0463
Comparing self-reporting concussion assessments with an objective Diffusion Tensor Imaging (DTI) and resting state MRI (rsMRI) based measure1Electrical and Computer Engineering, McMaster University, Hamilton, ON, Canada, 2School of Biomedical Engineering, McMaster University, Hamilton, ON, Canada, 3Imaging Research Centre, St. Joseph's Healthcare Hamilton, Hamilton, ON, Canada, 4Radiology, McMaster University, Hamilton, ON, Canada, 5Toronto Rehabilitation Institute, Toronto, ON, Canada, 6Medicine, University of Toronto, Toronto, ON, Canada, 7neurorad.ch, Zurich, Switzerland, 8Radiology & Neuroradiology, University hospital of Schleswig-Holstein, Kiel, Germany
Synopsis
Keywords: Traumatic brain injury, Brain Connectivity, Gray Matter, White Matter
Traditional concussion self-reporting has significant limitations due to its subjectivity and inconsistency, therefore a more objective MRI-based approach is proposed in this research. A concussion population was assessed using the traditional PCSS method versus DTI anisotropy analysis and rsMRI complexity analysis. Concussed patients were compared to large age and sex matched datasets and a Z-transform was used on white and gray matter ROIs to identify injured areas in the cerebrum. A weighted mean equation was then used to compare Z-scores to the 7-point PCSS. Results confirmed sex differences in self reporting and shows promise as a future objective assessment tool.Introduction
Concussions are a common and devastating condition that severely affects over 1.7 million people globally each year1. Unfortunately, patients further suffer from poor diagnostic outcomes as current clinical evaluations are subjective and inconsistent. The goal of this study was to compare the post-concussion symptom scale (PCSS), a routinely used subjective patient self-reporting assessment tool2, against an objective assessment measure based on diffusion tensor imaging (DTI) and resting state MRI (rsMRI) analysis, within a concussion population3.Methods
