0707
The Fuzzy MAD Stroke Conjecture, using Fuzzy C Means to classify Multimodal Apparent Diffusion for stroke stratification1Radiology, University of Illinois at Chicago, Chicago, IL, United States, 2Medical Imaging, Sun Yat-sen University Cancer Center, Guangzhou, China, 3Pathology, University of Illinois at Chicago, Chicago, IL, United States, 4Anatomy and Cell Biology, University of Illinois at Chicago, Chicago, IL, United States, 5Radiology, Fujian Medical University Union Hospital, Fuzhou, China, 6Bioengineering, University of Illinois at Chicago, Chicago, IL, United States
Synopsis
Keywords: Stroke, Diffusion/other diffusion imaging techniques
The ischemic stroke cascade is a complex menagerie of processes causing disruption of neuronal function and willful and/or reactive breakdown of the neural vascular unit (NVU), and, prevails to recovery, repair, or patient demise. To better understand the underpinnings of the stroke cascade we applied our Multimodal Apparent Diffusion (MAD) method to multi b‑value diffusion weighted magnetic resonance imaging, up to b‑value of 10K s/mm2, on 41 consecutive stroke patients. Using Fuzzy C Means we were able to discern 13 normal appearing tissue types and 16 lesion types. There are several findings that should be contemplated in current clinical imaging.
INTRODUCTION
The ischemic stroke cascade is a complex menagerie of processes, instigated by the disruption of blood supply to brain tissue, causing disruption of neuronal electrical function and willful and/or reactive breakdown of the neural vascular unit, and, prevails to recovery, repair, or patient demise depending on intrinsic, systemic, or external manipulation. The heterogeneity of lesions and limitations in imaging techniques has hindered our ability fully understand the stroke cascade. To better understand the underpinnings of the acute focal ischemic stroke cascade in vivo we applied our Multimodal Apparent Diffusion (MAD) method[1] to multi b‑value DWI, up to b‑value 10K s/mm2, on 41 acute focal ischemic stroke patients. Using Fuzzy C Means clustering technique, we were able to discern 13 normal appearing tissue / flow / fluid (NAM) tissue types and 18 lesion types.METHODS
This study was performed with IRB approval. Multi b-value diffusion weighted images of acute stroke patients (n=41, time from onset 1-17 days or 5±3.3 days) were acquired using 9 b‑values (0-10,000 s/mm2) over 4.5 minutes. The acquired diffusion data was processed using the MAD analysis method[1], briefly, the analysis results in flow (F, >3 μm2/ms), and, unimpeded (UI, ~3 μm2/ms) – viz fluid, hindered (H, 0.2-3 μm2/ms) – viz extracellular, and restricted (R, 0.2 μm2/ms) - viz intracellular, diffusion modes. Due to the limited number of b‑values collected the rate of flow is not reliable, and not used further.Fuzzy C Means takes a collection of voxels, with N MAD parameters, and determines each voxel’s memberships in M clusters, e.g., tissue/lesion types. A cluster’s N parameters are a best estimate of the MAD parameters for a theoretical homogeneous voxel of the cluster’s tissue/lesion type. The Fuzzy C Means method can be run iteratively to determine the most unique and precise set of clusters for a dataset, or using a predetermined set of clusters to analyze commonality among a population of datasets.
RESULTS
The MAD parameters within focal ischemic stroke lesions, as depicted in figure 1, shows the predominate lack of flow/fluid, spatial blurriness of parameters – cellular dedifferentiation, and abundance of restricted diffusion (fR) and the dichotomy of restricted diffusion coefficient (DR) between increased and decreased apparent diffusivity.The Fuzzy C Means clustering identified 13 types of NAM (3 GM, 4 WM, 3 flow, 3 fluid), and 18 types of lesions, see complete set of clusters in table 1. The majority normal appearing tissue (NAM) is loosely explained by extracellular space (fH ~70%) with an apparent diffusivity DH of about of 0.9 μm2/ms with a sizable amount (fR ~15%) of intracellular space with apparent diffusivity DR between about of 0.06 and 0.18 μm2/ms, where WM < GM, including noticeable amounts of fluid (fUR ~5%) and flow (fF ~5%). Two types of lesions are consistent with the FLAIR/Diffusion mismatch. Seven types of lesions are prevalent among most patient’s lesions.
