0556
Free-running 5D whole-heart MRI with ferumoxytol enhancement to evaluate cardiac function in congenital heart disease1Radiology department, University of Lyon, Lyon, France, 2CIBM, CHUV, Lausanne, Switzerland, 3CIBM, CHUV, Lausanne, France, 4Research radiology department, Hospices Civiles de Lyon, Lyon, France, 5Cardiology, CHUV, Lausanne, Switzerland, 6Pediatric cardiology department, CHUV, Lausanne, France
Synopsis
Keywords: Cardiomyopathy, Data Analysis, cardiac function
Free-running 5D whole-heart imaging (5D CMR) has been proposed as a means of simplifying CMR exams by capturing the entire 3D cardiac anatomy without the need for ECG gating or breath-holds. We demonstrated that 5D CMR with ferumoxytol enhancement enables the evaluation of cardiac function in comparison to ECG gated 2D CINE images in congenital heart disease patients. In addition, it enables evaluation of the cardiac morphology with improved diagnostic quality in ~40% of the cases. This suggests that the free-running approach has the potential for replacing the conventional 2D imaging for evaluation of both cardiac function and morphology.Background
Cardiac magnetic resonance imaging (CMR) plays a critical role in the management of patients with congenital heart disease (CHD)(1,2). In a conventional CMR exam, electrocardiogram (ECG) gated 2D CINE images (2D CMR) are the current gold standard for assessing cardiac function, but require a reliable ECG signal, precise prescription of multiple imaging planes, and patient ability to perform breath-holds. Recently, free-running 5D whole-heart imaging (5D CMR) has been proposed for simplifying CMR exams by capturing the entire 3D cardiac anatomy without the need for ECG gating or breath-holds (3,4). In this work, and using a gold standard comparison, we demonstrate the feasibility and validity of using ferumoxytol-enhanced 5D CMR to evaluate cardiac function in a cohort of patients with CHD.Methods.
