0558
Fully ungated, free-breathing, 3D T2* mapping for imaging hemorrhagic Myocardial Infarction
Xingmin Guan1, Hsin-Jung Yang2, Jane Sykes3, Xinheng Zhang1, Richard Tang1, Anthony Christodoulou2, Behzad Sharif1, Debiao Li2, Frank S Prato3, and Rohan Dharmakumar1
1Indiana University School of Medicine, Indianapolis, IN, United States, 2Cedars-Sinai Medical Center, Los Angeles, CA, United States, 3Lawson Health Research Institute, London, ON, Canada
1Indiana University School of Medicine, Indianapolis, IN, United States, 2Cedars-Sinai Medical Center, Los Angeles, CA, United States, 3Lawson Health Research Institute, London, ON, Canada
Synopsis
Keywords: Image Reconstruction, Cardiovascular, T2*
T2* CMR is widely used for detecting hemorrhagic myocardial infarction (MI). However, the conventional T2* CMR (2D breath-held, ECG-gated, multi-gradient-echo T2*) can suffer from limited spatial resolution and motion artifacts. We have recently developed a time-efficient, fully ungated, free breathing, 3D T2* mapping approach using a low-rank tensor (LRT) framework to address the above issues.Background
T2* cardiac MRI is the gold-standard for assessment of myocardial iron overload such as intramyocardial hemorrhage (IMH). However, the conventional 2D breath-held, ECG-gated, multi-gradient-echo T2* images can suffer from motion artifacts from unsuccessful breath holding or irregular heart rate which is very common in patients with heart diseases, and limited resolution due to signal-to-noise ratio (SNR) and scan time trade-off within one breath-hold. We developed a time-efficient, fully ungated, free breathing, 3D high-resolution T2* mapping approach using a low-rank tensor (LRT) framework1 to address the above issues. In the LRT framework, the correlation between the shape of the heart and its dynamics over time is exploited in a multi-dimensional cardiovascular image, which substantially reduces redundant information enabling increased efficiency, permitting continuous motion-resolved, free-breathing, non-ECG-triggered 3D acquisition. And as a benefit of 3D acquisition, the LRT method has enabled a desirable imaging resolution at 3T. In this study we investigated the capability of our 3D T2* mapping approach for detecting and characterizing hemorrhagic MI.Methods
The proposed LRT approach was built using the previously described low-rank tensor framework1,2.Hemorrhagic MIs were created in canines (n=5) by 3 hours of LAD occlusion, followed by reperfusion. CMR scans were performed 3 to 5 days after reperfusion in acute phase of MI. Short-axis, conventional 2D and proposed 3D (resolution-matched and two-fold higher resolution) T2*-weighted images, followed by LGE images were acquired in a clinical 3T CMR system. Whole heart acquisition times for conventional 2D, proposed 3D matched resolution and 2-fold higher resolution were approximately 10min, 5min and 10min, respectively. T2* maps were constructed using non-linear least-squares approach as previously described2. Spatial resolution of conventional (2D) and resolution-matched 3D T2*-weighted images were: 1.6x1.6x6 mm3; and higher-resolution T2*-weighted images were acquired with 1.6x1.6x3 mm3. All images were acquired with 8 echoes from 1.41ms to 15.44 ms. Subsequently, hearts were explanted for validation and ex-vivo images were acquired at an isotropic spatial resolution of 1.0 mm. Intramyocardial hemorrhage (IMH) extent was determined based on mean-2SD criteria and represented as %LV volume.
