0509
Synthetic phase-sensitive inversion-recovery imaging for assessing extramural venous invasion in patients with rectal cancer1Affiliated Hospital of Jiangnan University, Wuxi, China, 2GE Healthcare, Shanghai, China, 3Department of Radiology,Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, Xiangyang, China
Synopsis
Keywords: Pelvis, Quantitative Imaging, synthetic MR, rectal cancer, vessels
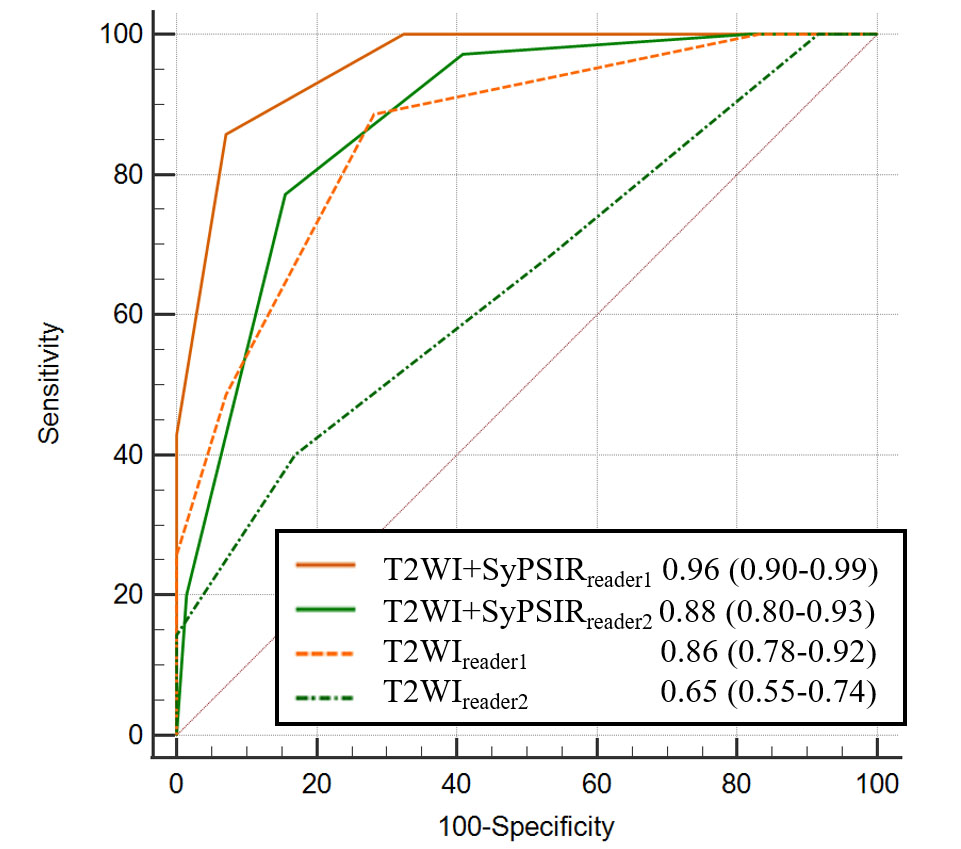
This study aimed to investigate the feasibility of synthetic phase-sensitive inversion recovery (SyPSIR) vessel for extramural venous invasion (EMVI) detection in patients with rectal cancer. One hundred and six histologically confirmed rectal cancer patients (35 EMVI+ and 71 EMVI−) were evaluated. Compared with using T2WI alone, the area under the receiver operating characteristic curve using the combination of T2WI and SyPSIR was increased from 0.86 to 0.96 and from 0.65 to 0.88 for the senior and junior radiologist, respectively. Therefore, SyPSIR can provide additional information to improve EMVI diagnostic efficiency of in rectal cancer.Introduction
Extramural venous invasion (EMVI) is an important factor that leads to poor survival outcomes in rectal cancer [1]. MRI, especially T2-weighted imaging (T2WI), is a valuable method that is widely used for preoperative EMVI assessment [2]. However, the diagnosis is highly dependent on the subjective judgment of radiologists with an accuracy of < 60% to > 80% among different radiologists [3].Phase-sensitive inversion recovery (PSIR) vessel images is a contrast images that reconstructed simultaneously through post-processing of Synthetic MRI. Synthetic PSIR vessel showed a higher area under the receiver operating characteristic (ROC) curve than TOF (time of flight) magnetic resonance angiography (MRA) [4]. Therefore, the PSIR vessel seems particularly promising for the detection of EMVI in rectal cancer and is expected to corroborate and complement conventional T2WI.
