0512
Accelerated 3D MR cholangiopancreatography using a deep learning-based reconstruction in patients with cholelithiasis1West China Hospital of Sichuan University, Chengdu, China, 2Clinical Science, Philips Healthcare, Chengdu, China
Synopsis
Keywords: Liver, Biliary
In this work, we aimed to compare image quality and lesion detectability in patients suspected with gallstones among single breath-hold three-dimensional magnetic resonance cholangiopancreatography (MRCP) with gradient and spin-echo (GRASE) technique, with compressed sensing (CS) and with deep learning (DL) technique. DL MRCP showed the best image quality and better lesion conspicuity and lesion edge sharpness.Synopsis
In this work, we aimed to compare image quality and lesion detectability in patients suspected with gallstones among single breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography (MRCP) with gradient and spin-echo (GRASE) technique, with compressed sensing (CS) and with deep learning (DL) technique.Introduction
Cholelithiasis a very common condition (∼10–20% of the global adult population) and is associated with high socioeconomic costs[1]. 3D MRCP is a noninvasive imaging technique to evaluated with the biliary tree. MRI accelerated imaging techniques have been applied to 3D MRCP to enable imaging in a single breath-hold, including the 3D GRASE technique[2, 3] and 3D CS technique[4, 5]. Recently, the DL–based image reconstruction has been introduced to 3D MRCP promising higher acceleration factors while simultaneously increasing SNR[6]. Sometimes the reduction in noise could bring about a reduction in image detail and decrease in diagnostic performance. It is necessary to evaluate the diagnostic efficacy of accelerated techniques. The purpose of this study is to compared the imaging quality and diagnostic confidence among GRASE, CS and DL in patients suspected with cholelithiasis.Methods