Results
Figure 1 shows representative conventional 2D, proposed 3D with matched and 2-fold higher-resolution T2* images, along with LGE image for reference. Image scoring performed by two experts on 1 to 5 scale (1 – poor; and 5 - excellent), showed the following: 3.5 ± 0.5 (conventional 2D), which was lower than that observed with proposed 3D approach with matched spatial resolution (3.8 ± 0.3, p<0.05). The highest image quality scores were found with 2-fold higher-resolution 3D T2* with a score of 3.9 ± 0.5 (p<0.05). Results of IMH extent measured from different imaging approaches, along with regression analysis, are shown in Figure. 2. Sensitivity and specificity determined using the ex-vivo T2* scans as the ground truth are shown in Figure. 3. Area-under-the-curves from ROC analysis were: 0.67 (conventional 2D); 0.76 (3D LRT) and high-resolution 3D LRT (0.79).Our findings show that the proposed 3D LRT T2* mapping can provide better image quality than conventional 2D T2* imaging. The lower image quality on conventional 2D T2* images were due to motion artifacts from unsuccessful breath-holding and ECG-gating. By using 3D acquisition, LRT approach was able to overcome the limitations for higher resolution acquisition in 2D breath-held cardiac MR imaging. Better image quality scores were given to 2-fold high-resolution 3D LRT T2* images because of better delineation of endo- and epicardium as a benefit of higher imaging resolution and the mitigated intra-voxel dephasing due to susceptibility. The ROC and AUC results indicated that the proposed 3D LRT T2* imaging method had better diagnostic capability in terms of intramyocardial detection comparing to conventional 2D T2* imaging method due to better image quality and higher resolution.
Conclusion
In conclusion, the proposed 3D T2* mapping can provide much needed improvement in image quality of conventional 2D T2* CMR used for hemorrhage detection without the need for breath holding or cardiac gating, both of which are known problems in acute MI patients. Further studies are needed to directly evaluate the benefits of the proposed approach in clinical setting.Acknowledgements
No acknowledgement found.References
1. Christodoulou, A.G., et al., Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging. Nature biomedical engineering, 2018.
2. Guan, X., et al., Fully Ungated 3D Cardiac T2* MR Mapping using a Low-Rank Tensor Framework. ISMRM Abstract, 2022
Figures
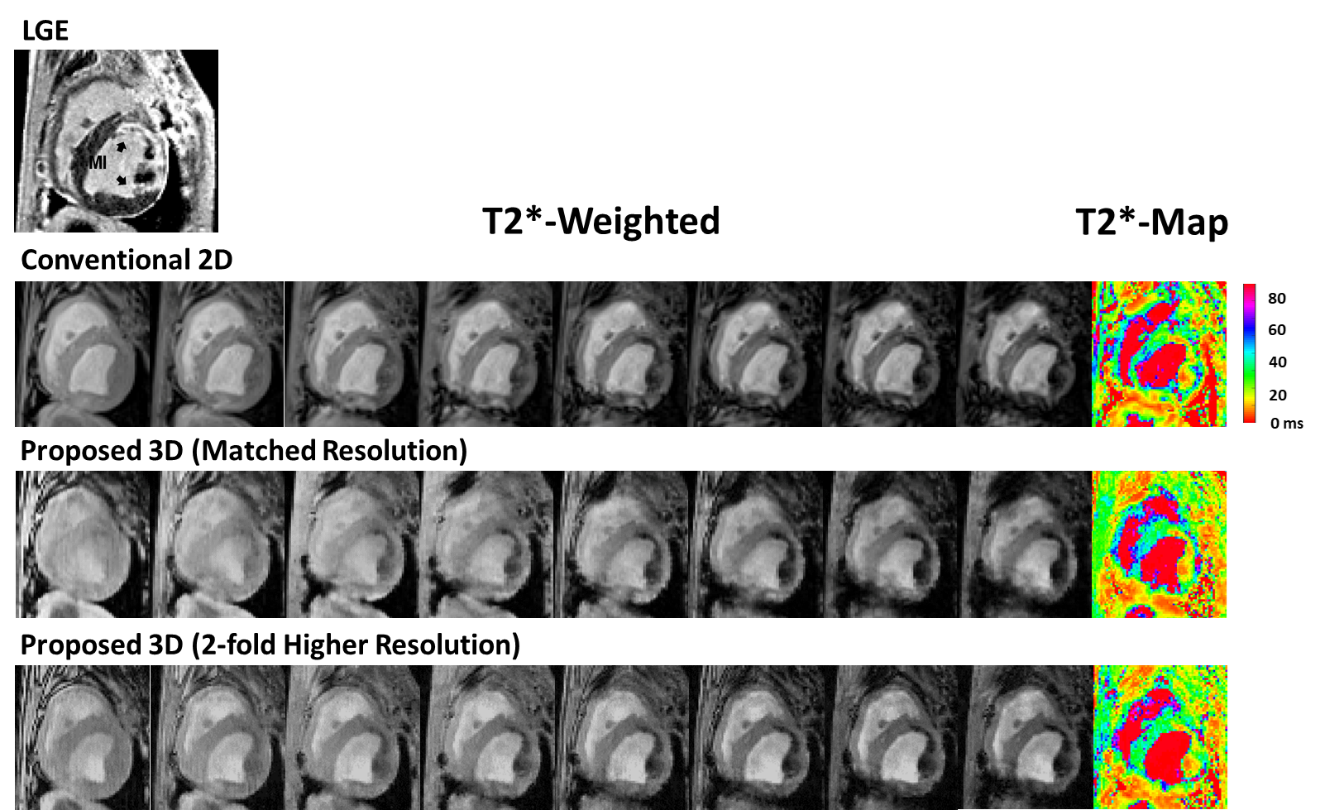
Figure 1. Representative Examples: Multi-echo
T2*-weighted images and T2*-maps from conventional 2D, proposed 3D
LRT with matched and 2-fold higher resolution CMR. Slice-matched LGE image is
displayed on top for reference.
