0573
Harmonization of Spinal Cord Diffusion Tensor Imaging Data from a Multi-Site, Multi-Scanner Study using Longitudinal ComBat
Devon M Middleton1, Yutong Li2, Andrew Chen3, Russell T Shinohara3, John H Woo3, Adam E Flanders1, Scott H Faro1, Laura Krisa2, and Feroze B Mohamed1
1Radiology, Thomas Jefferson University, Philadelphia, PA, United States, 2Thomas Jefferson University, Philadelphia, PA, United States, 3University of Pennsylvania, Philadelphia, PA, United States
1Radiology, Thomas Jefferson University, Philadelphia, PA, United States, 2Thomas Jefferson University, Philadelphia, PA, United States, 3University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Keywords: Spinal Cord, Diffusion Tensor Imaging
This study uses longitudinal ComBat data harmonization on a multi-site/multi-scanner spinal cord DTI study with a traveling cohort imaged on four scanners. The results show considerable improvement in correlation between scanners as well as decerased coefficient of variation. This approach has potential benefits for large, multi-site spinal cord studies.Introduction
Diffusion tensor imaging (DTI) of the spinal cord has increased considerably over the past decade and continues to show promise as a source of biomarkers for injury and pathology. A major confound, as in brain studies, is the difficulty in comparing DTI metrics acquired from different sites and scanners due to scanner effects: variations in hardware, acquisition schemes, and sequence capabilities. Data harmonization, the process of remove the effects of these variations, has been explored in the brain in attempts to make more comparable data from different studies. In this work, the longitudinal ComBat technique1 was employed using a set of multi-site, multi-scanner spinal cord DTI data to examine whether these scanner effects can be reduced via data harmonization.Methods
DTI data was acquired from 30 healthy volunteer subjects, age range 20-30 years in a previous study2. Subjects were scanned on four different scanners to collect DTI data for the entire cervical and thoracic spinal cord (C1-T12). Two 1.5T scanners were used (Philips Achieva, Siemens Avanto) and two 3T (Philips Ingenia, Siemens Prisma). Sequence parameters including TE, TR, and cardiac gating varied between the acquisitions due to scanner hardware capabilities. Reduced-FOV imaging was used for all scanners except the 1.5T Avanto. Full and reduced FOV data were acquired on the 1.5T Achieva, resulting in 5 DTI acquisitions for each subject. Average values for FA, MD, AD, and RD at each vertebral level were used as inputs for the longComBat model. Age and sex were included as covariates. The resulting harmonized results for FA, MD, AD, and RD were examined for correlation and variability pre-and post-harmonization.Results
Considerable reduction in variability and improvement in correlation was found with the harmonized data. Average values by level for FA, MD, AD, and RD all showed greater consistency in averaged values by vertebral level between scanners (Figure 1). Substantial decreases in coefficient of variation (CoV) for all vertebral levels was achieved where percentage decreases in CoV were: FA = 64%, MD = 59%, AD = 51%, RD = 66%. Correlation measures demonstrated large improvements as well. All DTI metrics showed higher Pearson r values between all scanners post-harmonization (Figure 2).Discussion
The use of longComBat showed substantive improvement in agreement of DTI metrics for all scanners. Prior to harmonization, considerable variability was seen, particularly in diffusivity metrics. Besides offsets of the mean values, different patterns were observed in the upper thoracic region, some scanners showing increases, and some decreases. This is likely due to cardiac pulsation's varying effects on sequences with different TR and gating. The longComBat technique was effective in mitigating this and other scanner effects in diffusivity measures as can be seen in Figure 1. FA, being a normalized metric, exhibited better agreement in the original data compared with diffusivity, but still benefited from harmonization as it saw decrease in CoV comparable with diffusivity metrics. The post-harmonization correlation matrix for FA (Figure 2) shows excellent agreement between scanners with the possible exception of the Achieva 1.5T full FOV.As quantitative spinal cord imaging, including DTI, grows in popularity, the need to combine data from multiple sites into meaningful results becomes increasingly important. Work has been performed to suggest standardization techniques for DTI and other quantitative acquisitions3 and harmonization approaches such as longComBat may serve as an important compliment in taking steps to collect and analyze large, heterogeneous datatsets in quantitative spinal cord imaging.