Case 1 (figure 1/figure 2) – 63 yo male, 3 days after symptom onset with NIHSS of 4. This lesion’s voxels are predominantly of one lesion type. Apparent complete blockage of a large artery resulting in a medial anoxic epicenter, lesion5 – viz coagulative necrosis, juxtaposed with lesion8 – viz macrophages, and lesion10 – viz cellular debris, and collocated with the DWI‑FLAIR mismatch. The lesion radiates laterally toward normoxic tissue with decreasing severity of compromise and increasing amounts of edema, thru lesion3, lesion2, lesion6, lesion1, lesion7, lesion4 and finally to normal appearing GM2 at the pial surface. There are hints of excitotoxicity – viz lesion9, along the periphery of the lesion coincident with lesion4; with a notable void within the lesion proper.
Case 2 (figure 3/figure 4) – 64 yo male 5 days after symptom onset with NIHSS of 6. This lesion’s voxels contain one or more lesion types. A stroke lesion with an epicenter, lesion5 – viz coagulative necrosis, progressing posterolaterally with cellular demise/debris – viz lesion10/C30 and macrophages – viz lesion8, and progressing from epicenter anteromedially with increasing cellular survival. Excitotoxicity – viz lesion9, is seen in the most anteromedial portion of the lesion. Cellular debris – viz lesion10/C30 is undetected by DWI b0/b1000 and T2-FLAIR. Macrophages emanate from protruding blood vessels? Lesion maps, lesion3/2/6/MS, have lower than anatomically expected contrast in the anterolaterial direction from the identified ROI; suggestive of progression?
DISCUSSION
Given the latest understanding of the stroke cascade and MAD imaging, this study evaluated 41 consecutively examined/imaged acute stroke patients. Although the MAD parameters directly provides useful information about the stroke lesion, Fuzzy C Means was added to delve further inside the voxel to more precisely understand the heterogeneous microstructure involved. Each stage in the stroke cascade manifests in unique changes in the tissue at a cellular level that are reflected in MAD parameter signatures – viz cluster centers.CONCLUSION
As the data analyzed was a small number of clinical patients, without followup or contemporaneous histology, the finding, conclusions, and theorizing should be treated as conjecture, albeit there are several findings that may help in clinical management of stroke patients, and a couple that should be contemplated in current clinical imaging. Further investigation, with animal models and clinical studies, will help to consolidation of these conjectures.Acknowledgements
NIH grant R01AG061114References
[1] Damen FC, Scotti A, Damen FW, Saran N, Valyi-Nagy T, Vukelich M, Cai K. Multimodal apparent diffusion (MAD) weighted magnetic resonance imaging. Magn Reson Imaging. 2021 Apr;77:213-233. doi: 10.1016/j.mri.2020.12.007. Epub 2020 Dec 10. PMID: 33309925; PMCID: PMC7878401.
Figures
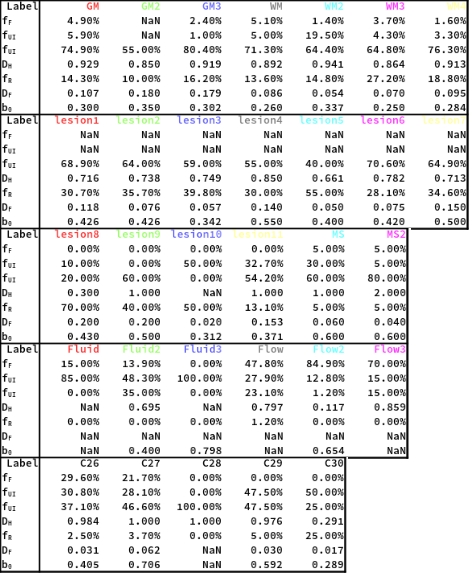
Table 1: Set of fuzzy clusters used to analyze, compare, and infer the underpinnings of the NAM, MS, and stroke lesions. Each block corresponds to a row in figures 2-4, save the last block, which contains minor lesions types. fF, fUI,fH, fR, are the fraction of a voxel explained by each MAD mode. DH, DR, are the diffusion coefficients for said MAD mode in units of μm2/ms. b0 is the normalize b0, i.e., T2, weighting. The value NaN serves as a wild card during clustering.
