2W MRI sequence provided by Elekta and the contours of organs at risk (OARs) propagated fraction-to-fraction using Monaco deformable image registration (DIR) algorithm and edited by the physician and planners within a 2 cm ring during online adapt-to-shape (ATS) plan adaptation, limited the pancreatic tumor visualization on T2W images and the DIR-based contour propagation of OARs across fractionated pancreas-SBRT. Hence, this study proposed (1) a T1W sequence to improve the visualization of pancreatic tumors OARs for fast and accurate contouring for increasing/decreasing the dose to the PTV and OARs during multi-fractionated pancreas-SBRT.METHODS
Twenty one patients with 16 pancreatic cancers, 2 left adrenal glands and 3 lymph nodes (i.e., peri-aotic and aortacaval) completed a CT simulation followed by an MR simulation on the same day, and underwent multi-fractionated pancreas-SBRT every other day. For abdominal imaging, a T1W 3D TFE (Turbo Field Echo) MR pulse sequence in a 1.5T Unity Philips MR-Linac with two MR receiver coils (a 4 channel anterior coil and a 4 channel posterior coil) was used and typical imaging parameters were TR/TE = 4.5/2.2 ms, FOV = 400 × 400 mm2, pixel size = 1.1 × 1.1 mm2 and image matrix = 280 × 280, thickness = 2 mm, flip angle = 10o, bandwidth = 383 Hz and number of signal average = 5. Each MR image set contains 161 images and total acquisition time is approximately 80 seconds. In each fraction of pancreas-SBRT, a plan-MR image set was acquired for online adapt-to-position (ATP) and ATS plan adaption, and verification-MR and post-MR were also acquired before and after the beam delivery to verify patient setup. The workflow of multi-fractionated pancreas-SBRT is shown in Fig 1. Fig 1. The workflow of multi-fractionated pancreas-SBRT on Elekta MR-Linac. (a) Patient selection with pancreatic cancers and 1st MR screening to check the eligibility of each patient, (b) CT and MR simulations with an abdominal compression belt to acquire CT and MR image sets, (c) contouring OARs on CT images and targets on MR images for developing a CT or MR reference plan, and (d) MR-guided pancreas-SBRT in 3 – 5 fractions on MR-Linac. An identical unity couch top and the same abdominal compression belt were used in CT and MR simulations, and across all fractions. Fig 2. An example of pancreas tumors on the three images of (a) CT + Gadolinium with FB, (b) T2W with NAV, and (c) T1W with FB. The yellow contour indicates the target tumor region. Pancreas tumors were visually identified to evaluate the improvement of tumor visualization on T1W images compared to T2W images.RESULTS
Compared to a T2W image (Fig 2(b)), the boundary of pancreas tumors in all 12 patients is clearly shown on a T1W image (Fig 2(c)). Similarly, the visualization of pancreas tumors and OARs was maintained across all fractions, resulted in fast and accurate delineation of target tumor volumes and OARs in each fraction. An average of the time consumed in 12 patients was about 55 and 79 minutes in ATP and ATS, respectively. The most time consuming steps are (1) fusion and contouring, and (2) beam delivery (25 Gy to 45 Gy in 3 – 5 fractions with 7 – 13 beams).DISCUSSION
Online treatment plan adaptation requires superior tumor visualization for delineating fast and accurate targets and OARs. We utilized a motion averaged T1W image (less than 80 s) which can shorten the imaging time of plan-, verification- and post-MR(s) more than 2.5 times, compared to a T2W image without/with navigation (up to 360 s). In addition, tumor visibility (Figure 2(c)) can (1) minimize delineation uncertainty, (2) reduce treatment planning target volume and (3) spare OAR(s) during MR-guided pancreas-SBRT.CONCLUSIONS
This was the first study that we utilized an optimized T1W sequence to improve pancreatic tumor visualization for adaptive planning on the 1.5T Elekta Unity MR-Linac. Tumor boundaries were clearly visible for delineation of targets and OAR(s). Our results can facilitate consistent visibility of pancreatic tumors to achieve fast and accurate MR-guided pancreas-SBRT.Acknowledgements
We thank the physicians, therapists, physicists, nurses, dosimetrists and staff at the Allegheny Health Network and Department of Radiation Oncology for continuous support.References
(1) Neelam T, et al., Physics and Imaging in Radiation Oncology (2021), 19:53–59.