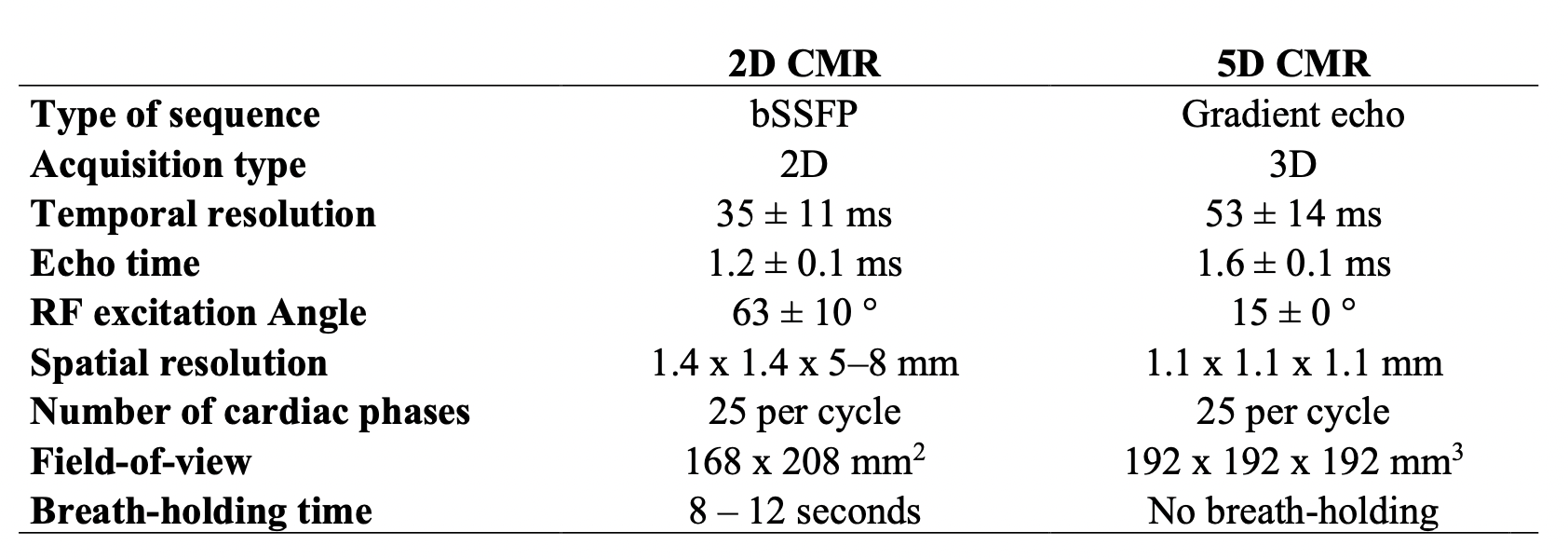
Seventeen CHD patients (22±15-years of age, 7 female (41%)) were retrospectively included in this monocentric study, after approval by the IRB. All patients underwent both 2D CMR and a research 5D sequence after an injection of 2 mg/kg of ferumoxytol (3,4) on a 1.5T clinical MR scanner (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany) with a 18-channel phased-array coil. Relevant scan parameters for both sequences are listed in Table 1. A cardiac radiologist with 7 years of experience reformatted the end-inspiratory images from 5D CMR to match the respiratory phase, orientation and slice thickness of 2D CMR. Two readers without experience of 5D CMR (R1: a radiologist and R2: research engineer with 7 and 9 years of experience in cardiac imaging, respectively) blinded to the patient’s identity and condition, independently performed the measurement of end-diastolic and end-systolic cardiac volumes (EDV, ESV) in a random order on a clinical workstation using Circle software (cvi42 5.12.1). Inter- and intrareader reproducibility were assessed with the intraclass correlation coefficient (ICC). A two-way model with measures of consistency was used to calculate ICC values. Reproducibility was defined as poor (ICC<0.400), fair to good (ICC=0.400–0.750), or excellent (ICC>0.750). Two-sided P .05 was considered to indicate a significant difference. Diagnostic image quality was assessed and compared according to a five-point quality scale ranging from 1= insufficient due to blurring and/or breathing motion and/or insufficient contrast, to 5= excellent without blurring or breathing motion and with excellent contrast.Results.
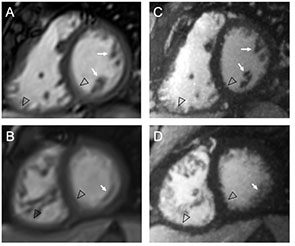
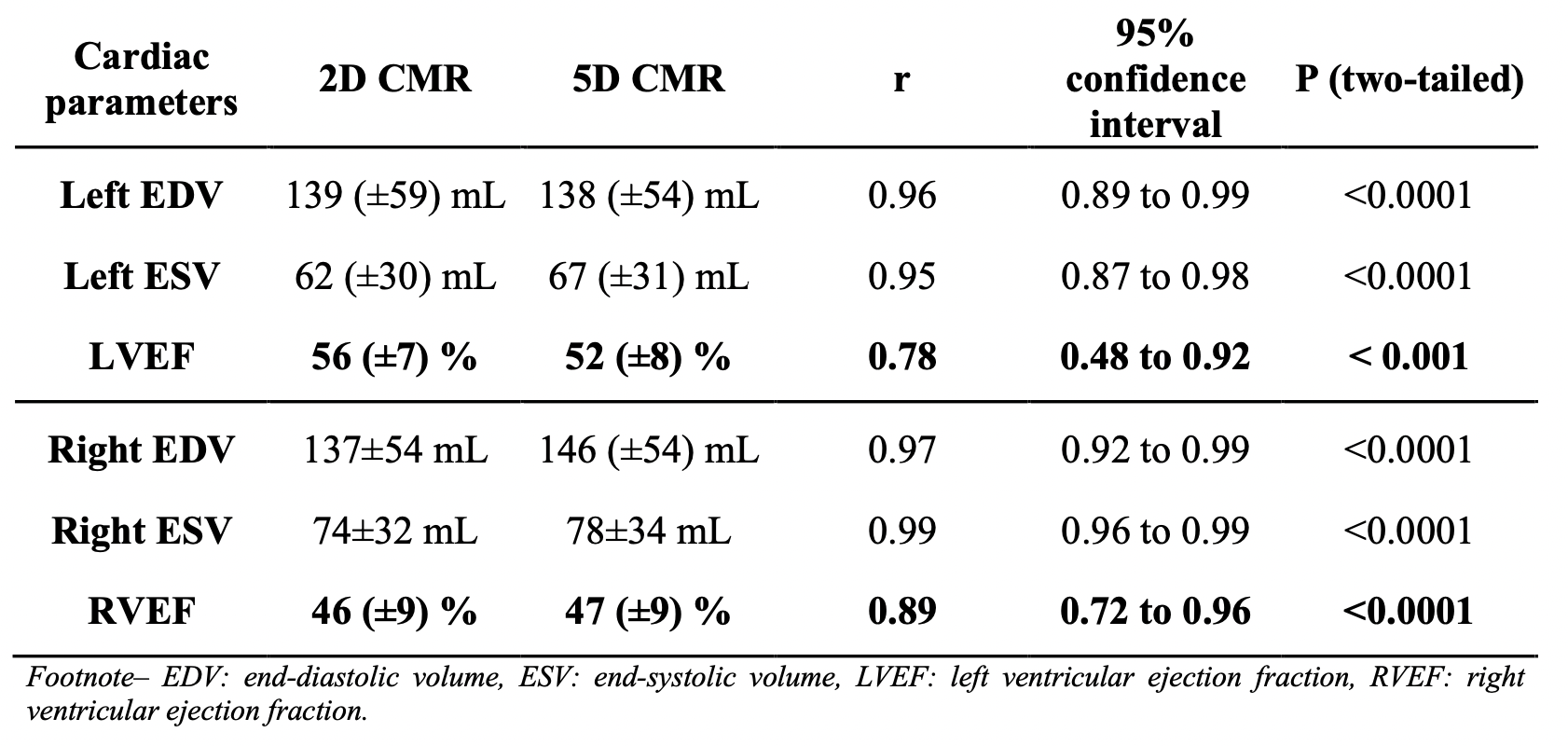
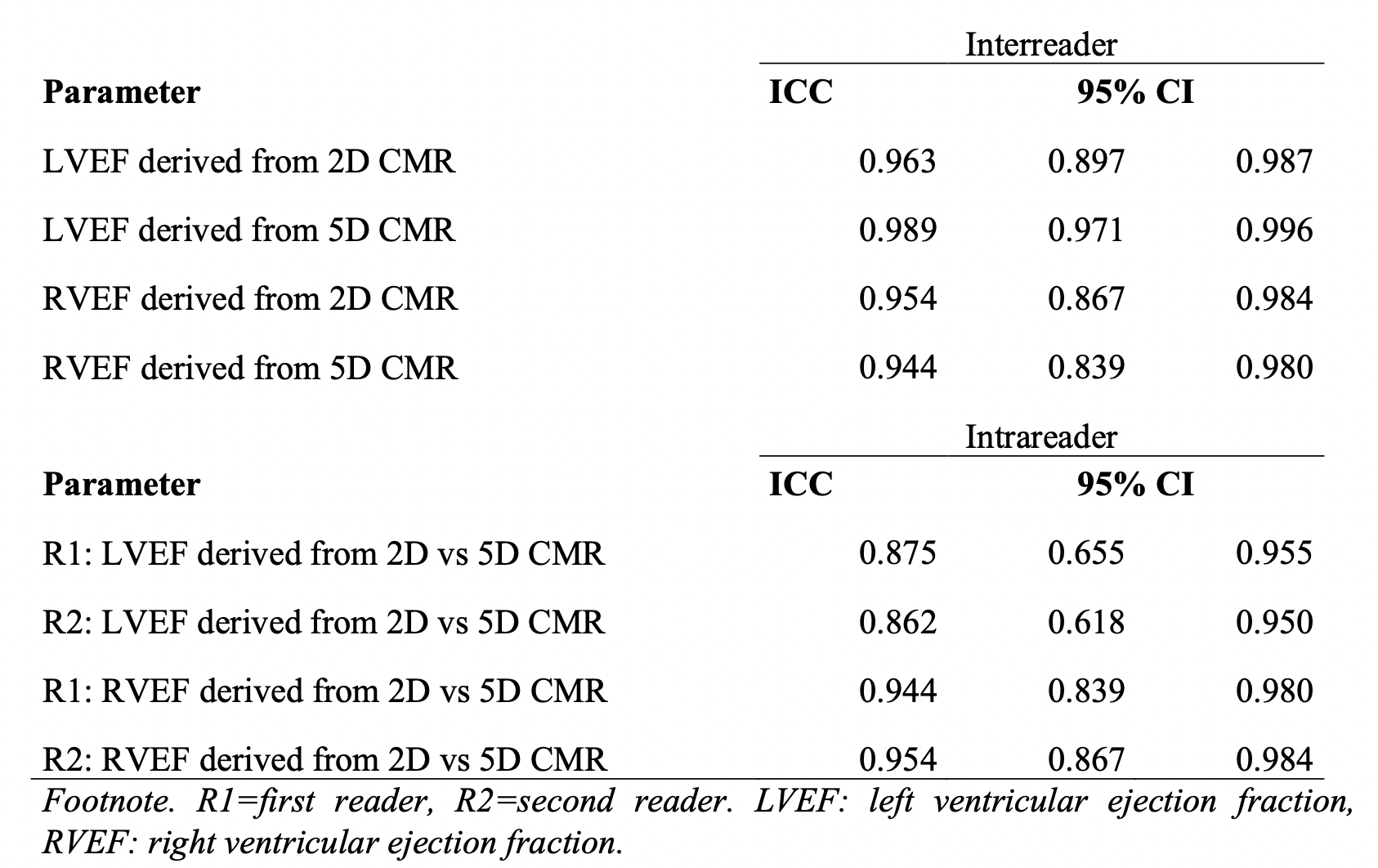