This study was approved by the local IRB. Fifty-three patients suspected with cholelithiasis were examined on a 3.0T system (Ingenia Elition, Philips Healthcare) with a 16-element phased-array coil. The MRCP sequences were scanned in a random order. The imaging parameters were shown as following:(1) 3D GRASE: TR/TE = 235/93 ms, field of view(FOV) = 300x300x100 mm2, voxel size = 0.59×0.59×1 mm3, NSA = 1, acquisition time (TA) = 13 s; (2) 3D CS: TR/TE = 1800/390 ms, FOV = 300×300×100 mm2, voxel size = 0.59×0.59×1 mm3, NSA = 1, CS acceleration factor = 24, TA = 13 s; (3)AI-CS: TR/TE = 1800/385 ms, FOV = 300×300×100 mm2, voxel size = 0.59×0.59×1 mm3, NSA = 1, CS acceleration factor = 24, TA= 13 s. Two radiologists independently and blindly evaluated image quality and lesion detectability using the 5-grade scoring (5= excellent, 4 = good, 3 = moderate, 2 = poor, 1 = nondiagnostic). The image quality included the following parts: overall image quality, artifacts, background suppression and duct visualization of common bile duct, right hepatic duct, anterior branch, posterior branch, left hepatic duct, medial branch, lateral branch, pancreatic duct. The lesion detectability included lesion conspicuity and lesion edge sharpness.Results
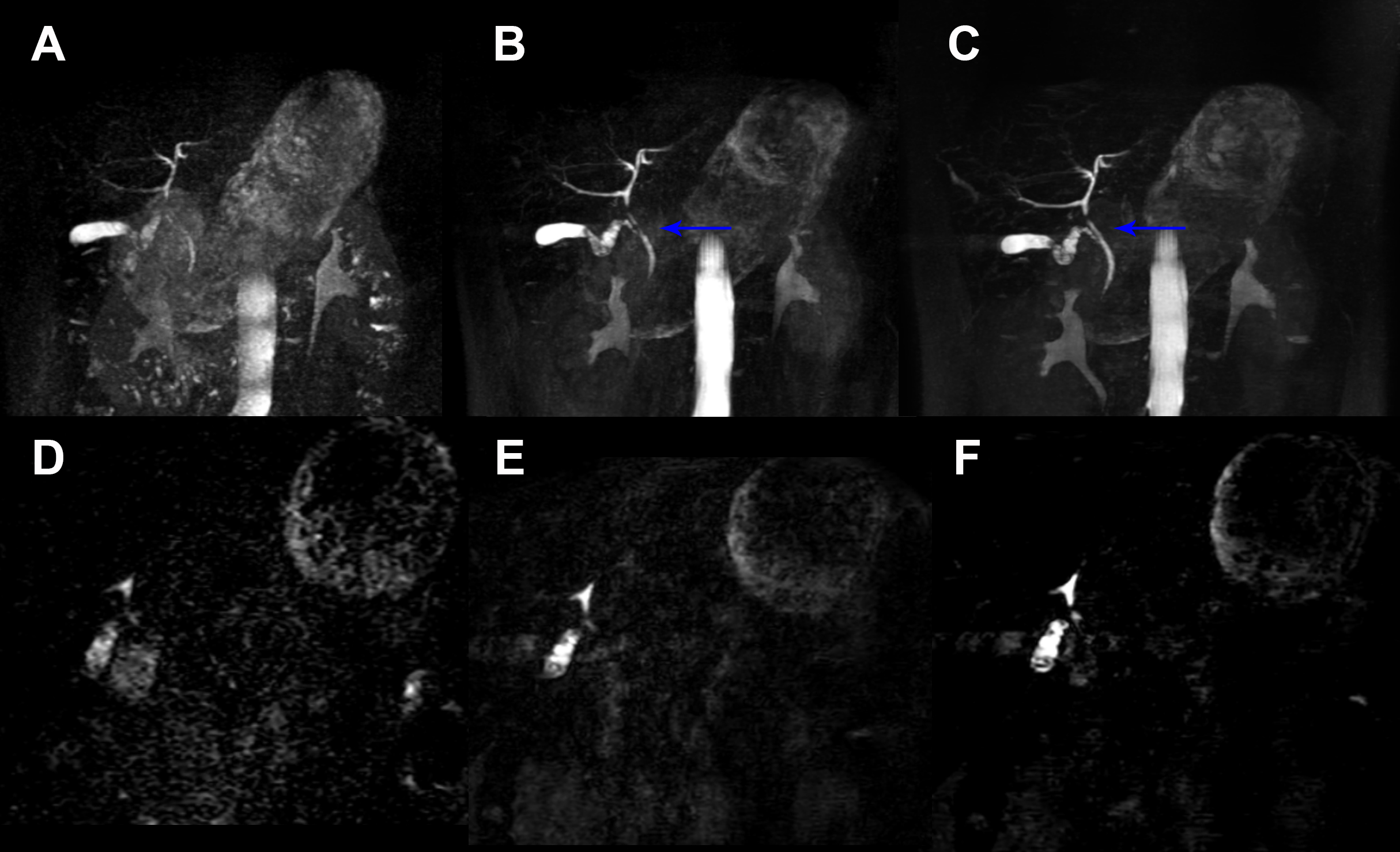
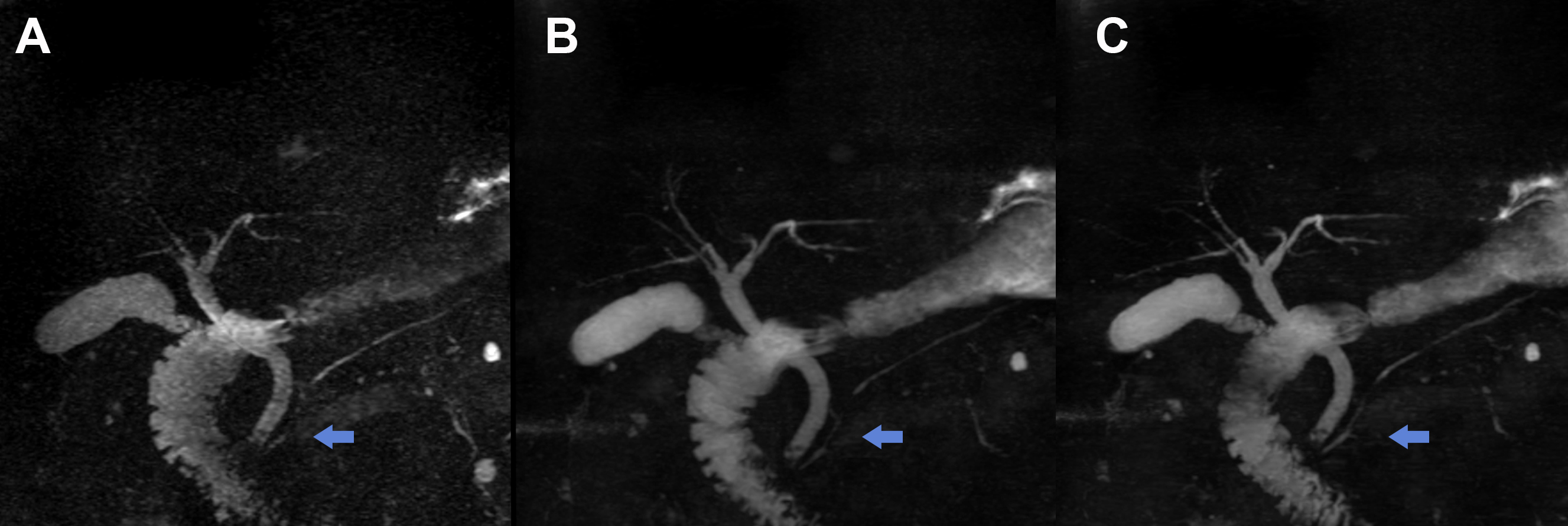
DL sequence received significantly higher scores than GRASE for overall image quality (3.83 ± 0.64 vs 3.40 ± 0.69), duct visualization of common bile duct (3.83 ± 0.75 vs 3.30 ± 0.70), right hepatic duct (3.58 ± 1.08 vs 3.04 ± 1.02), anterior branch (3.38 ± 1.09 vs 2.68 ± 1.24), posterior branch (3.39 ± 1.10 vs 2.68 ± 1.19), left hepatic duct (3.74 ± 0.98 vs 3.26 ± 0.94), medial branch (3.15 ± 1.17 vs 2.25 ± 1.24), lateral branch (3.53 ± 0.97 vs 2.74 ± 1.15), pancreatic duct (2.68 ± 1.25 vs 2.23 ± 1.20)(all p < 0.05). Compared with CS, DL also demonstrated better duct visualization in anterior branch (3.38 ± 1.09 vs 3.11 ± 1.10) and posterior branch (3.39 ± 1.10 vs 3.13 ± 1.19) of the right hepatic duct and medial branch (3.15 ± 1.17 vs 3.05 ± 1.18) and lateral branch (3.53 ± 0.97 vs 3.26 ± 1.06) of the left hepatic duct (all p < 0.05).Lesion conspicuity was rated good to excellent in all 3 sequences