(2) Luterstein, E., et al., Cureus (2018), 10(3).
(3) Boye D, et al., Acta radiologica open (2015), 4(6):2058460115589124.
Figures
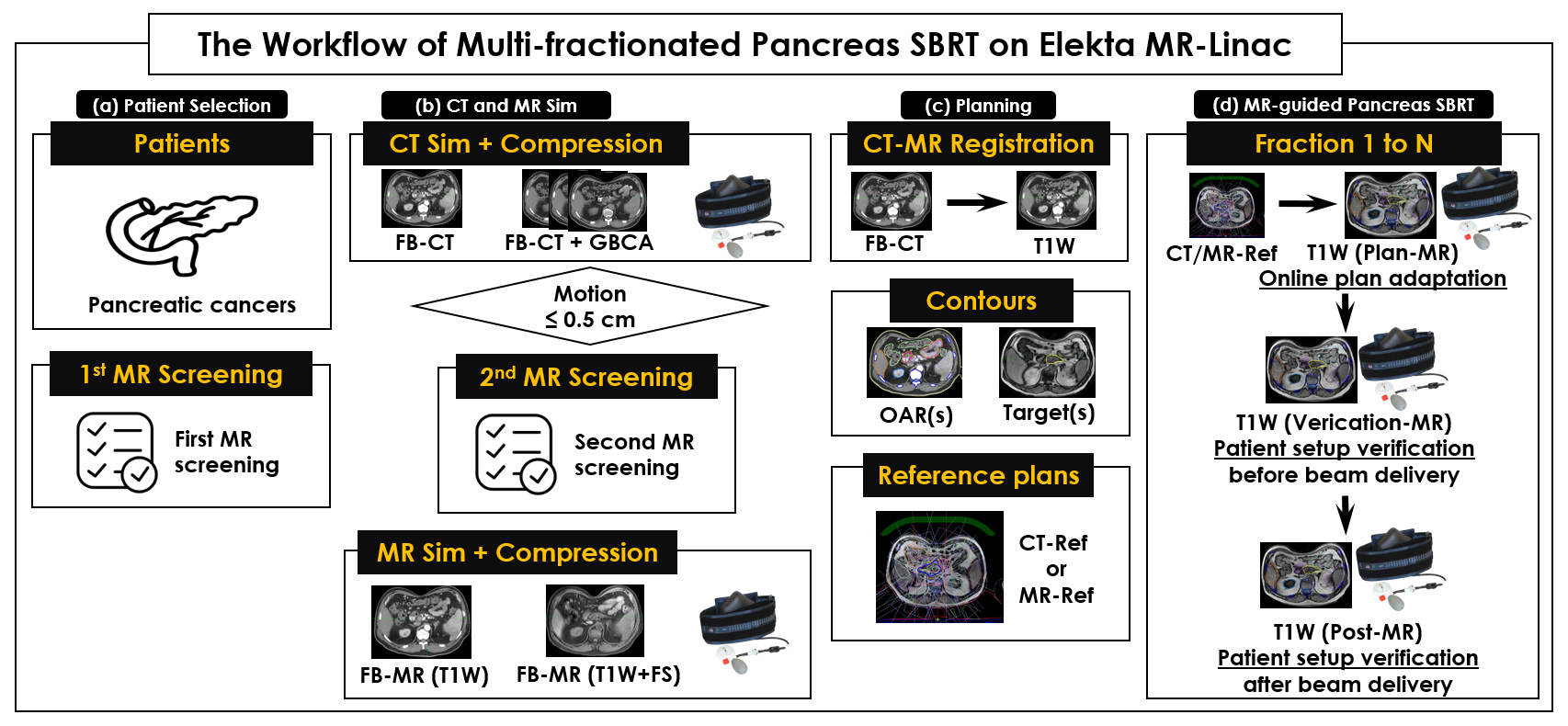
Fig 1. The workflow of multi-fractionated pancreas-SBRT on Elekta MR-Linac.