All patients were successfully analyzed. Time of acquisition of 5D CMR was significantly reduced by 58±101 seconds in comparison to 2D CMR (5.8±0 min vs 6.8±1.7 min, P<0.02). Absolute mean differences among both readers in left EDV, ESV and LVEF for 5D CMR relative to 2D CMR were 0.6±14.8 mL, 5.8±9.1 mL and 3.6±5.0%. Absolute mean differences among both readers in right EDV, ESV and LVEF for 5D CMR relative to 2D CMR were 9.9±13.7 mL, 7.1±7.8 mL and 0.1±4.2 %, respectively. Almost perfect correlation between left and right cardiac volumes and volume ejection fraction was observed (all r>0.87) (Table 2). Interreader agreement was excellent for all ejection fraction measures on both 2D and 5D CMR images (all ICC >0.940) with a highest value for LVEF on 5D CMR images (0.989) (Table 3). Similarly, intrareader agreement for both readers was excellent for all ejection fraction measures between 2D and 5D CMR images (all ICC>0.862) with highest values for RVEF (0.944 and 0.954 for R1 and R2, respectively). Diagnostic quality was improved in 35% and 41% of the cases on 5D CMR images for R1 (mean score: 4.4±0.6 vs 4.0±0.8) and R2 (mean score: 4.2±0.5 vs 3.7±0.7), respectively to be found from good to excellent in 94% of the cases (compared to 65% on 2D images) (Figure 1).Discussion and Conclusion
In the present study, we demonstrated in a population of CHD patients the feasibility of using ferumoxytol-enhanced 5D CMR to evaluate both right and left cardiac functions with higher spatial resolution, faster time of acquisition and similar temporal resolution than CINE 2D CMR but without the need for ECG gating or breath-holds. Our results showed an excellent intrareader agreement of the LVEF and RVEF between 5D and 2D CMR images. The average difference between EF was close to 0% for the right ventricle and slightly higher at 3.6% for the left ventricle. A larger difference for LVEF may be explained by a more difficult delineation of the left cavity in