This study initially investigated the value of synthetic PSIR vessel in assessing the EMVI status of rectal cancer, and further compared its diagnostic efficacy as an aid to a junior radiologist and a senior radiologist.
Materials and Methods
Patients: This retrospective study was approved by institutional review board and the ethics committee of our hospital. The requirement for informed consent was waived by the institutional review board. Between October 2020 and April 2022, 189 participants with pathologically confirmed rectal cancer, who underwent both conventional and synthetic MRI at our institution, were recruited. The exclusion criteria were pathological stage T1/2N0 (n = 31), radiotherapy or chemotherapy before MRI examination (n = 28), and no surgery in our hospital (n = 24).MRI experiment: All MRI examinations were performed using a 3.0 T scanner (Signa Architect; GE Healthcare, Milwaukee, CA, USA) equipped with a 16-channel phased-array body coil. The scan sequence included T2WI in the sagittal, axial, and coronal positions (3227–5326 ms/102 ms [repetition time ms/echo time ms]; field of view, 24 cm × 24 cm–30 cm × 30 cm; flip angle, 111°; matrix size, 320 × 224; 3 mm/0.3 mm [slice thickness/spacing]; number of sections, 18–28; acquisition time, 2 min 24 s–2 min 35 s) and axial synthetic MRI (two echo times [19.5/97.3 ms] and four saturation delay times [210/610/1810/3810 ms]; FOV, 24 cm × 24 cm; FA, 111°; matrix size, 320 × 224; 3 mm/0.3 mm; number of sections, 18–28; acquisition time, 4 min 32 s). Synthetic MR (v8.0; Linköping, Sweden) was used to process the synthetic images to generate SyPSIR.
Data analysis: MRI EMVI status was assessed using a subjective scoring system developed by Smith et al. [5] (score 0: no vessel in the vicinity of extramural tumor penetration; score 1: vessel with normal caliber and no obvious tumor signal intensity; score 2: slightly expanded vessel with no