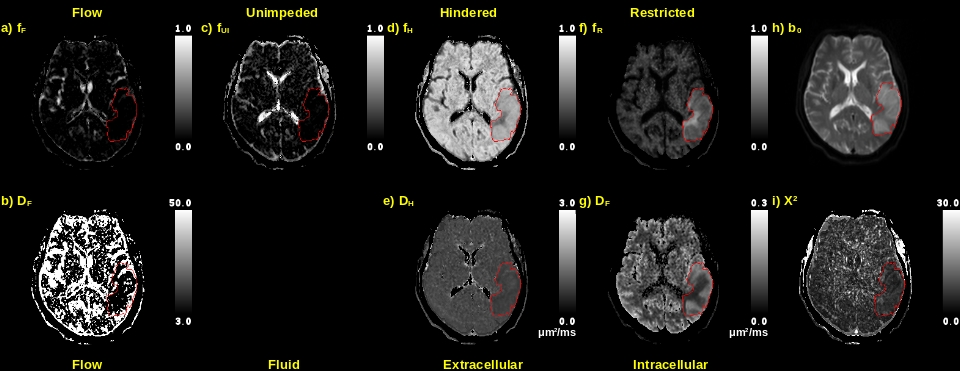
Figure 1: Case 1’s MAD mode maps. Top row are the fraction of the voxel explained by flow (F), and unimpeded (UI), hindered (H), and restricted (R) diffusion, respectively. Second row are the pseudo perfusion and hindered and restricted diffusivities. Last column are the b0 and chi squared fitting error. ROI was drawn around the lesion on the b1000 image. Note the lack of flow/fluid and cellular texture within the lesion, and the lack of correlation of fitting error to anatomy or lesion.
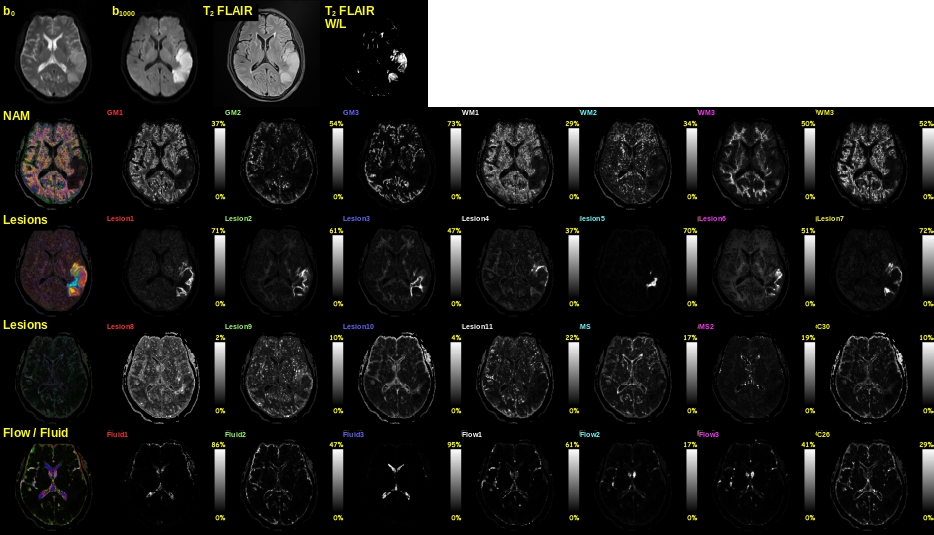
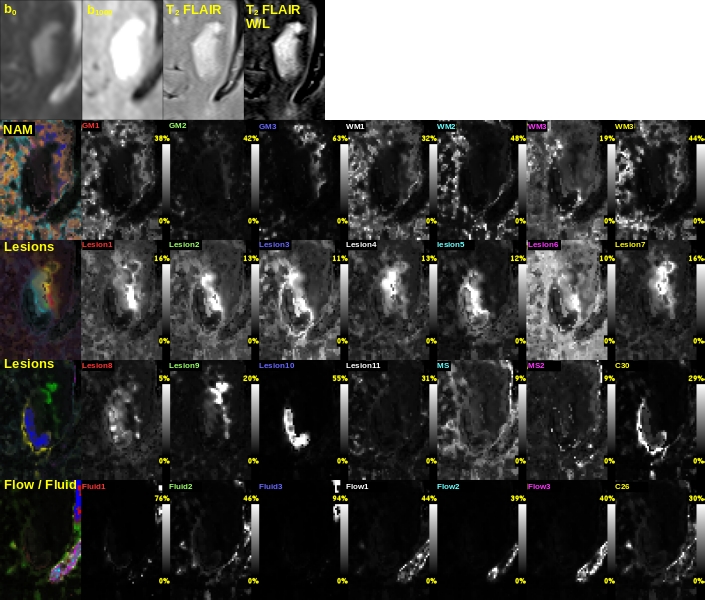
Figure 2: Case 1’s (lesion’s voxels predominately one type) cluster membership maps and related images. First row are the b0 and b1000 DWI, T2 FLAIR standard and lesion enhanced (window & level). Second