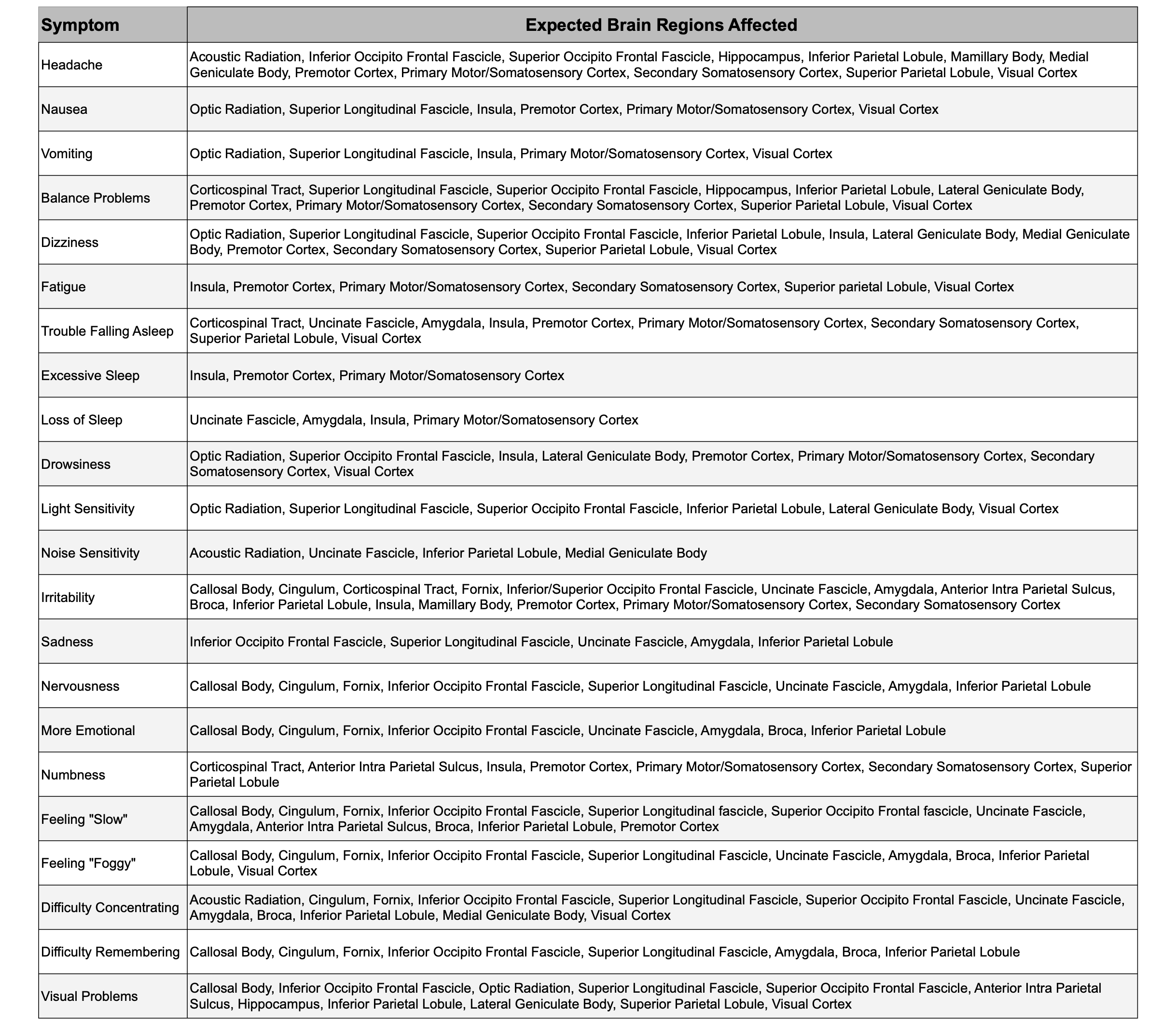
Images were obtained using a GE MR750 Discovery 3T MRI scanner and a 32-channel RF receiver coil (General Electric Healthcare, Milwaukee, WI). Axial DTI was acquired using a dual echo EPI sequence (60 non-coplanar directions, 6 b=0s/mm2 images, TE/TR=87/8800ms, b=1000s/mm2, 122x122 matrix, 2mm thickness, FOV=244mm) while resting state BOLD data was acquired using an EPI sequence (FOV=22cm, 64x64 matrix, TE/TR=35/2000ms, 3mm thickness, and 175 temporal points). 26 patients who suffered a concussion were analysed (10 males (33±12 yrs) and 16 females (38±12 yrs)) where a traditional PCSS test (includes 22 symptoms) was administered prior to the scanning session2. A minimum of 88 DTI and rsMRI dataset pairs of healthy age and sex matched controls (age matched ±2yrs) were collected through the IDA, NITRC, and HCP databases4,5,6 to satisfy the Cochran formula for 95% sensitivity7. Injured and healthy control datasets were warped into the MNI152 space, eddy corrected, and brain extracted and further segmented into common region of interests (ROIs) for DTI (19 white matter ROIs) and rsMRI (91 gray matter ROIs), respectively8,9. A homebuilt python processing pipeline was used to perform routine rank-2 tensor analysis (FA, AD, MD, RD) on DTI data and voxel-wise rsMRI temporal complexity based on the Hurst exponent3,10,11,12,13. Statistical map distributions for each healthy control population DTI and rsMRI dataset pairs were created and verified through skewness and kurtosis tests which enabled the application of a Z-score approach to identify subject-specific abnormal ROIs in the concussion patient3. The Z-score magnitudes were then classified into a severity metric on a 6-point scale in order to be compared to the 6-point scaled PCSS2. A synthetic MRI-based assessment score was then calculated using a weighted sum mean