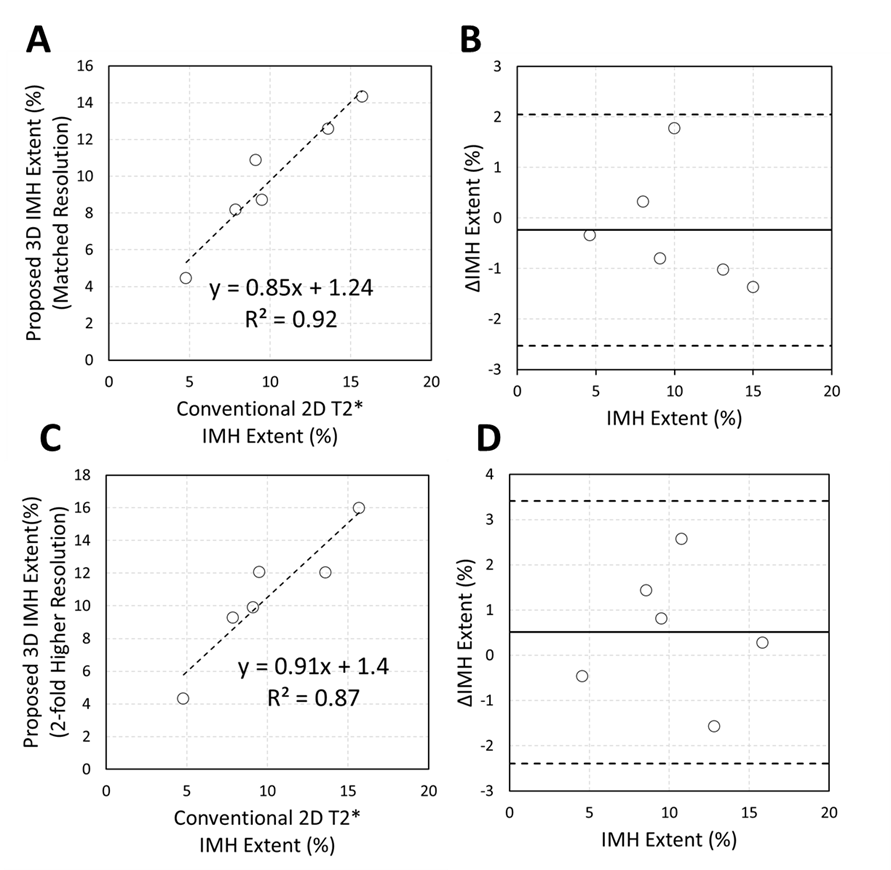
Figure 2. Comparison of IMH Extent
Extracted from 2D, and Proposed 3D T2*.
A. Relation between IMH Extent measured
from conventional 2D T2* and proposed 3D LRT T2* at matched imaging resolution: y = 0.85x
+ 1.24, R2 = 0.92, p<0.05. B. Bland-Altman analysis of
data in (A) shows that the mean bias between the two approaches is -0.24 ± 1.15
%. C. Relation between IMH Extent
measured from conventional 2D T2* and proposed 3D LRT T2* at higher imaging resolution: y = 0.91x
+ 1.4, R2 = 0.87, p<0.05. D. Bland-Altman analysis of data
in (C) shows that the mean bias between the two approaches is 0.51 ± 1.45 %.