with higher scores for DL (4.60 ± 0.77) in comparison to CS (4.45 ± 0.87) and GRASE (4.02 ± 1.35, p < 0.05) (Figure 1). Lesion edge sharpness was higher scores for DL (4.63 ± 0.87) in comparison to CS (4.42 ± 0.66) and GRASE (3.99 ± 1.17, p < 0.05) (Figure 2). Two radiologists showed good to perfect interobserver consistency (0.77 - 0.92).
Discussion and Conclusion
DL reconstruction provides better duct visualization, especially small hepatic duct visualization than GRASE and CS. And DL shows a significant higher lesion conspicuity and lesion edge sharpness compared GRASE in patients suspected with cholelithiasis. DL allows to do the fast acquisition and maintain well image quality.Acknowledgements
No acknowledgement found.References
1. Lammert F, Gurusamy K, Ko CW, et al (2016) Gallstones. Nat Rev Dis Prim 2:. https://doi.org/10.1038/nrdp.2016.24
2. Yoshida M, Nakaura T, Inoue T, et al (2018) Magnetic resonance cholangiopancreatography with GRASE sequence at 3.0T: Does it improve image quality and acquisition time as compared with 3D TSE? Eur Radiol 28:2436–2443. https://doi.org/10.1007/s00330-017-5240-y
3. Nam JG, Lee JM, Kang HJ, et al (2018) GRASE Revisited: breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography using a Gradient and Spin Echo (GRASE) technique at 3T. Eur Radiol 28:3721–3728. https://doi.org/10.1007/s00330-017-5275-0
4. Yoen H, Lee JM, Lee SM, et al (2021) Comparisons between image quality and diagnostic performance of 2D- and breath-hold 3D magnetic resonance cholangiopancreatography at 3T. Eur Radiol. https://doi.org/10.1007/s00330-021-07968-w
5. Chen Z, Sun B, Xue Y, et al (2021) Comparing compressed sensing breath-hold 3D MR cholangiopancreatography with two parallel imaging MRCP strategies in main pancreatic duct and common bile duct. Eur J Radiol 142:109833. https://doi.org/10.1016/j.ejrad.2021.109833
6. Pezzotti N, Yousefi S, Elmahdy MS, et al (2020) An adaptive intelligence algorithm for undersampled knee MRI reconstruction. IEEE Access 8:204825–204838. https://doi.org/10.1109/ACCESS.2020.3034287
Figures