(a) Patient selection with pancreatic cancers and 1st MR screening
to check the eligibility of each patient, (b) CT and MR simulations with an
abdominal compression belt to acquire CT and MR image sets, (c) contouring OARs
on CT images and targets on MR images for developing a CT or MR reference plan,
and (d) MR-guided pancreas-SBRT in 3 – 5 fractions on MR-Linac. An identical
unity couch top and the same abdominal compression belt were used in CT and MR
simulations, and across all fractions.
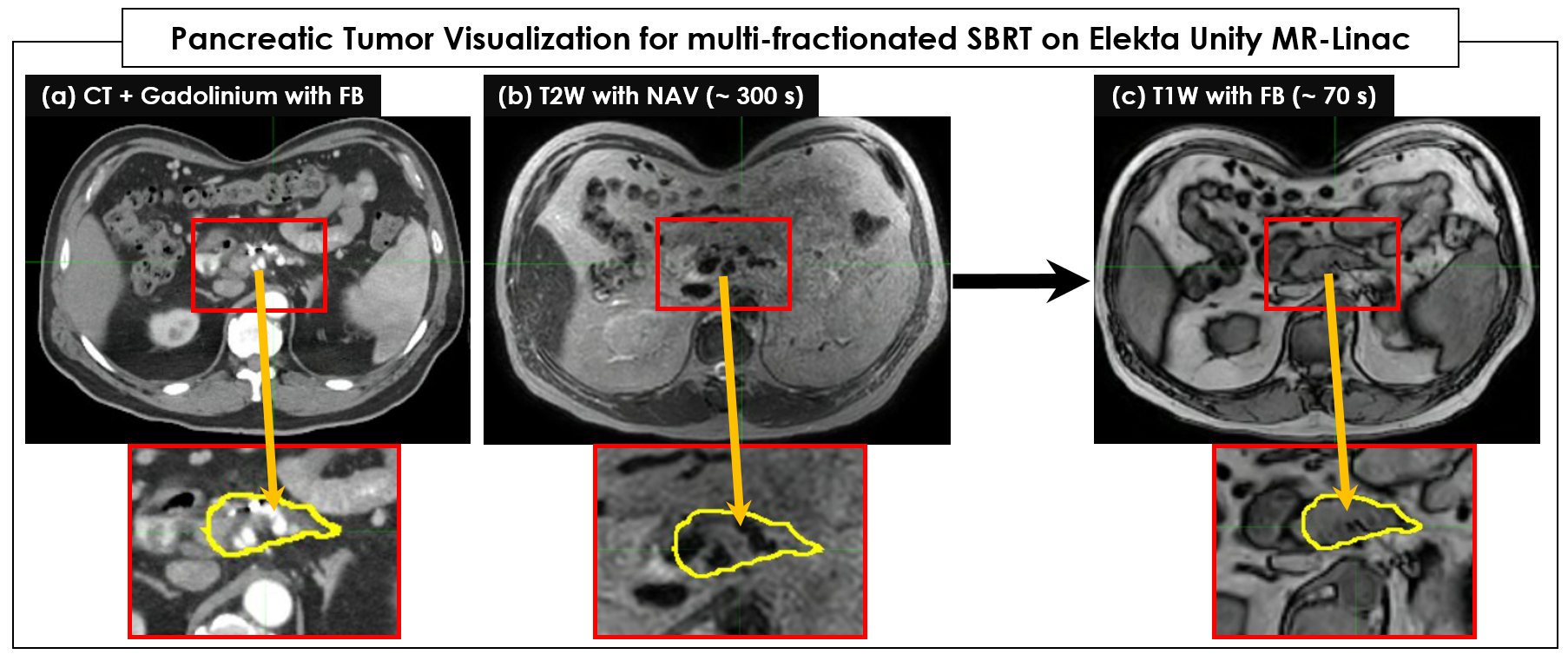
Fig
2.
An example of pancreas tumors on the three images of (a) CT + Gadolinium with
FB, (b) T2W with NAV, and (c) T1W with FB. The yellow contour indicates the
target tumor region.

Table
1. The time consumed in online
ATP/ATS pancreas-SBRT across 10 steps. The verification-MR was acquired during
plan optimization.
DOI: https://doi.org/10.58530/2023/0723