comparison to the right one particularly during systole because of thicker wall and trabeculations of the left myocardium. This anatomical particularity probably explains also the larger difference found for the left ESV compared to EDV between 5D and 2D CMR images. In addition, while our results showed an excellent interreader agreement of LVEF on 5D and 2D CMR images, 5D CMR images showed a higher agreement. This finding is probably explained by the improved diagnostic quality using 5D CMR, such as found in ~40% of the cases due to higher spatial resolution, lower motion artefact and higher contrast. However, 5D and 2D CMR are not based on the same sequence which would introduce a difference in cavity contrast and may explain the difference in diagnostic quality score. Nevertheless, this suggests that 5D CMR could reduce the operator dependency of cardiac function analysis while outperforming its feasibility, time of acquisition, convenience and diagnostic quality.Acknowledgements
No acknowledgement found.References
1. Dorfman AL., Geva T., Samyn MM., et al. SCMR expert consensus statement for cardiovascular magnetic resonance of acquired and non-structural pediatric heart disease. J Cardiovasc Magn Reson 2022;24(1):44. Doi: 10.1186/s12968-022-00873-1.
2. Fratz S., Chung T., Greil GF., et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson 2013;15(1):51. Doi: 10.1186/1532-429X-15-51.
3. Roy CW., Di Sopra L., Whitehead KK., et al. Free-running cardiac and respiratory motion-resolved 5D whole-heart coronary cardiovascular magnetic resonance angiography in pediatric cardiac patients using ferumoxytol. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson 2022;24(1):39. Doi: 10.1186/s12968-022-00871-3.
4. Di Sopra L., Piccini D., Coppo S., Stuber M., Yerly J. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. Magn Reson Med 2019;82(6):2118–32. Doi: 10.1002/mrm.27898.
Figures