of the abnormally identified ROI Z-scores for each patient, given DTI and rsMRI Z-score magnitudes. A synthetic assessment score was also calculated for each symptom corroborating the ROIs function and associated pathology (i.e. optic radiation pathology is associated with the symptom of visual problems), (see Figure 1). The weighted mean equation can be explained by $$MRIScore=\frac{1}{2}\left(\frac{\sum(x_i*w_i)}{\sum(w_i)}+\frac{\sum(y_i*w_i)}{\sum(w_i)}{}^{} \right)$$ where the MRIScore represents the rounded MRI-Based symptom score, x, represents the actual Z-score of an abnormal DTI ROI, w, represents the weights of the Z-score, and y, represents the actual Z-score of an abnormal fMRI ROI. Total PCSS scores (i.e. the sum of scores) that were self-reported where then compared to the MRI-Based method (i.e. synthetic scores). Overall accuracy was evaluated with age and sex effects where concussion patients were divided into younger (under 35 yrs) or older (over 35 yrs), and male or female respectively.Results
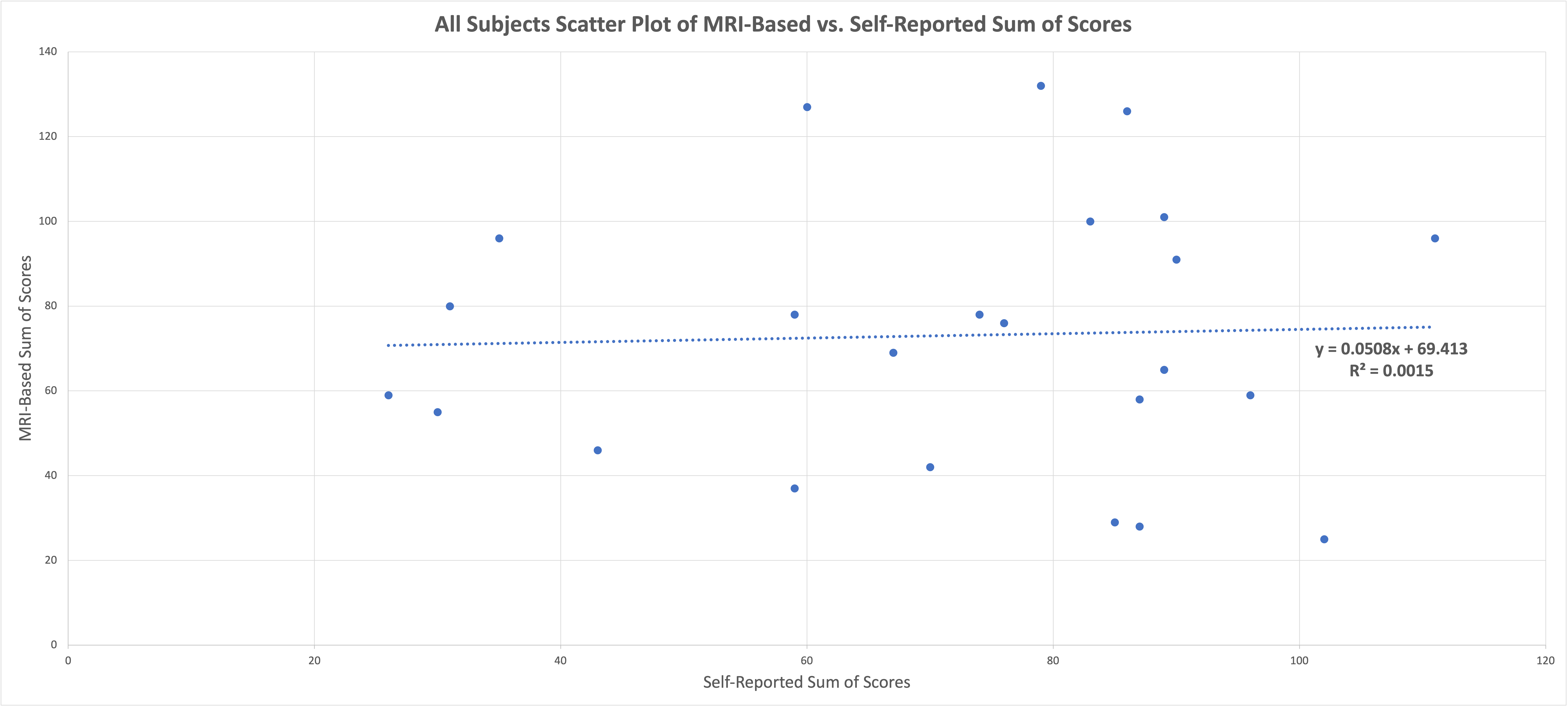
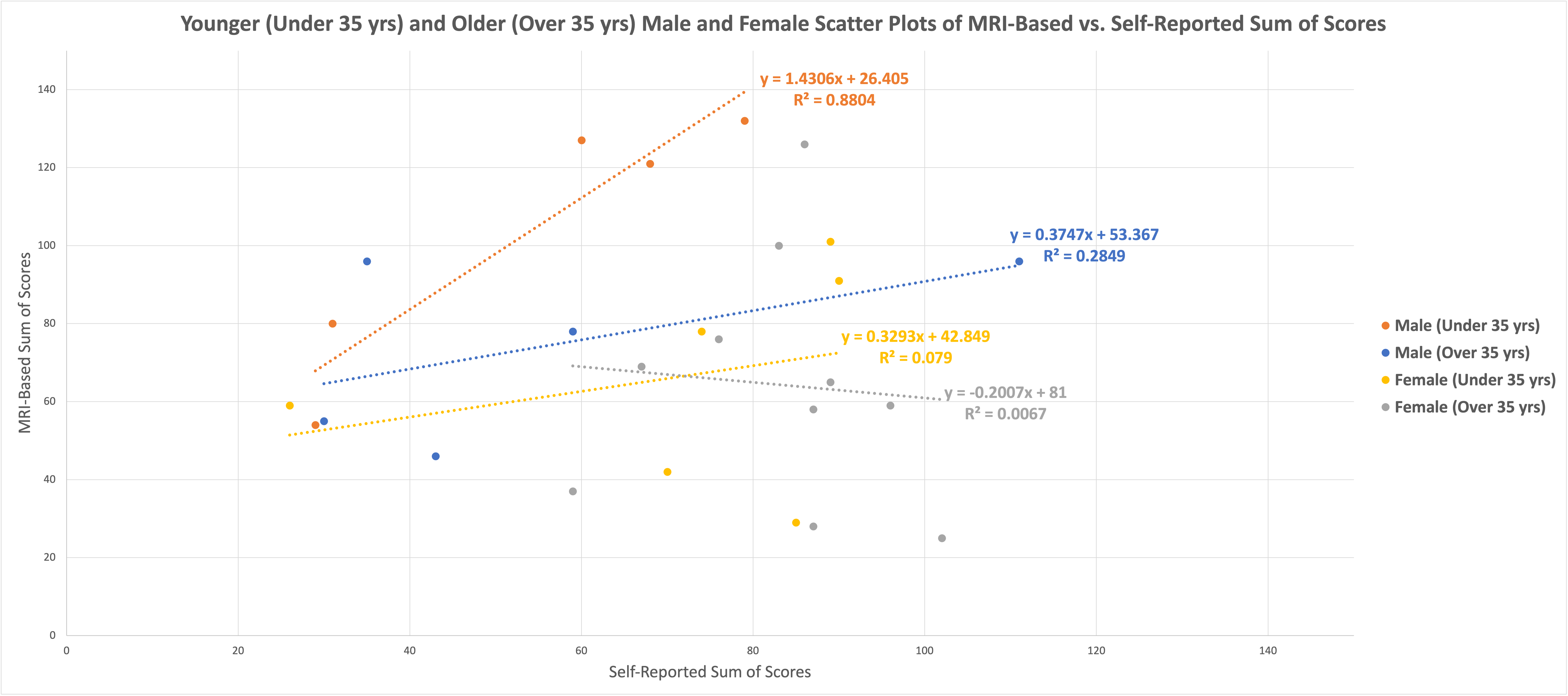
Each concussion patient self-reported symptoms using the PCSS and each had at least one DTI or rsMRI abnormality based on our MRI-based objective analysis. For each patient, there was a 15% accuracy in terms of symptom matching the self-reported PCSS with the MRI-based calculated scores. Given that the PCSS is highly subjective and inconsistent, exact symptom matching is notoriously difficult. When assessing the sum of scores (self-reported vs. MRI-based), overall, no trends were found (see Figure 2). However, the evaluation of age and sex yielded some interesting trends where young men (under 35 yrs) tended to underreport concussion symptoms (i.e. lower self-reported scores than the MRI-based scores) whereas older women (over 35 yrs) tend to overreport their symptoms (i.e. higher self-reported scores than MRI-based scores) (see Figure 3). This trend corroborates with traditional literature that outlines younger men, in professional athletic settings, tend to underreport their symptoms14,15.Conclusions