obvious tumor signal intensity; score 3: intermediate tumor signal intensity inside an expanded vessel; and score 4: evident irregular vessel contour or nodular expansion of the vessel by the tumor signal). A score of 0–2 indicates EMVI−, and a score of 3–4 indicates EMVI+. All statistical analyses were performed in SPSS version 22.0 or MedCalc Statistical Software version 18.2. Chi square test and unpaired t-test were used to compare TN stage, and the length/ thickness of tumors, respectively. Sensitivity, specificity, accuracy, and area under the ROC curve (AUC) were used to compare the diagnostic efficiencies of different sequences. P<0.05 was considered statistical significance.
Results
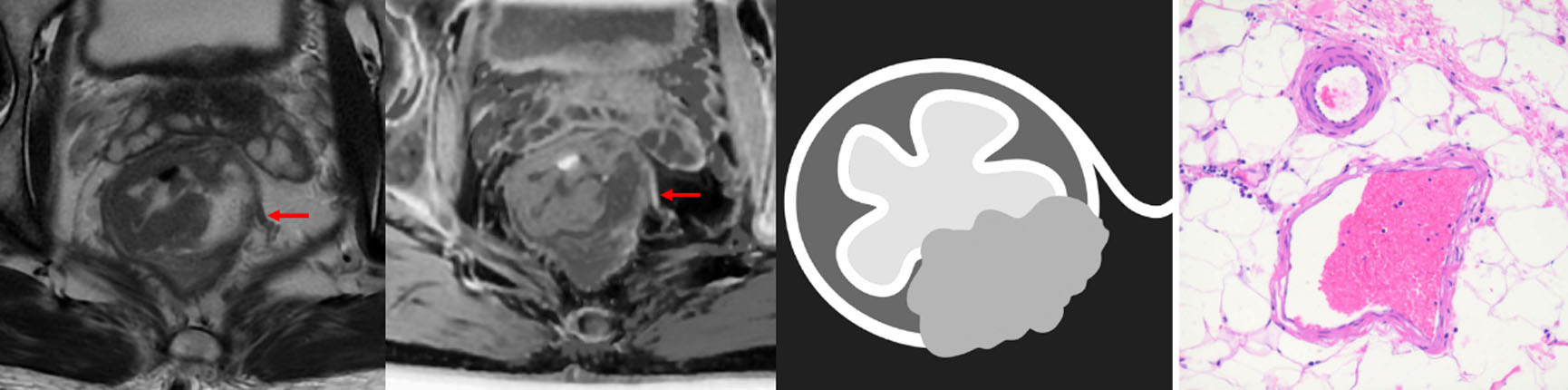
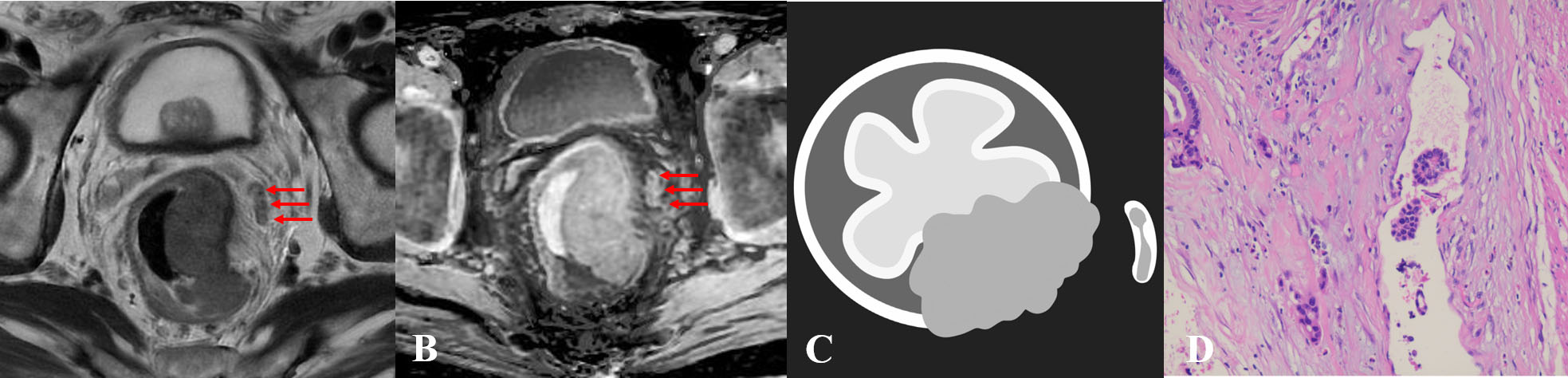
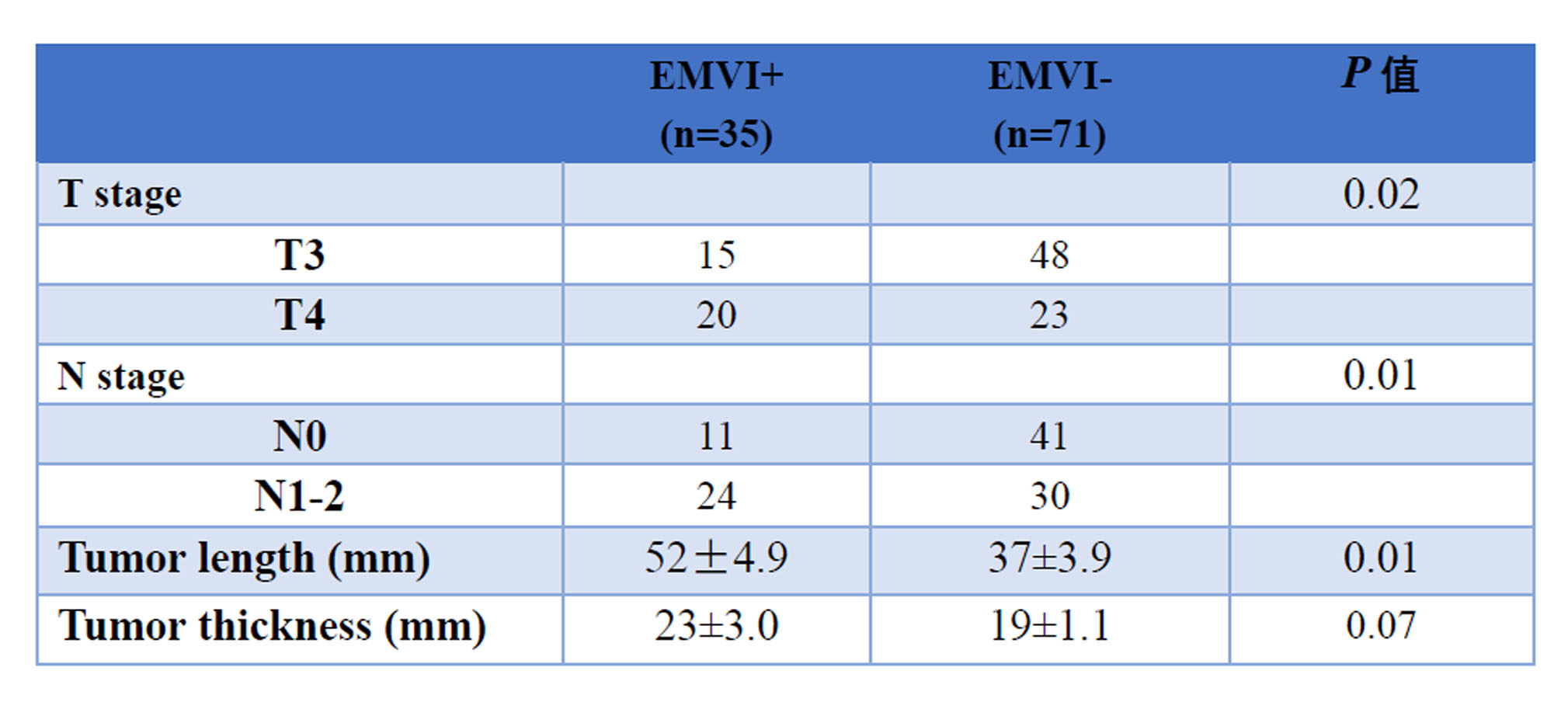
Among the 106 cases, 35 were pathologically confirmed as EMVI+ and 71 as EMVI−. The EMVI+ patients demonstrated significantly higher levels of T and N stages than EMVI– patients (P = 0.02 and 0.01, respectively). The tumor length was significantly longer in EMVI+ than in EMVI– patients (52 ± 4.9 mm and 37 ± 3.9 mm, respectively; P = 0.01). The tumor thickness tended to be thicker in EMVI+ than in EMVI– patients but this not statistically significant (23 ± 3.0 mm and 19 ± 1.1 mm, respectively; P = 0.07) (Table 1).On the SyPSIR, normal vessels demonstrated obvious hyperintensity around the tumor, with a normal diameter or slightly thickened caliber (score 2, Figure 1), but no tumor signal in the vessel running area or intraluminal region. When EMVI occurs, the vessels are partially replaced by tumors and an intermediate tumor signal can be detected inside a high signal and expanded vessel (score 4, Figure 2). Compared with using T2WI alone, the AUC using the combination of T2WI and SyPSIR was increased from 0.86 to 0.96 and from 0.65 to 0.88 for the senior and junior radiologist, respectively.