row is the colorized (comparative intensities) conglomerate NAM and respective individual maps (W&L optimally per map). Third row are the common lesions. Forth row are the less common lesions. Fifth row are the fluid / flow. Note: Lesion 5 and Lesion3 are collocated with DWI-FLAIR mismatch.
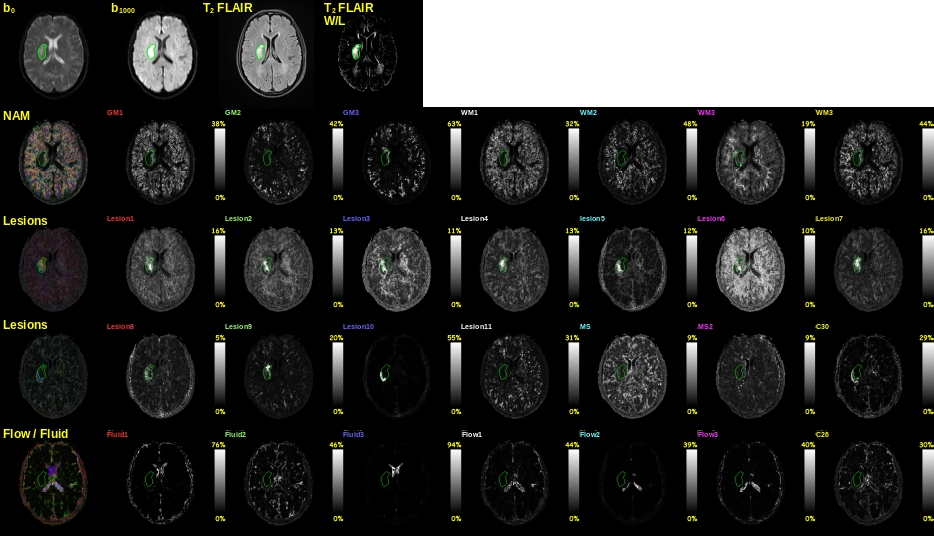
Figure 3: Case 2’s (lesion’s voxels multiple types) cluster membership maps and related images. First row are the b0 and b1000 diffusion weighted images, T2 FLAIR standard and lesion enhanced window & level. Second row is the colorized (comparative intensities) conglomerate NAM and respective individual maps (W&L optimally per map). Third row are the common lesions. Forth row are the less common lesions. Fifth row are the fluid / flow. Lesion 10/C30 are not detectable of T2 or b1000.