The MRI-based approach proposed shows tremendous promise as a future tool to assess concussion patients and their symptoms more objectively. Future work must be performed to identify how self-reporting and MRI-based findings change in a longitudinal fashion in these patients. Our results confirm that sex differences play a significant role in self-reporting and that cultural effects most likely also confound self-reporting results. Together, these factors clearly indicate why objective measures for concussion must be investigated.Acknowledgements
Special thanks to my supervisors and mentors Dr. Michael D. Noseworthy, Dr. Dinesh Kumbhare, Dt. Stephan Ulmer, and Norm Konyer for their abilities and guidance. More thanks to my fellow Brain Trust colleagues Ethan Danielli, Ethan Samson, Neil MacPhee, Bhanu Sharma, Mahnaz Tajik, Lauren Anderson, Calvin Zhu, and Yves Pauli. Thank you for the financial support from McMaster University, the National Sciences and Engineering Research Council of Canada (NSERC), and the MITACS Accelerate program. Lastly, thank you to my beautiful wife, my family, and friends who have tremendously supported me along the way.References
- Voss JD, Connolly J, Schwab KA, Scher AI. Update on the epidemiology of concussion/mild traumatic brain injury. Current pain and headache reports. 2015 Jul;19(7):1-8.
2. Lovell MR, Collins MW. Neuropsychological assessment of the college football player. The Journal of head trauma rehabilitation. 1998 Apr 1;13(2):9-26.
3. Danielli E, Simard N, Sharma B, Doughty M, Noseworthy MD. Functional, but minimal microstructural brain changes present in aging Canadian football league players years after retirement. Brain Disorders. 2022 Jun 1;6:100036.