Conclusion
The use of longComBat harmonization in multi-site/multi-scanner DTI data for a single cohort scanned multiple times was effective in reducing variability and increasing correlation between DTI metrics obtained from MR scanners of differing field strengths and manufacturers. This approach may be beneficial to studies employing multiple sites or longitudinal studies in spinal cord DTI.Acknowledgements
This data used in this work was acquired in a study funded by the Craig H. Nielsen Foundation.References
1. Beer JC, Tustison NJ, Cook PA, Davatzikos C, Sheline YI, Shinohara RT, Linn KA; Alzheimer’s Disease Neuroimaging Initiative. Longitudinal ComBat: A method for harmonizing longitudinal multi-scanner imaging data. Neuroimage. 2020 Oct 15;220:117129.
2. Middleton DM, Fisher J, Flanders AE, Mohamed FB, Woo, JH, Elliot M, Faro SH, Krisa L;A Multi-site/multi-scanner DTI study of the adult spinal cord. ISMRM 2019. Paris, France.
Figures
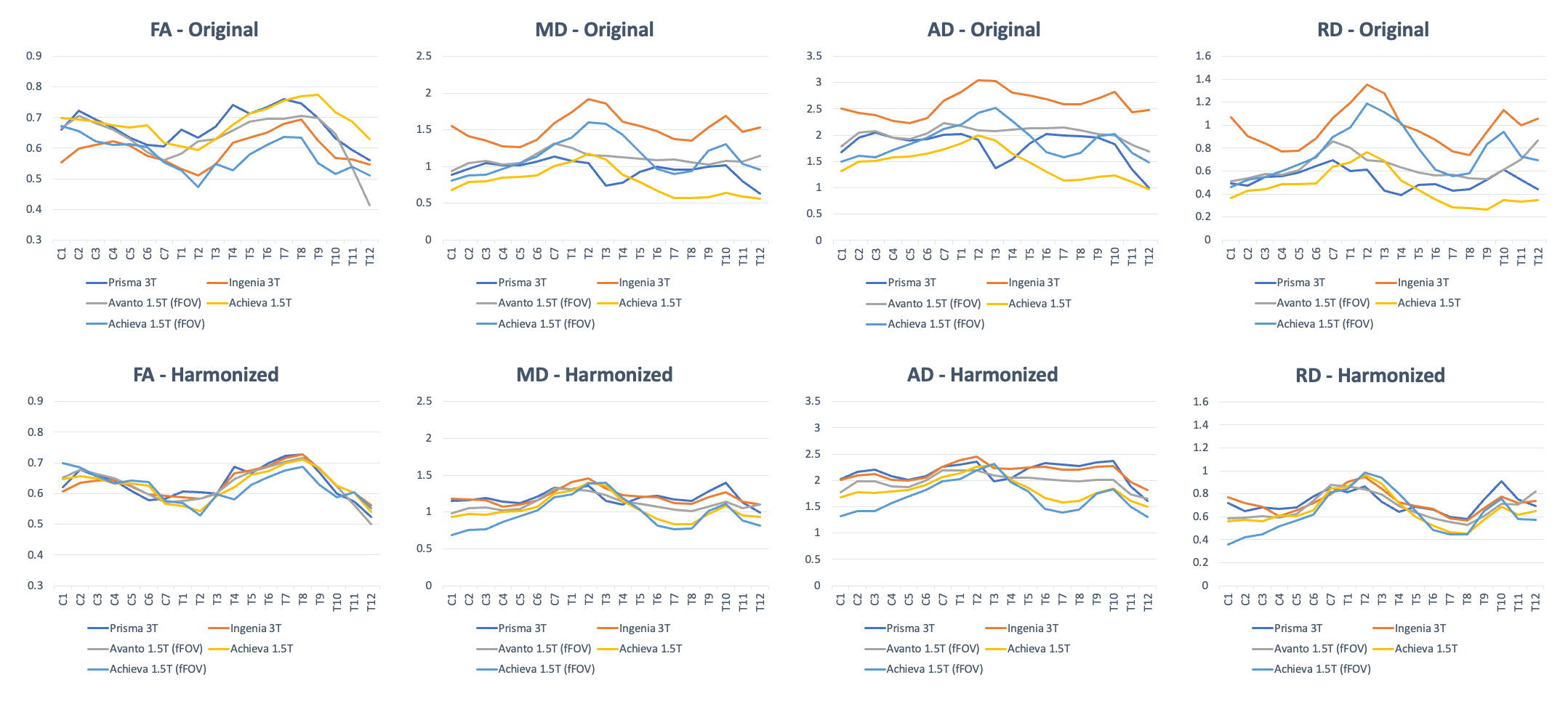
Original and harmonized DTI metrics for FA, MD, AD, and RD. Values are averaged by vertebral level for each scanner.