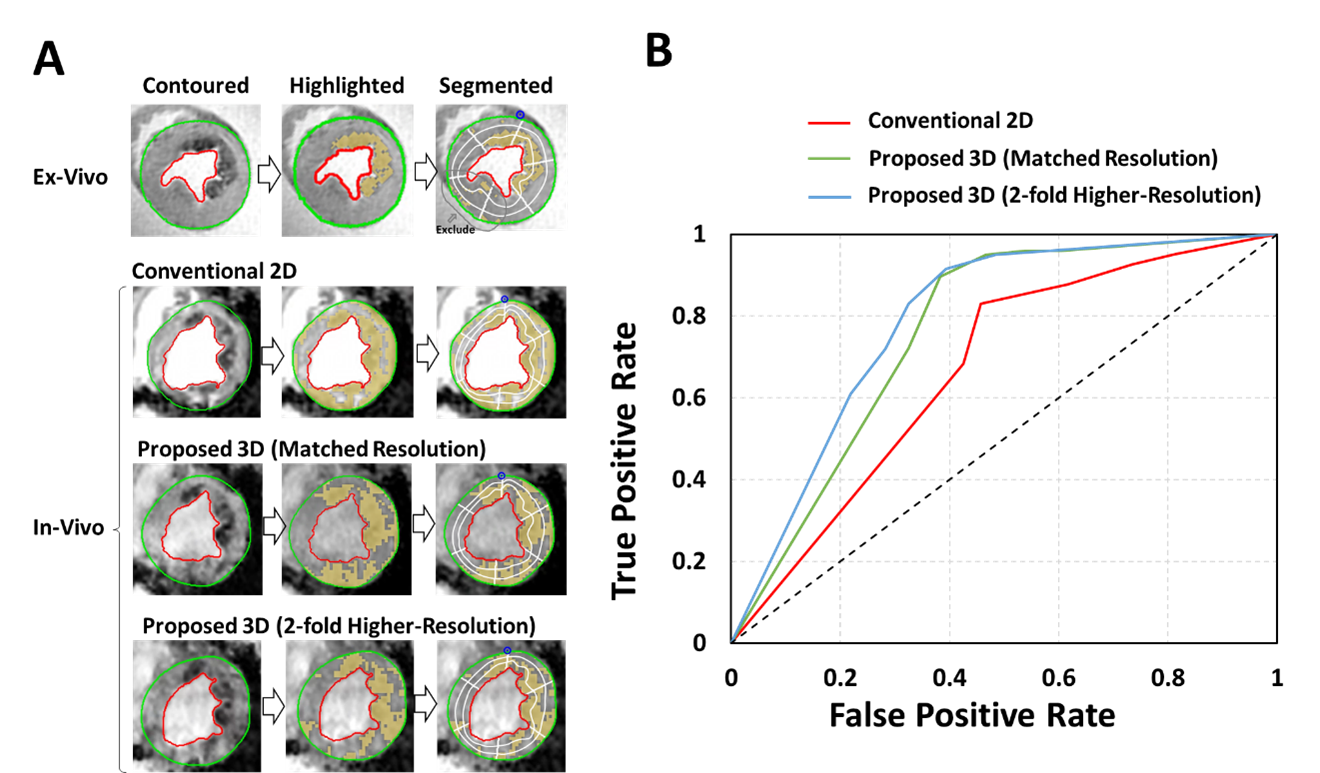
Figure
3. Diagnostic Accuracy of IMH Detection by Conventional 2D, Proposed 3D LRT-based
T2*. A. Ex-vivo and in-vivo contoured T2* images (first column), highlighted to identify hemorrhagic
infarction territory (second column), that are
segmented and further divided into endo-, mid- and epi-cardial
segments are shown. Sensitivity and
specificity of all in-vivo imaging approach for detection of IMH were analyzed
using ex-vivo T2* images as ground
truth. B. ROC curves of IMH detection by conventional 2D, proposed
3D with matched and 2-fold higher-resolution are shown.
DOI: https://doi.org/10.58530/2023/0558