4. Crawford KL, Neu SC, Toga AW. The image and data archive at the laboratory of neuro imaging. Neuroimage. 2016 Jan 1;124:1080-3.
5. Kennedy DN, Haselgrove C, Riehl J, Preuss N, Buccigrossi R. The NITRC image repository. NeuroImage. 2016 Jan 1;124:1069-73.
6. Van Essen DC, Smith SM, Barch DM, Behrens TE, Yacoub E, Ugurbil K, Wu-Minn HCP Consortium. The WU-Minn human connectome project: an overview. Neuroimage. 2013 Oct 15;80:62-79.
7. Cochran WG. Sampling techniques. John Wiley & Sons; 1977.
8. Bürgel U, Schormann T, Schleicher A, Zilles K. Mapping of histologically identified long fiber tracts in human cerebral hemispheres to the MRI volume of a reference brain: position and spatial variability of the optic radiation. Neuroimage. 1999 Nov 1;10(5):489-99.
9. Bürgel U, Amunts K, Hoemke L, Mohlberg H, Gilsbach JM, Zilles K. White matter fiber tracts of the human brain: three-dimensional mapping at microscopic resolution, topography and intersubject variability. Neuroimage. 2006 Feb 15;29(4):1092-105.
10. TE JM, Woolrich MW, Smith SM. Fsl. Neuroimage. 2012;62(2):782-90.
11. Dona O, Noseworthy MD, DeMatteo C, Connolly JF. Fractal analysis of brain blood oxygenation level dependent (BOLD) signals from children with mild traumatic brain injury (mTBI). PLoS One. 2017 Jan 10;12(1):e0169647.
12. Eke A, Herman P, Bassingthwaighte J, Raymond G, Percival D, Cannon M, Balla I, Ikrényi C. Physiological time series: distinguishing fractal noises from motions. Pflügers Archiv. 2000 Feb;439(4):403-15.
13. Eke A, Herman P, Kocsis L, Kozak LR. Fractal characterization of complexity in temporal physiological signals. Physiological measurement. 2002 Jan 28;23(1):R1.
14. Halstead ME, Walter KD, Council on Sports Medicine and Fitness. Sport-related concussion in children and adolescents. Pediatrics. 2010 Sep;126(3):597-615.
15. Dick RW. Is there a gender difference in concussion incidence and outcomes?. British journal of sports medicine. 2009 May 1;43(Suppl 1):i46-50.
Figures