Discussion and conclusion
This is the first study to investigate the clinical value of SyPSIR for evaluating EMVI in rectal cancer. The SyPSIR provides similar image quality to that of conventional T2WI and achieves high inter-observer consistency in image quality scores and tissue SI. Our data confirms that the SyPSIR provided an added value to T2WI for assessing EMVI, with the diagnostic accuracy of radiologists significantly improving from 69%–78% to 81%–91% by combining T2WI and SyPSIR.In summary, SyPSIR, as a robust and high-quality MRI images, may facilitate preoperative EMVI evaluation of rectal cancer by improving the diagnostic efficacy for radiologists.
Acknowledgements
We thank Ke-wei wang for help with the statistical analysis of the data in this paper. We thank Zi Wang, Xin-yi Zhou and Bo-jian Fei for their contributions to patient treatment data collection. All authors had access to the study data, and reviewed and approved the final manuscript.This study was funded by the Wuxi Science and Technology Development Fund (Grant No. Y20212019).References
1. Benson AB III, Venook AP, Al-Hawary MM et al (2018) Rectal cancer, version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 16:874–901.
2. Jhaveri KS, Hosseini-Nik H, Thipphavong S et al (2016) MRI detection of extramural venous invasion in rectal cancer: correlation with histopathology using elastin stain. AJR Am J Roentgenol 206:747-55.
3. Bae JS, Kim SH, Hur BY et al (2019) Prognostic value of MRI in assessing extramural venous invasion in rectal cancer: multi-readers' diagnostic performance. Eur Radiol 29:4379–4388.
4. Wang Q, Wang G, Sun Q, Sun DH (2021) Application of MAGnetic resonance imaging compilation in acute ischemic stroke. World J Clin Cases 9:10828-10837.5. Smith NJ, Shihab O, Arnaout A, Swift RI, Brown G (2008) MRI for detection of extramural vascular invasion in rectal cancer. AJR Am J Roentgenol 191:1517–1522.
Figures