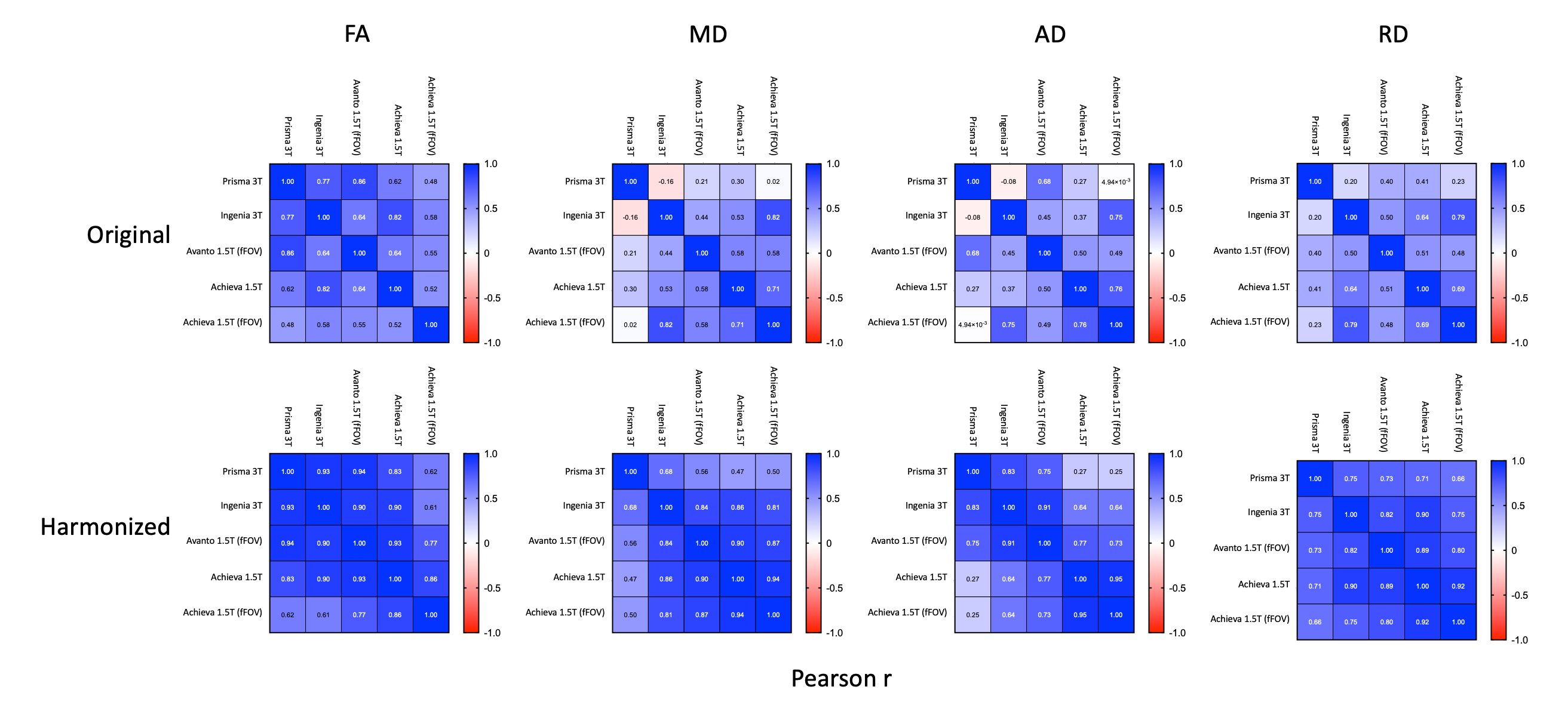
Correlation matrices showing Pearson r values for original and harmonized DTI metrics FA, MD, AD, and RD.
DOI: https://doi.org/10.58530/2023/0573